
Abstract
The Age-Friendly Health System (AFHS) movement continues to grow in the United States as more health systems implement the 4Ms framework. Despite this growth, there are relatively few studies that evaluate outcomes related to AFHS implementation. This study assessed patient satisfaction with AFHS by analyzing the rate at which patients returned to the clinic for future health care, serving as a measure of quality. A retrospective cohort design using electronic health record (EHR) data obtained from patients 65 years of age and older who received care at a large national network of convenient care clinics in the U.S. (N = 987,197) between January 2021 and March 2024. We assessed the level of AFHS 4Ms care received by these individuals in relation to their subsequent visit back to the clinic through descriptive statistics, a time-to-event analysis using the Kaplan-Meier cumulative incidence approach, and a Cox proportional Hazards model, adjusted for age, race, sex, prior appointments, and number of ICD-10 code diagnoses. Throughout the study period, patients who received complete AFHS 4Ms care exhibited greater rates of returning to the convenient care clinic compared to those who received partial or no 4Ms 4Ms care. Kaplan-Meier curves demonstrated that the cumulative probability of returning to the clinic was higher in patients that received 4Ms over time, compared to patients that did not receive 4Ms. Results from the Cox Proportional Hazards model demonstrated a risk ratio of 3.91 (p < .001) of returning to the clinic, after adjustment. The results indicate that patients are more likely to seek additional care in the future at the same health system when they receive complete 4Ms care, possibly due to increased satisfaction with care. As patient satisfaction is an indicator of quality care, this finding can further inform and spread the AFHS movement.
Keywords
Introduction
The Age-Friendly Health Systems (AFHS) movement began in 2018 as a John A. Hartford Foundation initiative in partnership with the Institute for Healthcare Improvement. 1 The AFHS model proposes that implementation of the evidence-based 4Ms framework, assessment and acting on What Matters, Medication, Mentation, and Mobility, leads to higher quality and safer care for older adults. The 4Ms framework places a high importance on ensuring that older adults reliably receive evidence-based care to enhance their overall health. The delivery of Age-Friendly 4Ms care in all health care settings is important, as specialized geriatric care is not always available due to the growing number of older adults in the U.S and internationally.2,3 The need for Age-Friendly primary care was first introduced by the World Health Organization and has since expanded to include an age-friendly ecosystem of communities, states, businesses, universities, healthcare, and public health systems.4,5 The Institute for Healthcare Improvement (IHI) has recognized 3,907 care settings as Age-Friendly since 2018, benefiting 3.29 million older adults. 6 However, by 2050, the number of adults aged 65 and older will raise from 761 million to 1.6 billion. 3 Working toward implementing AFHS into new settings will be of great importance in the coming decades.
Convenient care clinics, a relatively new addition to the healthcare landscape, focus on treating non-urgent, common health issues and promoting disease prevention through screenings, vaccinations, medication management, and chronic health management. 7 Although these clinics are not intended to replace primary care visits, they can provide some primary care services that benefit patients. Convenient care clinics are known for delivering affordable care to both insured and uninsured patients and are often more accessible, cost-effective, and have shorter wait times compared to primary, urgent, or emergency care settings.7 -9 The older adult population in the United States, who frequently utilize healthcare services and often have complex health conditions, stands to benefit from age-specific healthcare services provided by convenient care clinics. Due to their accessible and affordable nature,2,7 -9 these clinics can play a crucial role in delivering age-friendly care. Therefore, convenient care clinics present an excellent opportunity to increase access to age-friendly health care for older adults.
In 2020, a large national convenient care system (herein referred to as the “Clinic”) with clinics located throughout the United States in select pharmacy retail locations began the process to become an Institute for Healthcare Improvement (IHI) AFHS Committed to Care Excellence-recognized system. 10 Clinic leadership was dedicated to enhancing the standard of care for the increasing number of older adults seeking health services in their system, with an aim to reliably integrate the AFHS 4Ms Framework during eligible visits, and equitably improve health outcomes.10 -13 The implementation of the 4Ms at the Clinic has been described previously. Briefly, the workflow involves asking the patient what matters most and aligning care with their priorities, screening for inappropriate medication using the Beers Criteria, assessing mobility as the patient walks into the clinic room from the waiting area or administering a timed-up-and-go test, and screening for depression (PHQ-2/9), and cognitive impairment (mini-Cog).10,11
Measuring patient outcomes is important to evaluating the effectiveness of 4Ms care. Several outcome measures are suggested by IHI including reducing avoidable hospitalizations and emergency department visits, early detection and action on cognitive and mental health problems, improving patient mobility, and decreasing the occurrence of falls.2,14 -16 Additional measures include improved patient satisfaction, treatment quality, and reduced healthcare expenses.1,2
Patient satisfaction is widely acknowledged as a quality indicator of healthcare excellence. 17 There is a strong association between high levels of satisfaction with efficient communication, patient-centered treatment, and improved health outcomes.16 -20 Patient retention or loyalty, as measured by patients returning to the Clinic for future healthcare services, may be an objective proxy measure of patient satisfaction. Patients who return to a healthcare organization are shown to have confidence in their healthcare providers and their contentment with the care they received.21,22 Patients choosing to return to the same convenient care clinic for either treating or preventing common ailments may be an indicator of satisfaction with the quality and accessibility of the care, as typically patients have multiple options for such health concerns. To visualize the relationship between high quality care, patient satisfaction, and return clinic visits, a simple conceptual framework adapted from the model by Quigley et al. and based on prior literature is shown in Figure 1.16 -22

Even prior to implementation of the 4Ms, the Clinic organizational culture placed significant emphasis on patient satisfaction. Upon implementing the 4Ms, the Clinic began using “CollaboRATE” survey tool to collect patient satisfaction specific to older adults.
5
CollaboRATE asks three questions of each patient 65 and older:
However, a key limitation of the collaboRATE and many other patient satisfaction surveys is that the data collection is anonymous and cannot be tied back directly to the care an individual received in the clinic. An advantage of measuring return to the clinic rates is that it can be done using a health system’s own electronic health records data without the need for additional data collection and can be measured at the individual patient level.
Despite the wide adoption of AFHS 4Ms care, there are relatively few studies that evaluate the effectiveness of the 4Ms in improving outcomes following implementation. The goal of this study is to evaluate if the receipt of AFHS 4Ms care is associated with increased rates of patients returning to the clinic for future health care needs in a large cohort of patients from a national convenient care health system.
Methods
Study Design and Population
This study uses a retrospective cohort study design. We used electronic health records (EHR) data of patients who visited the clinic from the beginning of 2021 to the end of March 2024. The study population includes adults aged 65 and older at the time of their visit to the clinic. The study was approved by the lead author’s Institutional Review Board.
Exposure Variable: Index Clinic Visit and Age-Friendly 4Ms Care
An index clinic visit is defined as the first clinic visit for a patient 65 years or older, for any cause, excluding Express Lane visits. Express Lane visits are simplified appointments for vaccines, TB testing, and Vitamin B12 injections. Patient-level data are documented through EHR charting software. The measurement of each of the 4Ms, referred to as an “M,” is the assessment, acting on, and EHR documentation of 4Ms care. Patients’ scores range from 0 to 4 Ms for each AFHS clinic visit, with 0 indicating no Ms were assessed or acted on, and 4 indicating all 4Ms were assessed and acted on.
Outcome: Return Clinic Visit/ Patient Retention
A return clinic visit is defined as a patient who returns to the clinic for any condition or need after 1 day, and before 365 days, following an index clinic visit. A window of 1 day to 365 days was chosen to eliminate immediate conditions requiring a day-of, follow-up appointment, and to set a natural cut-off for patients who may return to the clinic after a year.
Other Variables
Additional covariates included demographic characteristics, number of conditions, number prior of appointments during the study period, and reason for visit as recorded in the EHR data. Age was categorized into three groups: 65-74, 75-84, and 85 or older. Sex/gender was classified as male and female. Race/ethnicity was categorized as White or Caucasian, Black or African American, Asian, Hispanic, Native American or Alaskan Native, Native Hawaiian or Pacific Islander, and Other/Unknown. Number of conditions was calculated as the sum of ICD-10-CM codes present on the visit. The number of ICD-10-CM code diagnoses were placed into categories based on the interquartile range of the study population. The number of prior clinic appointments during the study period was added as a covariate to address prior healthcare utilization as a predictor of future healthcare utilization. Reason for the visit was determined by the chief complaint listed in the EHR, entered as a free response, which was then grouped into broader categories for analysis.
Statistical Analysis
Rates of return clinic visits, stratified by the maximum number of Ms received at any visit, were calculated for 2021 through 2023. The maximum amount of Ms received was used as the stratifying variable, as patients who return to the clinic twice within a year may not receive all 4Ms at each appointment. While 2024 data are available, it was removed from this analysis due to an incomplete window of time for patients to return.
A time-to-event analysis using the Kaplan-Meier approach was used to identify the time to a return clinic visit. A Kaplan-Meier analysis is a statistical method used to estimate the probability of an event (e.g. returning to the clinic) over time by calculating the proportion of subjects who haven’t experienced an event at each point in time. This approach allows the full use of the entire available dataset (2021 to 2024), as it allows the inclusion of those with incomplete follow-up time (right censored). We produced Kaplan-Meier curves using the cumulative incidence approach. This analysis assessed the probability of a return clinic visit over a year, stratified by the number of Ms received.
We used a Cox proportional hazards model to investigate the association between the number of Ms received and the time to return to the clinic within a year, adjusting for patient age, race, sex, count of ICD-10 codes, and prior Clinic visits. A Cox-proportional hazards model allows for a multivariable analysis of our data. Our objective was to estimate hazard ratios for the time to clinic return based on varying M counts.
Additional analyses completed including evaluating age group, race, gender, number of prior appointments during the study period, and the total number of documented ICD-10 code conditions in each patient’s visit record stratified by Ms received, as well as assessing frequencies of reason for visit stratified by return and index appointments. As returning to the clinic soon after an index visit could be an indicator of a health concern or lack of care quality, sensitivity analyses were conducted that excluded repeat visits occurring within 1 to 7 and 1 to 30 days of the index visit from counting as an event. These sensitivity analyses are available in Supplementary Materials. All analyses and visualizations were generated on RStudio version 4.3.2.
Results
Highlighted in Figure 2, patients who received all 4Ms during an eligible clinic visit demonstrated a higher rate of a return clinic visit than patients receiving 0-3 Ms. This difference is statistically significant (p < .001), and consistent across the entire study period. It also appears the relationship between the number of Ms received by a patient and the rate of a return clinic visit is dose-responsive. Patients who received 3Ms have the second-highest rate of a return clinic visit for the majority of the study period, followed by patients who received 2, 1, and 0 Ms, respectively (Figure 2). These values are summarized in Table 1, paired with additional demographic and ICD-10 code stratifications to assess for confounding variables.

Percent of patients with a return clinic visit within 1 year of an index visit, stratified by the maximum number of age-friendly ms received per visit, from 2021 to 2023.
Percent of Return-to-Clinic Visits Within a Year of an Index Clinic Visit by Ms Received, Age Group, Gender/Sex, Race/Ethnicity, and Number of ICD-10 Code Diagnoses Documented in the EHR.

An assessment of additional patient variables that may have an impact on clinic utilization demonstrates statistically significantly different rates of returning to the clinic between groups. However, the magnitude of these differences is smaller in comparison to the stratification by Ms received (Table 1). Return to clinic rates were within a few percentage points across categories of age, sex, and count of diagnosis codes. There was more variation by race with return rates between 13.9% for Asian patients on the low end and 23.7% for White or Caucasian patients on the high end.
Figure 3 displays the results of a Kaplan-Meier cumulative hazards analysis assessing the probability of a return clinic visit over the year following an index clinic visit. Similarly to Figure 2, Figure 3 shows a higher likelihood of patients who received all 4Ms returning to the clinic, followed by 3, 2, 1, and 0 Ms (p < .001).
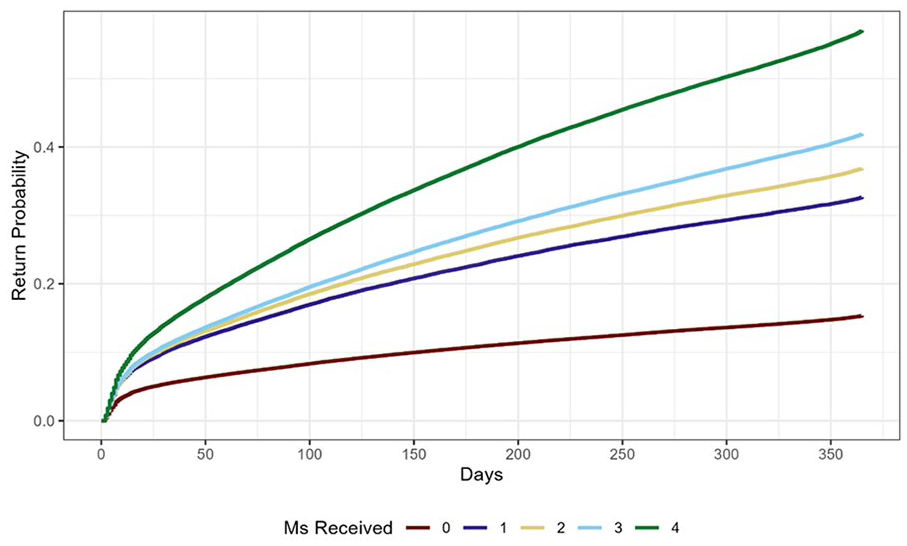
Kaplan-Meier cumulative hazard analysis demonstrating the probability of a return clinic visit over a year by the maximum number of Ms received per visit, from 2021 to 2024.
Table 2 demonstrates a comparison of the distribution of primary reason for visit between index and repeat appointments. While ear, nose, and/or throat concerns are the majority of both return and index clinic visits, Diagnostic/lab appointments are more common in index visits, and gastrointestinal visits are more common in repeat visits.
Reason for Index Visit Category, Stratified by Repeat or Index Visit.

Table 3 and Figure 4 highlight the results of a Cox proportional hazards model, predicting the rate ratios of returning to the clinic within a year of an index visit by the number of Ms received. After adjusting for age group, race, gender, number of ICD-10 code diagnoses, and total number of appointments during the study period, patients who received all 4Ms were 3.91 times more likely to return to the clinic than patients who received no Ms (p < .001). Once again, this effect is dose-responsive, as the likelihood of return gradually declines to 2.91 for patients receiving 3Ms, and 2.22 for those receiving only 1M.

Cox-Proportional hazard ratios demonstrating the rate of return clinic visits from 1 day to 1 year after index visit stratified by the number of Ms received per visit, adjusted by age group, race, gender, number of ICD-10 code diagnoses documented in patients’ electronic health record, and number of prior appointments during the study period from 2021 to 2024.
Results from the Cox Proportional Hazards Model, Calculating the Rate Ratio of a Return Clinic Visit Within a Year of the Index Visit by the Maximum Number of Ms Received, Adjusted by Age Group, Race/Ethnicity, Gender, Number of ICD-10 Code Diagnoses Documented in Patients’ Electronic Health Record, and Number of Prior Appointments During the Study Period, from 2021 to 2024.

Sensitivity analyses of both descriptive statistics and Cox proportional hazards ratios showed similar results for the distribution and likelihood of returning to the clinic after 7 days of the index visit, and after 30 days of the index visit (Supplemental Tables 1–2 and Supplemental Figures 1–6).
Discussion
Over a 3-year period, we found a consistent pattern that patients whose visits included assessment and act-ons for all 4Ms of the Age-Friendly Health Systems framework as a set, returned to the clinic at higher rates than those who did not receive all 4Ms. This finding suggests that patients may have higher levels of satisfaction of care when they receive all 4Ms as a set, and therefore are more likely to return and seek additional healthcare services at the clinic.
Patients might view the scope of convenient clinic services as limited and not use the clinic for more complicated services. An interesting finding was that diagnostic lab tests were more common in the index visits, while services that were related to gastrointestinal concerns were more common in the return visits. This may suggest that after receiving the 4Ms, trust was built, and older adults felt more confident to return for more complex care needs.
There are limitations to this study due to the use of return to the clinic as a proxy indicator of patient satisfaction. While it is well-documented that patient satisfaction is an indicator of healthcare quality, there are other factors that may play a role in the frequency of healthcare utilization and the locations chosen to receive health care.18,20 -22 For example, older age, mental health conditions, injuries, and increased number of major diseases have all been shown as factors increasing healthcare utilization. 23 It has also been observed that older adults with more chronic health conditions are more likely to receive all 4Ms, which may be an important confounder in this study. 24 This limitation is addressed by adjusting for age group, number of ICD-10-CM code diagnoses documented, and total number appointments during the study period, covariates directly related to healthcare utilization. After adjusting the Cox proportional hazards model for these covariates, the positive relationship between receiving all 4Ms and returning to the clinic was maintained.
Additionally, returning to a convenience care clinic within a relatively short amount of time after an index visit may indicate insufficient treatment or decreased quality of care, resulting in a preventable follow-up appointment. This idea may apply particularly when assessing returning to the same facility for care in a short period of time in other clinical settings, such as emergency departments. However, our sensitivity analyses which excluded visits occurring within 7 days, and within 30 days of the index visit, both yielded similar results as the main analysis in terms of showing a dose-response relationship in the hazard ratios by M count. Yet, this important consideration may limit the generalizability of this study to other clinical settings. In certain clinic settings, a patient returning to the same facility may actually indicate poor quality of care. In those cases, then it would be inappropriate assess rates of return as a successful outcome.
Conclusion
We found strong evidence of an association between receiving 4Ms care and patients returning to the convenient care health system for future care. The return to clinic outcome measure may be an objective proxy for patient satisfaction and quality of health care. Higher patient retention due to 4M care delivery may further encourage the adoption of this evidence-based model of care. Further research on the outcomes of large-scale AFHS implementation is necessary to support the expanding Age-Friendly movement. Demonstrating successes and quality improvements will enable systems to confidently decide to adopt AFHS.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241309194 – Supplemental material for Outcomes of Age-Friendly Health Systems: Return to Clinic After 4Ms Care Delivery
Supplemental material, sj-docx-1-inq-10.1177_00469580241309194 for Outcomes of Age-Friendly Health Systems: Return to Clinic After 4Ms Care Delivery by Grace Q. Armstrong, Heba M. Aldossary, Jessica Bingham, Lilia Pino, Anne Pohnert, Mary A. Dolansky and Nicholas K. Schiltz in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We would like to acknowledge Sarah Ball and Mary McCormack at MinuteClinics in select CVS Health Pharmacy locations for their expertise and work in the implementation of Age-Friendly Health Systems care, Naji Ayyash and Long Vu for assistance with coding, and the Institute for Healthcare Improvement for support and guidance.
Data Availability
The data utilized in this study are not publicly available due to private health information restrictions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the John A. Hartford Foundation. The John A. Hartford Foundation, based in New York City, is a private, nonpartisan, national philanthropy dedicated to improving the care of older adults.
Ethical Approval and Informed Consent Statements
This study has been approved as exempt, quality improvement research by the Case Western Reserve Institutional Review Board STUDY20230257.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.