
Abstract
This study aims to examine the effectiveness of mHealth delivered through LINE application in improving physical activity of older adults. This was a parallel, two-arm, randomized controlled trial, single-blind allocation to experimental and control groups. The sample consisted of 91 individuals (46 experimental and 45 control groups) aged 45 years or older, and had internet access. Intervention group received customized activities focused on raising awareness and knowledge provision for 8 weeks. Out of 91 participants, 82 completed the study (41 in each group). Comparison of Mean Difference values within groups found a significant difference at P < .05 (t = 2.294). The experimental group increased their PA by 7.2 min on average, while the control group decreased to 44.1 min. Subgroup that fully complied with the activity process had a significantly higher percentage of adequate PA at P = .01 level (χ2 = 7.853**). Tailoring activity content to older adults’ diverse lifestyles via a Mobile Health application can effectively boost PA levels by meeting their needs conveniently and quickly.
Clinical trial registration: Thai Clinical Trials Registry (TCTR) TCTR20240422004.
Introduction
Engaging in sufficient physical activity (PA) contributes to good health and strength in both physical and mental aspects. The World Health Organization (WHO) suggests moderate to vigorous PA (MVPA) totaling at least 150 min per week to help reduce the risk of non-communicable diseases (NCD) such as diabetes, coronary artery disease, breast cancer, and colorectal cancer.1 -3 Additionally, PA contributes to significantly reducing premature mortality.4,5
Similar to global situation, the prevalence of sufficient MVPA among older persons in Thailand (age 60+ years) continue to be lower compared to younger adults in the population.5 -7 Age-related adverse health issues, such as decline in bone density, weakening of muscle strength, and problems with various joints, are the most common reasons of low PA among older person in addition to concerns about accidental falls. 8 The onset of illness and physical decline over time inevitably leads older persons to suffer insufficient PA, which can lead to various NCD. Psychologically, insufficient PA contributes to declining cognitive ability, such as dementia, Alzheimer’s disease, and depression among older persons. 9
Promoting PA among older persons is crucial to improving their physical and mental health. The advancement of information technology such as mobile health (mHealth) has shown to be effective in facilitating wider access to health information for all populations.10,11 MHealth has now become an important tool for self-managed physical health care in many countries around the world 12 and serves as a medium for providing advice, for example, there is data sharing between patients and caregivers, including data transmission of an abnormal condition in emergency cases, and comprehensive physiological data of patients collected remotely. There are surveillance systems related to remote databases where collected physiological data is sent and stored periodically, accessible by doctors, families, and friends (based on different permissions) to manage and monitor the current and past conditions of patients. 13
Although mHealth serves as a tool that facilitates easy access to health information and communication, older persons may find it difficult to access technology-based information sources. This difficulty arises when the tools are not designed to be elder-friendly, such as having too small font sizes that make it challenging to read, leading to reluctance or avoidance in using the tools. Additionally, overly complex menu navigation can also contribute to usability challenges for older persons.14,15
We developed an mHealth system through the LINE application called “Nong Paew Waew,” aiming to create and enhance tools for monitoring and sharing appropriate health behavior information for older persons, accessible anytime and anywhere. The core concept involves conveying emotions and feelings akin to being cared for by a grandchild, who monitors and provides alerts to ensure that older persons engage in sufficient PA. This includes notifications and embedded knowledge about safe PA practices tailored to the older person’s behavioral context throughout the day. Continuous health education and information has shown a positive result in enhancing PA participation. 16 In addition, the apps also provides a real-time health status notification that older persons can directly monitor and then to follow up and seek advice from healthcare professionals. This study aims to evaluate the effectiveness of a mobile health (mHealth) intervention, delivered via LINE application, in improving physical activity of older adults. By participating in the intervention, we expect an increase in the physical activity of the sample in the experimental group, and this increase will be higher than individuals in the control group.
Methods
Study Design, Population and Sample
This study is a two-arm, randomized, controlled trial, conducted in a single-blind manner with a pretest-posttest control group design. Participants were randomly selected using probability random sampling based on personal-level factors, ensuring equal chance of selection for all individuals in the population of interest. Both the experimental and control groups were blinded to their group assignment to minimize bias in participation.
The population of interest in this study consists of older persons and middle-age adults age 45 years or older, who have internet access. They were selected from the database of health service recipients at the primary level of Ban Salawan Subdistrict Health Promotion Hospital, responsible for providing services in the area of Village #5 and #6, Salaya Subdistrict, Phutthamonthon District, Nakhon Pathom Province. We selected this hospital due to the high number of older adults being served in the area. Subsequently, the research team established inclusion criteria for selecting the sample groups for this study as follows: able to access the internet and be age 45 years or older, is a Thai citizen, does not have a disability, and is willing and enthusiastic to participate in the research throughout the study process.
This study calculated the sample size using analysis through G*Power version 3.1 software. 17 To ensure statistical robustness and prevent dropout or refusal during the study, the research team increased the sample size by more than 10%, resulting in a final sample size of 40 individuals per group. In each subgroup, individuals were categorized based on the proportional distribution of sex and age ranges, include those in middle-age adults and those in old age. The reason for defining the pre-elderly population to participate in the study is to ensure the generation of knowledge that can be used to prepare the health readiness of the population promptly before entering old age.
Randomization
After determining the sample size, the procedure for sampling to obtain the study sample groups is as follows. Cluster sampling was used to randomly select samples by dividing the population into clusters based on villages. Subsequently, villages were randomly sampled using Probability Random Sampling with Simple Random Sampling with replacement to obtain 2 village sample groups for the experimental and control areas. Random Selection was employed to determine the experimental and control areas and designated cluster 5 as the experimental group, whereas cluster 6 as the control group. Sampling of individual participants involved a systematic sampling from the database of healthcare service recipients at the primary level of care provided by Ban Salawan Subdistrict Health Promotion Hospital. In this sampling stage, the population was divided into equal intervals based on proportions calculated from the sample and population sizes. The sampling started by randomly selecting a number to obtain the first sample unit. Subsequent sample units were selected sequentially by counting according to the calculated intervals. This process continued until the predetermined number of sample groups was reached. Throughout this process, all sample (91 participants) selected for the experimental (46) and control (45) groups were blinded to their group assignment to reduce bias in participating in research intervention activities.
The Intervention: Mobile Health Intervention With the Experimental Group
This activity proceeded within the experimental group of the sample, conducted over a total of 8 weeks (from September 16 to November 23, 2023). The key focus of this intervention process was the utilization of population characteristics, health-related information, data on health behavior, as well as measures of knowledge, and understanding regarding PA within the sample group prior to the experimental phase (Table 1).
Intervention Activity Plan.

The activities were conducted exclusively online via the LINE application (LINE Official Account) named “Nong Paew Waew,” which served as the primary tool for the intervention (Figure 1). Throughout the process, emphasis was placed on two-way communication to facilitate discussion, inquiry, and exchange of opinion between the researchers and the participants. The researchers sent activity information in the morning, afternoon, and evening every day. This schedule was based on observations that a number of middle-age adults and older persons accessed LINE immediately upon waking and again during breaks from work, particularly around noon and before bed. Therefore, the research team chose these times to send information to maximize the likelihood of participants reading the messages. 18 Regarding the content of the activities, the research team considered the format of the content, emphasizing simplicity, engagement, accuracy, clarity, and reliability. 19 The sources of infographics and media used for communication came from 3 channels: Social Marketing Thaihealth (Thai Health Promotion Foundation), Mahidol Channel, and the TPAK website. Additionally, some media were provided by the Communication for Knowledge Transfer Team at the Thailand Physical Activity Knowledge Development Center (TPAK), which assisted in producing and creating the artwork.

Functions of the LINE application: Nong Paew Waew.
Measurement
Physical activity was measured objectively using the ActiGraph wGT3X-BT accelerometer (set at 50 Hz). Participants wore the device on their waist for 24 h a day (except during showers) for 3 days. PA measurement was conducted twice, before and after the intervention, to ensure reliable and accurate data on the participants’ PA behavior.
Structured questionnaire administered through Lime Survey collected personal data, awareness of PA, knowledge of PA, and access to health facilities.
Data Management and Analysis
This research collected PA data using accelerometers from the entire sample group to obtain quality and sufficient PA data for analysis. The data management process utilized ActiLife software version 6.13.5. To determine if individual wear time durations were sufficient for data analysis, the Choi algorithm was employed. Research has shown that the Choi algorithm is more accurate for assessing wear time durations of waist-worn accelerometers. 20 Freedson VM3 (2011) algorithm was used to analyze energy expenditure 21 whereas Troiano Adult (2008) algorithm was used to analyze MVPA.22,23 The data obtained after data management included kilocalories (Kcal), metabolic equivalents (METs), light physical activity (PA-Light), moderate PA (PA-Moderate), vigorous PA (PA-Vigorous), moderate-to-vigorous physical activity (MVPA), sedentary behavior (Sedentary), sleep duration (Sleep), and steps (Step).
Uni-variate analysis was used to describe the characteristics and distribution of data, such as percentages, means, and medians. Bivariate analysis was used to describe data in the form of cross-tabulations and compare differences between group-level variables. Inferential statistics were used to examine the effectiveness of models. With normal data distribution, paired t-tests was employed to compare means before and after within the same group, and independent sample t-test was used to compare means between 2 groups. This study used the SQUIRE (Standards for QUality Improvement Reporting Excellence) guidelines for its reporting. 24
Results
Out of a total sample of 91 individuals, 9 withdrew from the study after refusing to provide post-experimental data. Therefore, the study sample for this research consists of 82 individuals in total, divided into an experimental group of 41 people and a control group of 41 people (Figure 2). The sample group has a mean age of 65 years (SD = 9.23). The mean age of participants in the control group was slightly older (66.4 years, SD = 9.43) than the intervention group (63.9 years, SD = 8.97). In both groups, the proportion of females was higher than males; 63.4% and 65.9% in the intervention and control group, respectively. The majority of the sample (73.2% in the intervention group and 78.0% in the control group) was married or living together In terms of body mass index (BMI), the experimental group has a mean BMI of 25.2 kg/m² (SD = 3.44), while the control group has a mean BMI of 23.6 kg/m² (SD = 4.67). Regarding chronic illnesses, both the experimental and control groups have an equal proportion of individuals with chronic illnesses, which is 30 (73.2%).
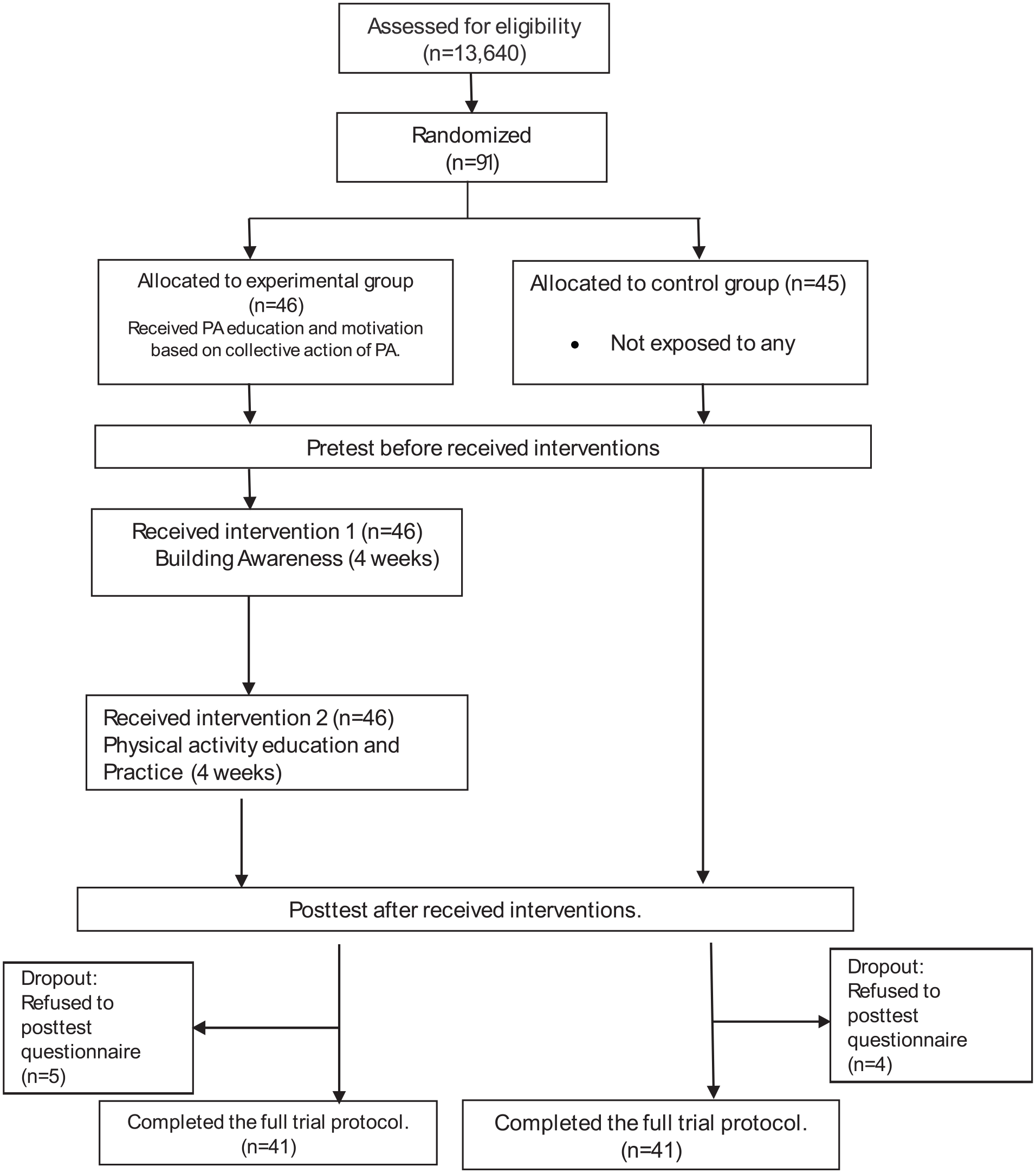
CONSORT (Consolidated Standards of Reporting Trials) flow diagram.
In the baseline (prior to the intervention), 70.7% of individuals in the experimental group have heard the term “physical activity’’. This proportion is slightly higher than of those in the control group (63.4%). Nevertheless, in terms of the average amount of PA (min/week), individuals in the experimental group collected lower level of PA than their counterparts in the control group (140 min/week and 181 min/week, respectively). Hence, testing for differences between the experimental and control groups reveals no significant difference (P > .05), indicating that initial data for comparing changes in PA between both groups can be used to assess the effectiveness of intervention activities (Table 2).
General Characteristics of the Sample.

Note. MVPA = moderate to vigorous physical activity.
P-values are based on the Chi-square test.
P-values are based on the 2-tailed t-test.
The intervention activities were conducted as planned over an 8-week period. The results of this study supported the research hypothesis as follows: when comparing the average PA between the experimental and control groups, no statistically significant difference was found. However, when comparing the mean difference within each group to analyze changes in PA, a statistically-significant difference was observed within the groups at P-value .05 level (t = 2.294). After participating in the intervention activities, the experimental group showed an average increase of 7.24 min in PA, whereas the control group decreased by 44.13 min. This indicates that participation in the intervention led to significant increase in PA (Table 3).
Effectiveness of the Intervention on Average PA Comparing by Sample Group.

Significance at P-value .05.
Further, the analysis categorizes the intervention group based on compliance with the complete activity process. This involves testing the continuous participation in the intervention activities of the experimental group to assess whether it assists in improving the effectiveness of the intervention. The experimental group is divided into 2 subgroups: (1) those who fully comply with the activity process, and (2) those who do not fully comply with the activity process. Compliance is considered as an important indicator for behavioral change, including PA. Data for this analysis comes from activity participation data, interactions, discussions, reflections, and feelings of the experimental group through the LINE Nong Paew Waew app, used to analyze the PA adequacy differences between both experimental subgroups.
When comparing the percentage of adequate PA between both subgroups using the Chi-square test, it was found that, after participating in the intervention, the subgroup that fully complied with the activity process had a significantly higher percentage of adequate PA at P = .01 level (χ 2 = 7.853**) (Figure 3). Specifically, the subgroup that fully complied with the activity process demonstrated 53.6% adequacy in PA, indicating a clear impact that participating in prescribed activities while fully complying with the activity process can effectively change the adequacy of PA within the experimental subgroup.
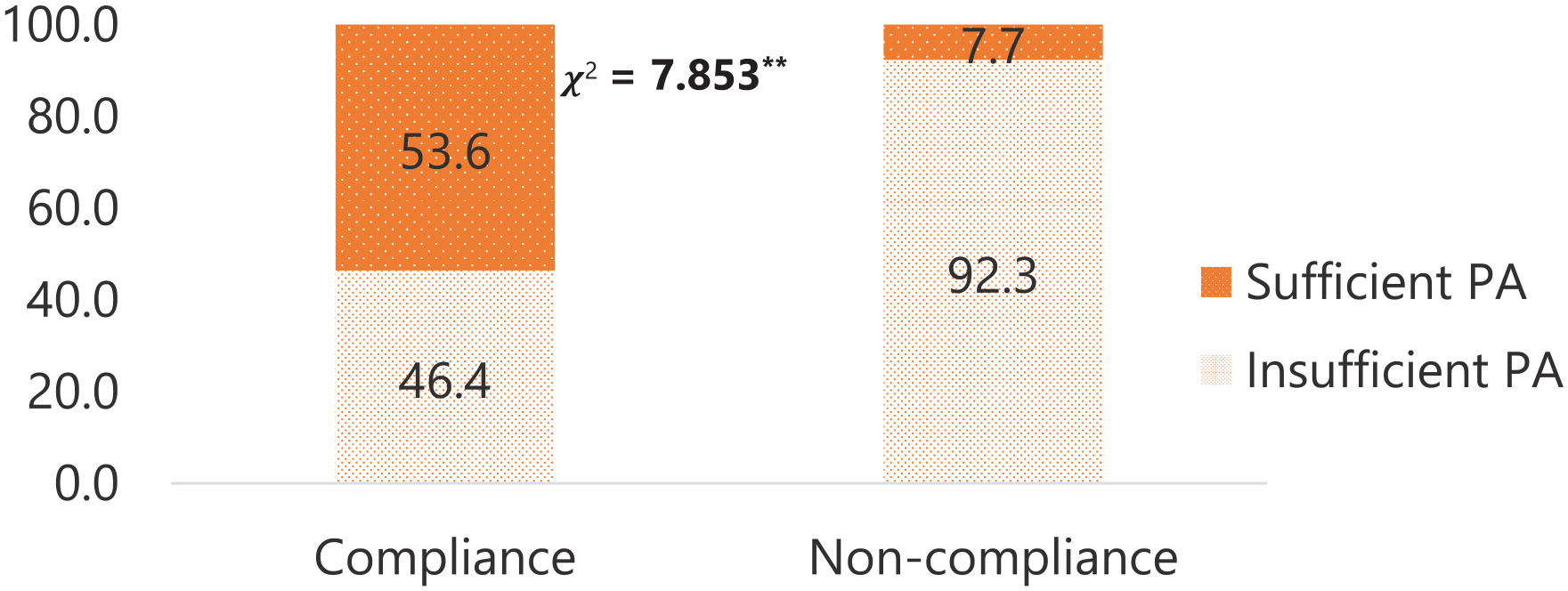
Percent adequate PA by experimental group after the intervention.
Discussion
The rapid development of information technology has led to the widespread use of mHealth (Mobile Health) systems in designing health intervention activities and promoting PA. 25 This study promoted PA among older persons through the design of intervention activities using technology to facilitate communication and monitor PA behavior. The intervention involved providing personalized PA advice and health-related feedback tailored to the characteristics and behaviors of the experimental group. The finding of this study supported our hypothesis, shown by improved healthy behaviors of the participants in the intervention group, marked by a 7.24 increase in the cumulative min of PA, whereas the control group decreased by 44.13 min. This indicates that information technology (mHealth) is effective in delivering health education messages. Previous studies utilized mHealth also showed a consistent finding, although with an emphasis on population with adequate internet access and motivational back up.26,27
This study suggested that the design of the apps and appropriate intervention deliveries may increase its effectiveness. Providing real-time tracking, feedback, and motivation on PA is shown to be one of the greatest values of the app apart from the design of LINE applications that utilized a local figure (Nong Paew Waew). In the Thai context, the figure Nong Paew Waew is believed as a positive norm, portraying a caring granddaughter, engaging in conversations and providing positive information to their grandparent(s). Studies showed that two-way communication strategies has always been more effective than one-way methods.27,28
The study also applied the Health Believe Model (HBM) framework through LINE app “Nong Paew Waew,” which was designed to induce positive changes in PA behavior among the experimental group. This approach aligns with findings from international research indicating that personalized PA advice, guidance on PA guidelines, goal setting, motivation enhancement, and self-monitoring through app-based messaging contribute significantly to increasing PA among older persons.29,30
The intervention was designed considering different behavior between middle-age and older adults. A decision tree model was used to simulate decision-making methods for engaging in PA within the sample group through the aforementioned data. Various factors related to decision-making on PA were used to categorize behaviors into subgroups and design intervention activities tailored to the behaviors of each subgroup. This subgroup categorization provided in-depth insights into linking characteristics of the sample group, and suggested strategies for designing intervention activities that could potentially impact the PA levels of individuals within the group. 31
The intervention deliveries also considered the appropriate timing in sending the health messages. The researchers sent activity information in the morning, afternoon, and evening every day during the period of the study. This schedule fits with the Thai context, where middle-aged adults and older persons accessed LINE immediately upon waking and again during breaks from work, particularly around noon and before bed. The contents was also designed to be “user-friendly” for older person, emphasizing simplicity, engagement, accuracy, clarity, and reliability of information.
The finding of this study also suggests that compliance and active participation in the intervention has increased the likelihood to have higher PA level than those who inconsistently applied the recommendations. Previous studies have shown that adherence with all stages of the intervention are imperative in order to attain the desired outcomes. 32 Intervention that ensure adherence toward specific behavioral goals also showed a higher efficacy in sustaining its positive impact in the long run. 33
This study has limitations, such as not evaluating the long-term effectiveness of the intervention after the research ends, which prevents tracking the sustainability of the gains from the intervention. However, previous studies also suggested that mHealth interventions can foster small to moderate increases in PA. The effects are maintained long term; however, the effect size decreases over time. 34 The tailored intervention may serve both as the strength and limitation of the study. While it may fit the context and characteristics of the study population, it may not be applicable to other groups of population. To generalize these findings to other population sub-groups, it is necessary to consider their specific characteristics and health behaviors to develop tailored interventions that align with each group. The notifications of various activities must also consider the lifestyles and personal needs of each subgroup to ensure that PA promotion is maximally effective. 26 The duration of intervention activities is another crucial point because stimulating behavior change in PA through an mHealth systems requires consideration of suitable durations for the activities to be conducted. This involves collaboration with relevant units in planning and implementing activities to ensure that PA promotion is consistent, continuous, and sustainable. 25
Conclusions
The design of the intervention process and content of activities tailored to different lifestyles of older persons through the Mobile Health LINE application “Nong Paew Waew’’ is convenient, fast, and responsive to the needs of older persons. It can effectively enhance PA among older persons. The process-oriented model can be applied to develop health promotion software products for various health services and industries. The findings of this study provide important evidence to support decision-making regarding PA promotion for older persons in the country. The findings can be used as a reference for designing guidelines and long-term PA intervention processes tailored for older persons.
Footnotes
Acknowledgements
The authors gratefully acknowledged the funding support from Mahidol University (Basic Research Fund:fiscal year 2023) with grant numbers FF-139/2566.
Author Contributions
Nanthawan Pomkai: conceptualization, conceived the study, formal data analysis, writing the first draft. Danusorn Potharin: conceived the study, data processing. Dyah Anantalia Widyastari: writing and revise the manuscript. Piyakrita Kaewpikul: data collection, review the revised version. Nattaporn Nilwatta: data management and processing. Vanapol Chamsukhee: visualization. Aunyarat Khanawapee: project administration. Chutima Yousomboon: project administration. Piyawat Katewongsa: conceptualization, methodology, funding acquisition. All authors reviewed and approved the submitted version.
Data Availability Statement
The data used for this manuscript is available upon request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research project is supported by Mahidol University (Basic Research Fund: fiscal year 2023) with grant numbers FF-139/2566
Ethical Approval
This research was conducted under the principles of human research ethics according to the regulations of Mahidol University. The research project protocol was certified by the Research Ethics Committee, Institute for Population and Social Research, Mahidol University, on March 31, 2024, with project code COA. No.2023/02-027.
Informed Consent
Consent was obtained from participants to conduct various activities, and data collection was done confidentially, without disclosing personally identifiable information. For the control group sample, if the activities proved effective in promoting PA upon completion of the study, they were adapted for use with the control group sample.
Registration of Clinical Trial
Thai Clinical Trials Registry (TCTR) website under the code TCTR20240422004.