
Abstract
Hospital mergers have increased significantly since 2010, driven by factors such as healthcare policy changes, reimbursement, economies of scale, and quality improvement goals. However, limited evidence exists about how these mergers affect the quality of care and cancer outcomes. We conducted a difference-in-differences analysis to assess the impact of hospital consolidation on cancer outcomes. Using data from the Surveillance, Epidemiology, and End Results (SEER) program, we identified cancer patients diagnosed between 2008 and 2016, then used the Health Cost Institute’s Healthy Marketplace Index to assess hospital consolidation as measured by the Herfindahl–Hirschman Index (HHI). The HHI is a measure of market concentration and competition between firms in a given industry. We found that increases in hospital consolidation were associated with a higher likelihood of early-stage cancer diagnosis compared to control areas (−1.1%, 95% confidence interval (CI) −2.3 to 0.0%), and improved overall survival (hazard ratio 0.94, CI 0.90-0.98). These improvements were restricted to cancers with screening recommendations. Our study suggests that hospital consolidation may have some benefits for cancer patients. However, these benefits may not be evenly distributed across all cancer types. Further research is needed to confirm these findings and to understand the mechanisms by which hospital consolidation affects cancer outcomes.
Introduction
Hospital consolidation has been increasing significantly in the 21st century, with data from 2017 showing that 66% of all hospitals were found within a larger network, compared to only 53% in 2005. 1 Consolidation reduces marketplace competition and limits patient choices and leads to higher prices. 2 While consolidation can improve efficiency through economies of scale, it may also introduce bureaucratic inefficiencies. Larger consolidated organizations comprise of multiple layers of management which may stagger communication and force delays between conception and implementation of quality improvement practices.1,2
Existing evidence of the impact of hospital mergers on quality of care is limited. A few studies on specific hospital system acquisitions have shown a potential improvement in quality of care depending on regional characteristics by a reduction in rate of infection and higher patient satisfaction, 3 or a modest reduction in overall mortality.3,4 However, most recent evidence suggests that reduced hospital market competition has led to higher patient costs and increased readmissions.3,5-7
Hospital consolidation has been associated with higher healthcare prices, with post-merger increases ranging from 2% to 40%.3-6 This is attributed to increased market power and negotiation leverage with health insurers. 8 Prior studies have indicated that reduced competition resulting from hospital consolidation leads to poorer patient outcomes.3,4,6-12 However, specific hospital system acquisitions have shown regional-dependent improvements in care quality or modest reductions in overall mortality.3,11 Understanding how hospital consolidation affects disease-specific care is lacking.
Our study investigates the impact of hospital consolidation on cancer outcomes including early-stage cancer identification, cancer-specific quality outcomes, and overall survival after cancer diagnosis. Using the Surveillance, Epidemiology, and End Results (SEER) dataset, we analyzed cancer patients in selected regions of the United States, linking changes in regional hospital market concentration to temporal changes in cancer outcomes.
Methods
Data Source
We conducted a retrospective observational study by identifying cancer patients in the SEER database diagnosed between 2008 and 2016. This period reflects the accelerated pace of consolidation since 2010. 12 We categorized them based on whether they lived in areas with significant increase in hospital market concentration or control areas. We conducted a multivariable difference-in-differences (DID) regression analysis to compare changes in cancer outcomes before and after the areas experienced high hospital marketplace consolidation. The degree of hospital market consolidation was measured using the Herfindahl–Hirschman Index (HHI), 13 which measures market concentration ranging from 0 to 10 000 with higher values indicating greater concentration. This value is calculated by squaring the market share of each firm operating in each market and summing the resulting values. 13 Mathematically, the HHI can be expressed as:

According to the US Department of Justice guidelines, markets with an HHI above 2500 are considered highly concentrated, 1500 to 2500 are moderately concentrated, while markets with an HHI below 1500 are unconcentrated. 14 When hospitals merge or acquire other hospitals, the HHI value for that market will increase, indicating a decrease in competition. We obtained HHI data from the Health Cost Institute report of Healthy Marketplace Index (HMI). Data is available on the SEER database (seer.cancer.gov) and our grouped raw data will be made available to any qualified researcher upon request.
Study Groups
We classified areas based on HHI values and changes over time as either the experimental group with high increases in consolidation or the control group with no significant change in consolidation. We adhered to U.S. Department of Justice and the Federal Trade Commission’s guidelines for classifying mergers.13,14 Inclusion criteria allowed only MSAs which would be classified as high concern, those which requires change in HHI >200, and final HHI >2500 (highly concentrated). Control group inclusion was derived from the same report and defined as change in HHI <200 and final HHI <2500 (unconcentrated or moderately concentrated). The exclusion criteria included the following: patients who did not live in a county within an MSA, if the entire MSA is not accounted for in the data, if HHI data was not available for the county in which that patient lived, or if the MSA did not meet the criteria for either the experimental or control group (Supplemental Figure 1). The study protocol utilized only publicly available data and the institutional review board of Wayne State University deemed this study exempt. All patient data in the SEER database was anonymized.
Outcomes
We categorized cancer types as screened, partial screening recommendations, and unscreened based on US Preventive Services Taskforce (USPSTF) recommendations for cancer screening during the entirety of the study duration. 15 Cancers with a USPSTF A/B recommendation were considered to be screened (breast, colon and cervical). Lung and prostate cancer were considered partially screened. Prostate cancer has a USPSTF grade C recommendation for screening for the study period. 16 Lung cancer has a USPSTF grade B recommendation for screening, but these were published in 2013 only covering a portion of our study period. 17 The remainder of cancers were considered unscreened.
We assessed the rates of patients achieving cancer quality metrics based on Commission on Cancer (CoC) guidelines. 18 We specifically evaluated the rates of patients achieving these benchmarks within bladder, colon, gastric, and lung cancers as these contained robust data in the SEER dataset based on lymph node yield from pathologic data. For bladder cancer, this requires “At least 2 lymph nodes are removed in patients under 80 undergoing partial or radical cystectomy”; Colon cancer requires “At least 12 regional lymph nodes are removed and pathologically examined for resected colon cancer”; Gastric cancer requires “At least 15 regional lymph nodes are removed and pathologically examined for resected gastric cancer”; Lung cancer requires “At least 10 regional lymph nodes are removed and pathologically examined for AJCC stage IA, IB, IIA, and IIB resected”.
Sensitivity Analysis
We performed a sensitivity analysis which involved changing the inclusion and exclusion criteria for the control and consolidation groups. Control groups used were the original definition with HHI <200 and final HHI <2500; final HHI <1500; and MSA which met the FTC definition for low concern (HHI change <100 or final HHI <1500). 13 Experimental groups were defined as the original definition with HHI >200 and final HHI >2500; any MSA which met the FTC definition for high concern (HHI change >200 and final HHI >2500). 13 A Cox regression survival analysis was then performed with each of these definitions.
Statistics
We utilized multivariate difference-in-differences (DID) regression analysis to compare changes in the percentage of early-stage cancer diagnosis, the percentage of patients achieving Commission on Cancer (CoC) Quality Measures in bladder, colon, gastric, and lung cancers, and overall survival. These comparisons were made between the initial evaluation period of 2008-2009 and 2015-2016. These periods were chosen to compare the acceleration of consolidation as represented by national trends over 8 years between 2008 and 2015. The DID models were adjusted for age, sex, race, cancer site, county percentage of patients below high school education, county percent of patients below poverty, county unemployment percentage, and county median household income. Our analysis did not include multiple comparison analysis because our primary analysis had a singular clear endpoint, with only exploratory investigations for secondary endpoints.
The DID analysis helped us control time-invariant characteristics such as sex, race, education level between MSA’s and to estimate the causal effect of HHI on diagnosis, cancer quality metrics, and overall survival. The DID model was flexible and was chosen to answer how effects differed between 2008-2009 and 2015-2016. We visually verified parallel trends assumptions by creating line graphs for each variable. Survival outcomes were analyzed using a Cox regression analysis to determine hazard ratios. Statistical analyses were performed using SPSS, version 29 (IBM Corporation). Determination of hazard ratios was given preference over other survival models to determine a proportional effect of covariates on outcomes instead of using a log-rank test to test for differences in survival between groups.
Results
Our study revealed increasing hospital consolidation in our cohort from 2008-2009 to 2015-2016. Out of 23 MSAs in SEER, the mean HHI increased from 2830 to 3096, representing an average increase of 266 over the study period. Initially, five MSAs were unconsolidated, eight were moderately consolidated, and ten were highly consolidated. By 2015 to 2016, only two MSAs remained unconsolidated, while six were moderately consolidated and fifteen were highly consolidated (Supplemental Table 1).
A total of 138 784 cancer patients between 2008 and 2016 were included who were residing in areas that experienced high hospital consolidation or served as the control area (Table 1). We identified five MSAs that experienced high hospital consolidation over the time period and one control that experienced no significant change in hospital consolidation (Table 2). The change in HHI for the control MSA was +24, while the mean change in HHI in the experimental groups was +1170.
Study Cohort Demographics and Clinical Characteristics.

Note. Demographic information of study cohort.
Level of Hospital Market Consolidation in Control Versus Consolidated MSAs.
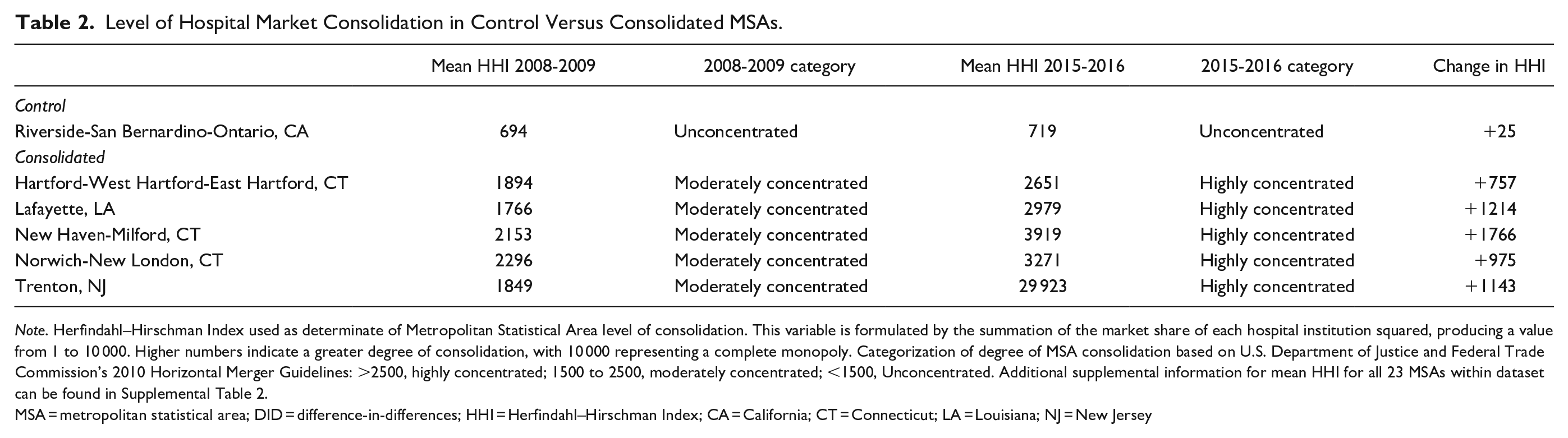
Note. Herfindahl–Hirschman Index used as determinate of Metropolitan Statistical Area level of consolidation. This variable is formulated by the summation of the market share of each hospital institution squared, producing a value from 1 to 10 000. Higher numbers indicate a greater degree of consolidation, with 10 000 representing a complete monopoly. Categorization of degree of MSA consolidation based on U.S. Department of Justice and Federal Trade Commission’s 2010 Horizontal Merger Guidelines: >2500, highly concentrated; 1500 to 2500, moderately concentrated; <1500, Unconcentrated. Additional supplemental information for mean HHI for all 23 MSAs within dataset can be found in Supplemental Table 2.
MSA = metropolitan statistical area; DID = difference-in-differences; HHI = Herfindahl–Hirschman Index; CA = California; CT = Connecticut; LA = Louisiana; NJ = New Jersey
Cancer Stage at Presentation
The rate of early-stage cancer diagnosis decreased by 1.0% in areas with increased consolidated areas and 1.8% in control regions. Adjusted DID models showed that hospital consolidation was associated with a 1.1% (CI −2.3 to 0.0%) increase in presentation of cancer at an early stage-stage with higher rates of early-stage diagnosis in consolidated regions (Table 3).
Outcomes of Cancer, CoC Quality Metrics, and Overall Survival.

Note. Adjusted for age, race, sex, cancer site, county percent under high school education, county percent in poverty, county percent unemployed, and county median household income.
DID = difference-in-differences; CoC = Commission on Cancer; CI = confidence interval.
Cancer Quality Metrics
Commission on Cancer Quality metrics were evaluated for bladder, colon, gastric, and lung cancer. Rate of achievement of bladder cancer quality metrics across the study period showed −3.4% absolute difference between intervention groups and adjusted DID models showed a −4.3% (CI −7.9 to 0.6%) change in achievement these quality controls. Colon cancer quality metrics improved by an absolute 3.7% in the control group compared to consolidation. Adjusted DID models showed 3.7% (CI 0.1-7.3%) greater improvement in the control group. Gastric cancer quality metrics demonstrated an absolute difference of 12.9% greater increase in the control group with adjusted DID models similarly showing 12.5% (CI 0.9-24.0%). Finally, lung cancer quality metrics showed a nonsignificant 3.8% increase in the control group with DID models showing 3.5% (−0.6 to 7.5%) greater improvement in the control group (Tables 4 and 5).
Subgroup Analysis for Cancers With and Without Screening Recommendations based on Early-Stage Diagnosis.

Note. Cancer types were stratified into those with grade A or B USPSTF recommendations throughout entirety of study period. Lung cancer USPSTF grade B recommendations were made in 2013 within study period and prostate cancer USPSTF screening recommendations are grade C, thus were assigned as Partial screening recommendations. The remainder of cancers were considered unscreened.
Adjusted for age, race, sex, cancer site, county percent under high school education, county percent in poverty, county percent unemployed, and county median household income.
DID = difference-in-differences; CI = confidence interval.
Subgroup Analysis for Cancers With and Without Screening Recommendations.
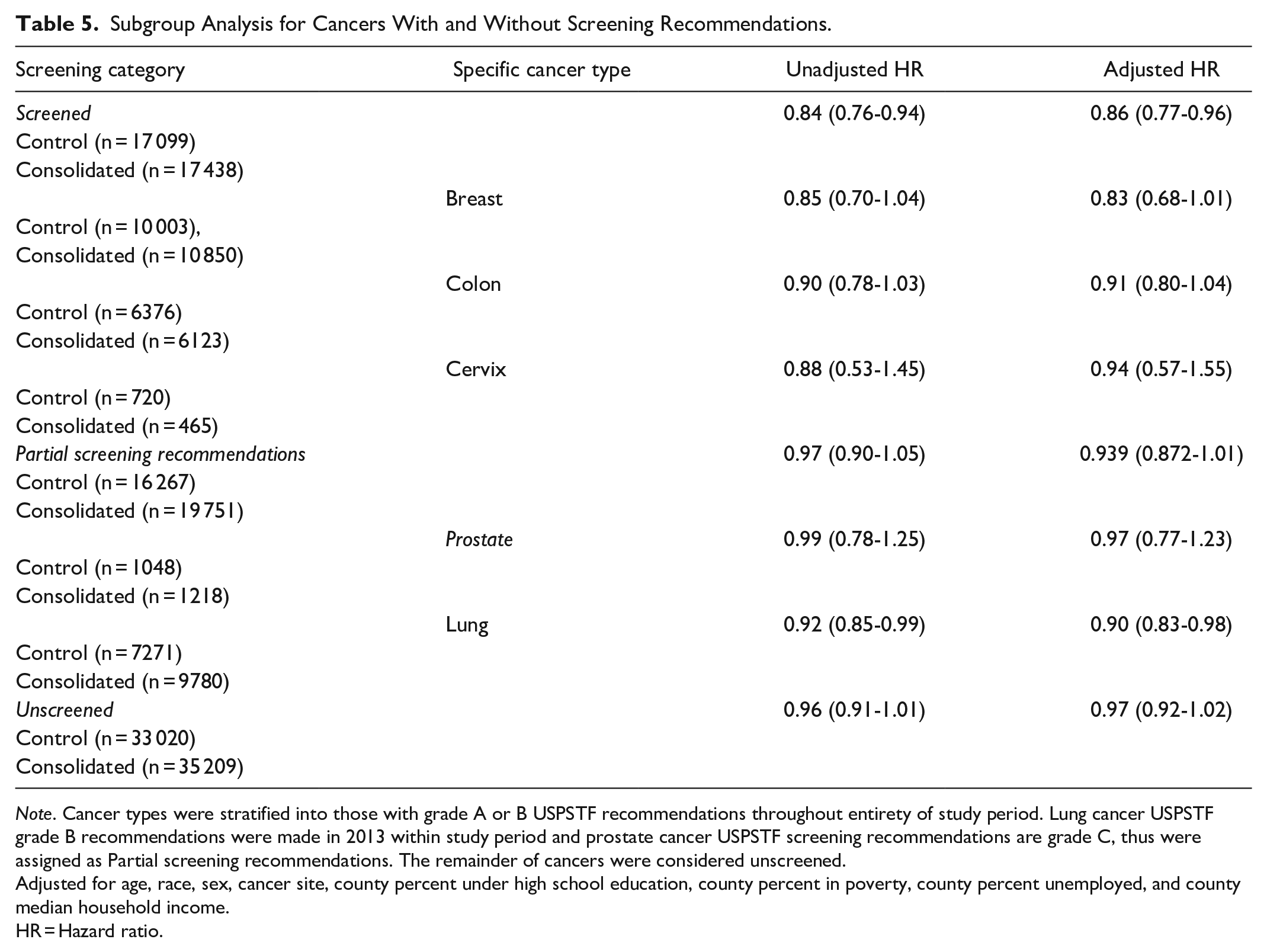
Note. Cancer types were stratified into those with grade A or B USPSTF recommendations throughout entirety of study period. Lung cancer USPSTF grade B recommendations were made in 2013 within study period and prostate cancer USPSTF screening recommendations are grade C, thus were assigned as Partial screening recommendations. The remainder of cancers were considered unscreened.
Adjusted for age, race, sex, cancer site, county percent under high school education, county percent in poverty, county percent unemployed, and county median household income.
HR = Hazard ratio.
Overall Survival
Overall survival was improved in regions with increased hospital consolidation compared to controls with the adjusted hazard ratio 0.94 (0.90-0.98).
Subgroup Analysis
We performed a subgroup analysis for cancers with screening recommendations, partial screening recommendations, and no screening recommendations. Screened cancers were found to have a 2.0% improvement in early-stage diagnosis in adjusted DID model for the consolidated group compared to control, while partially screened cancers showed a 1.7% improvement in the consolidated group. This contrasted with the unscreened cancers which showed a non-significant 0.6% improvement in early-stage diagnosis in the control group. Screened cancers showed significantly improved overall survival with adjusted hazard ratio 0.86 (0.77-0.96), compared to 0.94 (0.87-1.01) for partially screened cancers. In contrast cancers without screening recommendations did not experience any significant change in survival 0.97 (0.92-1.02).
Sensitivity Analysis
Our sensitivity analysis investigated the hazard ratios for overall survival with varying definitions for which MSAs were included in the control and experimental groups. We found persistence of statistical significance for improved overall survival for the control group with all combinations of definitions (Supplemental Table 2).
Discussion
We found that increased hospital market consolidation may have some benefits for cancer patients. Firstly, we observed that increased consolidation was associated with improvements in early-stage diagnosis and overall survival. These benefits were primarily seen in cancers with screening recommendations, suggesting that improvements in cancer screening may be one of the drivers of these positive outcomes. However, we did not observe consistent significant changes in cancer quality metrics in areas with increased consolidation. These findings highlight the potential of increased consolidation to improve cancer outcomes but that these improvements are not universal.
Much of the previous literature on the effects of hospital market consolidation have focused on the costs of care. Previous analyses of the prices of care after hospital consolidation have consistently observed increased prices after hospital mergers. Gaynor and Town 8 found that prices of hospital services after hospital mergers increased up to 20% due to lack of competition, especially in mergers that are geographically close. Consolidated hospitals benefit from being able to charge higher prices for care while also saving money through sharing facilities and the efficiencies of a single consolidated system. 19 These hospital systems also have increased market power, in that they can raise rates without losing insurance contracts, as insurers needed to stay contracted with the fewer healthcare systems in a given location to provide adequate coverage for their insured. 19 Schmitt 20 found in analyzing hospital mergers between 2000 and 2010, hospitals were realizing cost savings ranging from 4% to 7% after consolidation. An overview of the literature by Bazzoli et al 21 found that hospital mergers almost universally lead to cost savings for the hospital while also increasing the price of services. These findings demonstrate little evidence of cost savings being passed on to consumers, as utilizers of these healthcare systems usually end up seeing higher insurance premiums and health-care associated costs. 22
Previous studies comparing health outcomes after hospital market consolidation have shown inconsistent results. Beaulieu et al 12 investigated data surrounding the acquisition of 246 hospitals occurring between 2009 and 2013 and found a moderate decrease in patient-experience measures following mergers and no changes in readmission or mortality rates. Hayford 6 analyzed 40 hospital mergers between 1990 and 2006 and found higher post-merger treatment intensity and a 1.7% increase in inpatient mortality. In contrast, Jiang et al 23 investigated outcomes in rural hospitals after mergers, using 172 merged and 266 comparison hospitals, and found improved mortality outcomes following acute myocardial infarction in hospitals which had undergone consolidation. This data provides a context in which our findings of improved overall survival, and rate of early-stage of diagnosis of cancer patients in increasingly consolidated hospital systems is supported. However, this variability in findings likely reflects the significant diversity of regional differences leading to hospital consolidations, including geographic locations, economic incentives, population composition, and political landscapes.
Our study identified slight improvement in early-stage diagnosis of cancer and overall survival in areas that experienced increased hospital consolidation. We found that these improvements were primarily restricted to the subset of cancers with high level USPSTF recommendations for cancer screening. Our consolidated subgroup demonstrated a 1.1% increase in screening with a 3.8% increase in early lung cancer detection and 3.7% for colon cancer. While our dataset does not have information on the number of cancer screening exams, we proposed that hospital consolidation may have improved coordination of care leading to improvements in cancer screening. However, without data on specific rates of cancer screening in our data we are unable to directly draw this conclusion. It can be hypothesized that early diagnosis could be due to enhanced information sharing between different healthcare providers under a single network 23 that may improve follow up. Similar to other quality metrics, local ownership of screening benchmarks within a consolidated system and implementation of incentive-based analytics may drive improved rates of early diagnosis. 3
It is noteworthy to highlight that our improved survival hazard ratio was limited to those cancers with screening recommendations. Previous studies have shown that patient experience may be worse in areas with less competition and be correlated with higher prices, it could be suggested that the modest improvements in cancer quality metrics are diluted across the scope of care from diagnosis to regular treatments. Therefore, it is important for consolidated organizations to monitor and reassess their quality metrics to capture the outcomes across the range of services that cancer patients receive.
Our study contains several limitations. First, our data is based on MSA geographic regions and not individual hospitals. While we consider this a limitation, a strength of this is that our approach accounts for shifts of patients to different hospitals. Second, our control group is limited to a single MSA race. As the majority of MSAs across the United States experienced increased consolidation during our study period, this is consistent with national trends. In addition, patient characteristics from our control area did not differ significantly from our consolidated MSAs. Third, there is a lack of information regarding the specific practices of cancer screening in each of study groups, which may function as a confounding variable, given the importance we found in the stratification of screening on overall cancer outcomes. In addition, our dataset does not contain information on cost of care to determine the value of the care delivered. Lastly, the database established by the SEER program encompasses 26% of the US population 24 and our cohort consists of approximately 8% of this group. We account for this limitation by highlighting the similarities between our cohort and the overall SEER database (Table 1), our population had a mean age of 69.8 years, male % of 50.98%, 81.5% White participants, and median family income of $77 834—falling within the deviation of the overall SEER data demographics.
While we adjusted our model for age, sex, race, the SEER regions have a higher proportion of non-white individuals and survival rates derived from this dataset may not be representative of national cancer mortality rates. 24 A 2017 report on the influence of comorbidities on non-cancer mortality showed only slight differences when weighted using the Charlson index, 25 nevertheless, for future investigations, it would be valuable to assess the comorbidity index for the 2008-2009 and 2015-2016.
Understanding the implications of hospital consolidation is crucial for healthcare policymakers to make informed decisions about hospital mergers and ensure that quality and value of cancer care remains consistently high. Hospital consolidation provide the potential for improved efficiencies and improvements in the quality of care but also for increased costs. To mitigate the negative impacts of consolidation, 4 regulatory bodies should encourage disclosure and transparency in price and cost to the patient to allow informed decision-making. In addition, alternative payment models such as value-based care under accountable care organizations (ACO) could improve care coordination and efficiency. 26 A delineation of the metrics sensitive to improvement with consolidation suggests an avenue for restructured resource allocation or may elucidate gaps that should be addressed to optimize efficiency and quality of care delivery.
Our study indicates that one potential improvement from hospital consolidation is improvements in care coordination and cancer screening. We encourage further investigation of the role of insurance coverage in access to cancer screening and subsequent care, in the context of equitable access for underserved populations since the SEER database does not represent private insurance models. Additional research could also examine the long-term implications of either horizontal or vertical integration during consolidation on overall population health to inform policy. The potential outsized importance of cancer screening in effecting outcomes is a conclusion which deserves further study and consideration.
Conclusions
Our study suggests that certain cancer outcomes may be improved with hospital market consolidation. For example, upon subgroup analysis, early stage of diagnosis and survival were improved in cancers with screening recommendations in areas that underwent greater hospital consolidations while rate of achieving CoC quality care metrics was more equivocal. Further research is needed to confirm these findings and to understand the mechanisms by which hospital consolidation affects cancer outcomes.
Supplemental Material
sj-docx-1-inq-10.1177_00469580251314954 – Supplemental material for Association of Hospital Consolidation with Cancer Outcomes
Supplemental material, sj-docx-1-inq-10.1177_00469580251314954 for Association of Hospital Consolidation with Cancer Outcomes by Justin Graff, Mahnoor Ayub, Prashanth Prabakaran, Brendan Keelan and John D. Cramer in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Author Contributions
J.G: Conceptualization, Methodology, Validation, Investigation, Writing – Original Draft, Writing – Review and Editing. M.A: Investigation, Writing – Original Draft, Writing – Review and Editing. B.K: Writing – Original Draft. P.P: Review and Editing. J.C: Conceptualization, Methodology, Validation, Investigation, Writing – Original Draft, Writing – Review and Editing, Supervision, Funding acquisition.
Data Availability
Data available upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Detroit Medical Center Foundation Grant.
Ethical Statement
All procedures were performed according to the ethical standards of the institutional review board. All data pertaining to individuals was anonymous. The institutional review board of Wayne State University deemed this study exempt. As we utilized a publicly available anonymized dataset, ethical approval for the study was not required
Informed Consent
The institutional review board of Wayne State University deemed this study exempt.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.