
Abstract
This study aimed to measure the intention to leave and well-being indicators (ie, job satisfaction, burnout, moral distress, risk of depression, and resilience) of health care providers (HCPs) in Saskatchewan, Canada and to explore the association between their intention to leave and well-being indicators and other demographic factors, including gender. A cross-sectional study was conducted among registered nurses (RNs), physicians, and respiratory therapists (RTs) in Saskatchewan between December 2021 and April 2022. An online survey inquired about intentions to leave current positions, well-being indicators, and demographics of HCPs. Logistic regression models explored associations between intention to leave current positions and HCPs’ well-being indicators. Adjusted odd ratios (AORs) and 95% confidence intervals (95% CI) are reported. In total, 1497 HCPs participated; 38.6% considered leaving their positions. Controlling by gender, age group, children at home, redeployment, burnout, and resilience levels, the odds of considering leaving their positions decreased by 0.55 (95% CI = 0.43-0.70) per unit of increase in job satisfaction. HCPs experiencing high moral distress were more likely to consider leaving their positions (AOR = 3.97, 95% CI = 2.93-5.39). RNs were more likely to consider leaving their positions than physicians (AOR = 1.68, 95% CI = 1.13-2.50). Age interacted with gender, and burnout interacted with children at home. The job satisfaction, distress levels, and RN designation predicted HCPs’ intention to leave. We must recognize the dissimilar effect of age on the intention to leave between women and men and the effect of burnout between those with and without children. Strategies to increase retention of HCPs should consider well-being indicators and focus on reducing morally distressing environments and redeployment.
Keywords
What do we already know about this topic?
Studies around the world have studied the impact of the Coronavirus Disease 2019 pandemic on the well-being and turnover intentions of health care providers (HCPs), including nurses and physicians. However, limited studies are exploring the relationships between gender and well-being indicators when assessing HCPs’ intentions to leave their positions and few studies include respiratory therapists.
How does your research contribute to the field?
We identified that job satisfaction, distress, being redeployed, and being a nurse could predict HCPs’ intention to leave their positions and that there is a dissimilar effect of age on HCPs’ intention to leave their positions between women and men. Also, we contribute with data on the well-being and intention to leave current positions among respiratory therapists.
What are your research’s implications toward theory, practice, or policy?
Retention interventions could be targeted at nurses, redeployed HCPs, senior women, and professionals with high levels of moral distress, low job satisfaction, and symptoms of burnout. The factors associated with HCPs’ intention to leave their positions should be considered when designing health care policies that could directly or indirectly affect their retention.
Introduction
Well-being involves physical, mental, and emotional components1,2 and helps to achieve the most desirable human functioning. 1 Poor well-being of health care providers (HCPs) can be expressed in terms of emotional exhaustion, fatigue, depression, anxiety, suicide and addiction, which can seriously damage patient care and health care systems 2 and could lead to HCPs’ leaving their current positions and professions. 3
The well-being of practicing HCPs has worsened throughout the Coronavirus Disease 2019 (COVID-19) pandemic among HCPs in terms of experiencing post-traumatic stress disorder, stress, anxiety, depression, 4 and moral distress. 5 These experiences minimized effectiveness in the workplace, resulted in burnout, and caused intention to leave the profession.5,6 Physicians with high levels of fear had low job satisfaction, which was negatively associated with turnover intention. 7 Falatah reported that the turnover intention of nurses increased in a significant manner after the beginning of the COVID-19 pandemic due to burnout, low job satisfaction, and increased professional and organizational commitment. 8 Sheppard et al. found that registered nurses (RNs) had high levels of moral distress due to a lack of perceived quality of care provided to patients, a morally distressing work environment, and inadequate patient safety, leading them to consider leaving their positions. 9
Over 20% of nursing staff (ie, RNs and licensed practical nurses) in Quebec, Canada, reported high levels of fatigue, low job satisfaction, and high intention to leave their jobs or organizations. 10 Similarly, in the United Kingdom, nearly 40% of HCPs indicated they were considering leaving their jobs due to psychological strain and increasing workloads. 11 By gender, women HCPs have been more affected by the COVID-19 pandemic than men HCPs, experiencing more burnout, depression, sleep disorders, and stress. 12 In addition, women physicians struggle more in the workplace than their men colleagues, as they must maintain a balance between work and family responsibilities, causing substantial stress. 13 In a pre-pandemic study, Martinez et al. identified that being a woman is associated with the intention to leave the nursing profession. 14 Studies around the world have highlighted the effects of the COVID-19 pandemic on the well-being of HCPs and their turnover intentions.3,8,9,15 Notwithstanding, previous studies have not explored how gender and well-being indicators connect when evaluating the intention of HCPs to leave their positions.
In this study, we aimed to: 1) measure the intention to leave current positions and well-being indicators (ie, job satisfaction, burnout, moral distress, risk of depression, and resilience) of HCPs (ie, physicians, RNs, and RTs) in Saskatchewan, Canada, during the winter of 2022; 2) explore the association between HCPs’ intention to leave their current positions and their well-being indicators and other demographic factors; and, 3) explore the role of gender on the relationship between the intention to leave current positions and well-being indicators of the HCPs.
Methods
Study Design and Participants
This study was part of a mixed methods project. The first phase of the project was a quantitative study; a cross-sectional study that measured HCPs’ job satisfaction, symptoms of burnout, moral distress, risk of depression, and resilience levels, as well as their intentions to leave clinical practice. The second phase was a qualitative study that gathered perspectives on the impact of the Covid-19 pandemic on HCPs through individual interviews. 5 The results of the quantitative phase of the project are reported in this publication.
This cross-sectional study was conducted in the western Canadian province of Saskatchewan. All RNs, physicians, and RTs who were currently practicing in Saskatchewan were invited to participate in an online survey between December 2021 and April 2022. Retired RNs, physicians, and RTs, as well as those who were not practising in the province, were excluded from the study. Study participants completed a 10-minute anonymous online survey conducted via SurveyMonkey®. The study participants provided their consent prior to completing the online survey. Ethics approval was obtained from the University of Saskatchewan Behavioural Research Ethics Board (Beh-REB 3051) on November 9, 2021. Informed consent was obtained digitally from each participant at the beginning of the online survey. The completion and submission of the online survey were taken as implied consent. The STROBE cross-sectional guidelines were used for reporting. 16
Study Measures
The online survey asked about the intentions of RNs, physicians, and RTs to leave their current positions within the next 12 months. The survey also inquired about sociodemographic factors (eg, age, gender, marital status, and living with children at home) and work-related information (eg, duration of practice, location of practice, population primarily served in the practice, primary work setting and redeployment). In addition, HCPs’ well-being indicators (ie, job satisfaction, burnout, risk of depression, moral distress, and resilience) were measured using previously validated scales.
Job satisfaction of HCPs was measured using the 15-item Job satisfaction scale (JSS), a questionnaire developed based on the framework of Warr et al. 17 The items of the JSS were rated on a 5-point Likert scale (1 = very dissatisfied to 5 = very satisfied); resulting job satisfaction scores ranged from 1.00 to 5.00. 18
The single-item burnout scale was used to measure burnout. 19 Responses were scored on a five-category ordinal scale (1 = “I enjoy my work. I have no symptoms of burnout,” 2 = “Occasionally I am under stress, and I don’t always have as much energy as I once did, but I don’t feel burned out,” 3 = “I am definitely burning out and have one or more symptoms of burnout, such as physical and emotional exhaustion,” 4 = “The symptoms of burnout that I’m experiencing won’t go away. I think about frustration at work a lot,” and 5 = “I feel completely burned out and often wonder if I can go on. I am at the point where I may need some changes or may need to seek some sort of help”). 19 Then, the score of this item was dichotomized in “0 = no symptoms of burnout” if marked 1 or 2 on the scale and “1 = with burnout symptoms” if the participant reported 3, 4, or 5 on the single-item burnout scale.
The 2-item Primary Care Evaluation of Mental Disorders (PRIME-MD 2) scale was used to screen the risk of depression. 20 The items were “During the past month, have you often been bothered by feeling down, depressed, or hopeless?” and “During the past month, have you often been bothered by little interest or pleasure in doing things?.” A “yes” to either question was considered a positive test. A negative response to both questions indicated that the presence of depression was highly unlikely 20 and was dichotomized accordingly.
Moral distress was measured by the 27-item Moral Distress for Health Care Professionals instrument (MMD-HP). 21 The MMD-HP assesses five components of moral distress: involvement in unethical activities, inability to raise voice, professional values, crescendo effect (repetitive nature) of moral distress, and three levels of root causes (patient-level, unit/team-level, and system-level). The 27-item considered frequency (from “never” to “very frequently”) and level of distress (from “none” to “very distressing”), each scored using a 5-point Likert scale from 0 to 4. The frequency score and the distress score were multiplied by each other to create a composite score ranging from 0 to 16. The obtained composite scores were added together to get an overall MMD-HP score ranging from 0 to 432. 21 The scores above the observed MMD-HP mean were classified into 1 = experiencing high levels of moral distress, and the scores below the mean levels of MMD-HP were classified into 2 = experiencing low levels of moral distress. 21
The 2-item Connor-Davidson Resilience Scale (CD-RISC 2) was used to measure HCPs’ resilience. 22 The two items are: “Able to adapt to change” and “Tend to bounce back after illness or hardship.” Items are scored on a 4-point Likert scale from “Not true at all” to “True nearly all the time” during the last month. The scores of items were added, obtaining CD-RISC 2 scores ranging from 0 to 8. 22
Figure 1 shows our study variables and a conceptual model of the factors associated with the intention of HCPs to leave their positions.

Study variables and explored associations with the intention of health care providers to leave their positions.
Statistical Analysis
Means, standard deviations (SDs), medians, and interquartile ranges (IQR) were reported for JSS and CD-RISC 2 scores. The reliability of the JSS, MMD-HP, CD-RISC 2, and PRIME-MD 2 was verified by computing Cronbach’s alpha coefficients. Proportions were reported for burnout, moral distress, and risk of depression measures, and demographic characteristics. To check the randomness of missing data, Little’s missing completely at random (MCAR) test was performed. Observations with missing data points were excluded from subsequent data analysis.
Logistic regressions were used to explore the associations between the HCPs’ intention to leave their current positions and their well-being indicators and demographics. For the full HCP group, as well as for each sub-group (RNs, physicians, and RTs), unconditional analyses were conducted between the dependent variable (ie, intention to leave current positions) and the independent variables. A backward model-building strategy was used considering data of all HCPs participating in the study. In addition, models were built for RN and physician sub-groups (a multivariable regression model was not considered for RTs due to the small sample size). The final multivariable regression models included variables with P < 0.05, variables with evidence of a confounding effect, and factors with previous evidence of an association with the dependent variable. Then, interaction effects between gender identity (women/men) and the factors associated with the intention to leave the current positions were tested, as well as between children living at home and the variables in the model. Unadjusted odds ratios (UORs) and adjusted odd ratios (AORs), with their corresponding 95% confidence intervals (95% CI) were reported.
Results
In total, 1497 HCPs participated in the online survey; composed of 1053 RNs, 380 physicians and 64 RTs. In our sample, 31.9% of the participants were between 35 and 50 years and 63.6% were women. Most participants (64.4%) were married or in a common law relationship and 40.5% of the HCPs had children at home (Table 1).
Demographics and Professional Characteristics of Health Care Providers Who Participated in the Study; n (%).

The estimated response rates among RNs, physicians, and RTs were 8.4%, 13.3%, and 25.5%, respectively. These rates were calculated considering the number of practising RNs (n = 12 587), physicians (n = 2845) and RTs (n = 272) reported by the corresponding provincial professional colleges. Despite these estimated response rates, the age and gender distributions in our sample align with those observed in the target population, specifically with the demographics reported by the provincial professional colleges.23 -25
Among the HCPs participating in our study, 17.8% of them were redeployed to different positions or roles at some time during the pandemic. More than half (53.0%) of the participants had been practicing for more than ten years and 38.6% of them had intentions to leave their current positions within the next 12 months (Table 1). Among RNs, the primary practice areas were acute care (35.2%), critical care (23.3%), primary care (19.4%), long-term care (9.7%), and other areas (12.4%, eg, rural communities, advance practice, chronic disease management, patient education, etc.). Among physicians, 55.0% were family doctors, 30.7% were from medical specialties, and 14.3% from surgical specialties. Among RTs, 50.0% were working in critical care, 28.8% in general acute care, 5.7% in outpatient and community care, and 11.4% in other areas (including diagnostic and administration).
Well-being Indicators of Health Care Providers
Study participants had a high level of resilience (mean = 5.93 on a scale from 0 to 8.00) with a median of 6 (IQR = 2.00). However, HCPs were neither satisfied nor dissatisfied with their jobs (mean = 3.11 on a scale of 1.00-5.00) with a median of 3.13 (IQR = 0.93) and reported remarkably high levels of moral distress (mean = 312.62 on a scale from 0 to 432) with a median of 320 (IQR = 220). In addition, 60.3% of the participants were at risk of depression, and 71.4% had one or more symptoms of burnout (Table 2).
Well-being Indicators of Health Care Providers Who Participated in the Study; n (%), Mean (±SD), Median (IQR).

SD = standard deviation, IQR = interquartile range.
Good internal reliability levels were observed in the JSS (α = 0.89), MMD-HP (α = 0.96), PRIME-MD 2 (α = 0.80), and CD-RISC 2 (α = 0.72) scales. Regarding missing data, the Little’s MCAR test was not significant (P-value = 0.268), indicating that there was no evidence to reject the assumption that the data were missing completely at random.
Factors Associated With the Intention to Leave
The bivariate logistic regressions indicated that job satisfaction (UOR = 0.33, 95% CI = 0.27-0.41), moral distress (UOR = 5.92, 95% CI = 4.52-7.77), burnout (UOR = 2.94, 95% CI 2.18-3.95), being at risk of depression (UOR = 2.09, 95% CI 1.63-2.69), resilience (UOR = 0.83, 95% CI = 0.77-0.90), redeployment (UOR = 1.43, 95% CI 1.07-1.90), children at home (UOR = 0.59, 95% CI 0.47-0.75), and being a woman (UOR = 1.48, 95% CI 1.09-1.99) were associated with HCPs’ intention to leave their position (see table in Supplementary Material).
The final multivariable logistic model for the full group analysis included age, gender, HCP group, children at home, redeployment, job satisfaction, burnout, and level of moral distress. The final models for the RNs and physicians included age, gender, children at home, redeployment, job satisfaction, burnout, and level of moral distress. The model for physicians also included primary work settings.
Controlling by gender, age group, children at home, redeployment, burnout, and resilience levels, the multivariable logistic regression indicated that the odds of the intention to leave the current position decreased by 0.55 per unit of increase in job satisfaction (95% CI = 0.43-0.70). HCPs with high moral distress were more likely to consider leaving their positions (AOR = 3.97, 95% CI = 2.93-5.39) (Table 3).
Measures of Association Between Intention to Leave the Positions of Health Care Providers and Study Variables; Adjusted Odds Ratios (AOR) With Their Corresponding 95% Confidence Intervals (95% CI).

Note. Bold values denote statistically significant results.
Model adjusted by age, gender, HCPs group, children at home, redeployment, job satisfaction, burnout, and level of moral distress.
Model adjusted by age, gender, children at home, redeployment, job satisfaction, burnout, and level of moral distress.
Model adjusted by age, gender, children at home, redeployment, primary work setting, job satisfaction, burnout, and level of moral distress.
Variables with an interaction effect in the final model.
We also observed in the full group analysis that age interacted with gender, and burnout interacted with children at home. Older women (those in the >50 age group) were more likely to consider leaving their positions than younger women (those in the <34 age group). On the other hand, younger men (those in the <34 age group) were more likely to consider leaving their positions than men in the oldest age group (>50 years). In addition, looking within the <35 age group, younger women were less likely to consider leaving their positions than younger men. In the >50 age group, older women were more likely to consider leaving their positions than older men (Figure 2).

Probability of the intention of health care providers to leave current positions among women and men according to age groups, controlled by job satisfaction, burnout, moral distress, children living at home, health care provider group, and redeployment.
As presented in Figure 3, HCPs with symptoms of burnout were more likely to consider leaving their positions than those who did not have symptoms of burnout, and those HCPs with no children were more likely to consider leaving their positions than those with children living at home. However, the difference between those without and with children at home in the probability of considering leaving their positions was wider among HCPs with no symptoms of burnout in comparison to the gap observed in the groups of HCPs with burnout, indicating a lack of parallelism.
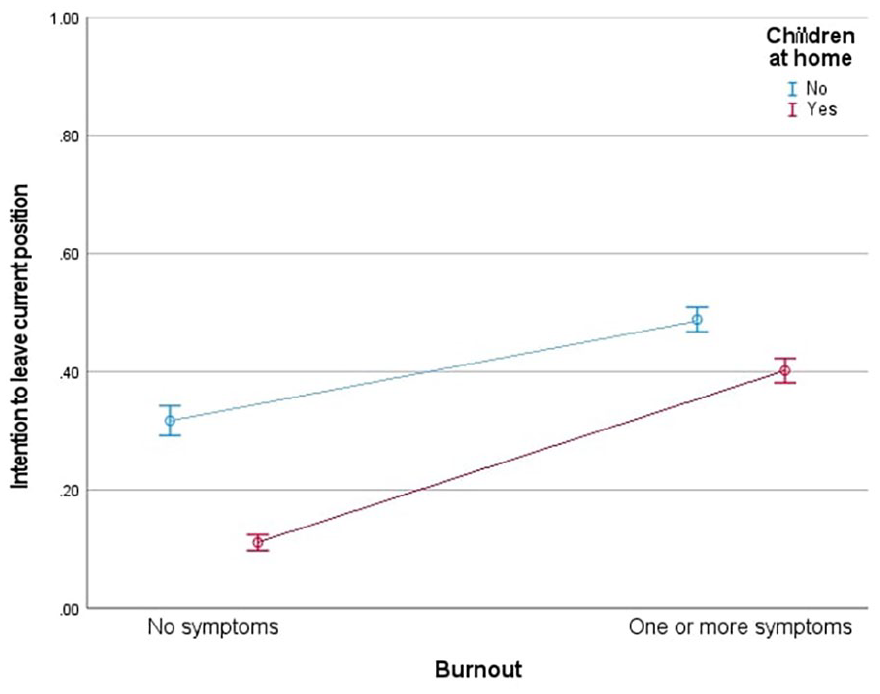
Probability of the intention to leave current positions of health care providers with and without children living at home by having symptoms of burnout, controlled by job satisfaction, moral distress, age group, health care provider group, redeployment, and gender.
In the sub-group analysis (Table 3), similar associations regarding job satisfaction and moral distress were observed in the RN and physician groups compared to the associations observed in the full group. In addition, we observed that redeployed RNs were more likely to consider leaving their positions than those who were not redeployed (AOR = 1.48, 95% CI = 1.03-2.14), and that RNs with symptoms of burnout were 1.66 (95% CI = 1.06-2.59) times more likely to consider leaving their positions than those without symptoms of burnout. On the other hand, RNs with children at home were 0.67 (95% CI = 0.48-0.93) less likely to consider leaving their positions than RNs without children. The interaction between age and gender was also observed among RNs (see figure in Supplementary Material). Among physicians, those with children at home were also less likely to consider leaving their positions than those without children (AOR = 0.67, 95% CI = 0.48-0.93). Furthermore, the odds of leaving the current positions were 2.18 (95% CI = 1.06-4.48) times higher in physicians who worked in private offices or clinics than those who worked at hospitals. No statistically significant interactions were identified among physicians.
Discussion
We observed that 38.6% of HCPs in Saskatchewan who participated in this study had intentions to leave their positions. Controlling by gender, age group, children at home, redeployment, burnout, and resilience levels, the odds of considering leaving positions decreased with increasing job satisfaction levels of the HCPs. We observed that HCPs experiencing high moral distress were more likely to consider leaving their positions. Age interacted with gender and burnout interacted with children at home. In addition, adjusting by age, gender, children at home, redeployment, job satisfaction, burnout, and level of moral distress, RNs were 1.68 (95% CI = 1.13-2.50) times more likely to consider leaving their current positions than physicians.
In our study, the proportion of RNs considering leaving their current positions was the highest (44.1%) among the three sub-groups of HCPs. A study from Quebec documented that around 30% of nurses had an intention to leave their positions during pandemic and that 22% of nurses were considering leaving their professions. 10 The proportion of intention to leave in this study and data from Quebec depict the burden of the COVID-19 pandemic on HCPs’ turnover intentions.
Nurses from Quebec, Canada, also reported that they have high levels of fatigue, low job satisfaction and higher intention to leave their jobs or organizations. 10 The reasons behind the intention to leave could be associated with an increased workload, lack of social support and fatigue, as well as a lack of rewards for HCPs’ performance. 26 In addition, we found that redeployed RNs were more likely to consider leaving their positions than those who were not redeployed during the COVID-19 pandemic. This finding aligns with data from China during the COVID-19 pandemic where 21% of nurses were redeployed and redeployment was a significant predictor of intention to leave. 15 A systematic review found that redeployment to other departments or any changes at the workplace could be linked to the increased turnover intention of HCPs based on being a new team member, being at risk of having interprofessional collaborations affected, and working within an environment where it could be challenging to ensure patient safety. 27 However, while comparisons with data from China provide a valuable context, it is important to note that Canada and China have distinct health care systems and sociopolitical environments that may influence HCPs’ experiences.
In addition, moral distress has been reported as a significant predictor of intent to leave current positions during COVID-19 among nurses in the United States. 9 We identified moral distress as a consistent factor associated with the intention to leave current positions among RNs in different primary practice areas, physicians from different specialties, and RTs during the COVID-19 pandemic. D’Alessandro-Lowe et al. reported that RTs with high moral distress were more likely to consider leaving their positions. 28 Interviews with RNs, physicians, and RTs practising in Saskatchewan, Canada, during the COVID-19 pandemic identified that HCPs experienced moral distress because of a sense of the compromised quality of care, feelings of bumping heads with authorities and patient families, and seeing family members of persons affected by COVID-19 making difficult decisions. In addition, HCPs shared during the interviews that they were experiencing burnout due to the increased expectations of patients, families, and health care managers, as well as due to unfavourable work environments, and that they recognized the need to step back. 5 Our findings and the available evidence highlight the need to monitor moral distress as a critical predictor of retention among HCPs and prevent further health human resources shortages.
Our present study also provides new evidence on the nuances of HCP well-being and intention to leave positions given the identified interactions. Regarding gender and age, women HCPs have been more affected by the COVID-19 pandemic than men HCPs. 12 Binnie et al. demonstrated that women HCPs working in Canadian intensive care units had an increased risk of developing mental health illnesses, especially among nurses rather than physicians. 29 A scoping review by Morgan et al. found that women HCPs were at an increased risk of being infected with COVID-19 and affected by mental health illness. 12 Martinez et al. identified that older age could be a protective factor in the intention to leave positions among nurses in Brazil. 14 However, an interaction effect between age and gender on the intention of HCPs to leave current positions was not previously reported in the literature. Furthermore, an association between burnout and having children was described in previous studies30,31 and Xiao et al. highlighted that there were high levels of stress experienced among HCPs during the severe acute respiratory syndrome outbreak, especially among nurses with children at home. 32 Notwithstanding, an interaction between burnout and children at home on the intention to leave current positions was not previously reported among HCPs. We must recognize the dissimilar effect of burnout on the intention to leave current positions between HCPs living with and without children.
Our study results could inform health care policy and decision-makers about some of the factors associated with the intention to leave and guide them in the development of strategies that could improve the well-being and retention of HCPs. Some strategies could include supporting mental health, fostering inclusive workplaces, or prioritization of family leaves. 33 In addition to and beyond individually focused strategies, organizational strategies are imperative to mitigate burnout and positively impact the well-being of HCPs. Specifically, the promotion of a supportive organizational culture is needed to sustainably improve the well-being of HCPs, including organizational changes that foster workload reduction, job crafting (redesigning a job and shaping task boundaries of the job), and peer networks. 34
Our study has limitations to be acknowledged. First, this study is based on data from a single province; generalization of the results to other provinces must be done with caution. Second, missing data was present, which could potentially cause a reduction of statistical power, bias in estimation parameters, and reduced sample representativeness. However, Little’s MCAR test was not significant, indicating that data were missing completely at random, and analysis could remain unbiased. Third, there is a chance of prevalence–incidence bias, as this study captured outcomes only from the winter of 2022. Prevalence incidence bias happens when a study only includes cases present at a specific time, often ignoring cases that started or resolved outside of that period. 35 Results from data obtained only in the winter of 2022 in this study may be skewed by factors that may have affected turnover intentions of HCPs at that specific point in time. In addition, respondents were those who were working during the data collection, and those who had already left their positions were not included. As a result, the outcome of this study may look less severe. Fourth, as this study was a cross-sectional study, it was also not possible to establish any causal relationship. Fifth, recall bias is another potential limitation of this study, as participants may have expressed their conditions more significantly than they experienced, leading to an overestimation of the obtained results. Sixth, the response rate was low and no sample size was estimated given that we invited all RNs, physicians, and RTs practising in the province to participate in the study. There might be a chance of selection bias due to non-response since the questionnaire was filled electronically, considering there were chances of technological difficulties, unavailability of logistics, and browser incompatibility. However, age and gender distributions in our sample align with those observed in the target population. Also, a non-response bias was tested with a brief online survey sent to non-participants. In total, 234 HCPs who did not participate in the study completed a brief survey that included demographic questions and overall items to measure job satisfaction, burnout, moral distress, risk of depression, and resilience of non-respondent HCPs. Differences between respondents and non-respondents were found to be negligible. Finally, the intention to leave positions does not necessarily mean the actual leaving of employees; so, follow-up studies could be conducted to determine the actual turnover of HCPs in Saskatchewan.
Conclusions
This study found that a considerable proportion of HCPs in the province of Saskatchewan had the intention to leave their positions during the COVID-19 pandemic, specifically in the winter of 2022. Our study revealed poor well-being indicators among Saskatchewan HCPs with major implications for their retention. HCPs’ levels of job satisfaction, distress levels, and RN designation could predict their intention to leave their positions. In the case of RNs, redeployment could predict their intention to leave their positions. We must recognize the dissimilar effect of age on HCPs’ intention to leave current positions between women and men, as well as the effect of burnout between HCPs with and without children at home. It is imperative to monitor HCPs’ well-being indicators and professional intentions. Strategies to increase retention of HCPs should focus on reducing morally distressing environments and decreasing redeployment. These findings could inform health care policies that enhance HCPs’ well-being and retention after the COVID-19 pandemic. In addition, our work and findings could apply to the context of future health emergencies and pandemics.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241306548 – Supplemental material for Health Care Providers’ Well-being Indicators are Associated With Their Intention to Leave Their Positions: A Cross-Sectional Study From Saskatchewan, Canada
Supplemental material, sj-docx-1-inq-10.1177_00469580241306548 for Health Care Providers’ Well-being Indicators are Associated With Their Intention to Leave Their Positions: A Cross-Sectional Study From Saskatchewan, Canada by Tasbeen Akhtar Sheekha, Noelle Rohatinsky, Jacob Albin Korem Alhassan, Dennis Kendel, Carmen Levandoski, Jeff Dmytrowich, Tenille Lafontaine, Matthew Cardinal and Juan Nicolás Peña-Sánchez in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580241306548 – Supplemental material for Health Care Providers’ Well-being Indicators are Associated With Their Intention to Leave Their Positions: A Cross-Sectional Study From Saskatchewan, Canada
Supplemental material, sj-docx-2-inq-10.1177_00469580241306548 for Health Care Providers’ Well-being Indicators are Associated With Their Intention to Leave Their Positions: A Cross-Sectional Study From Saskatchewan, Canada by Tasbeen Akhtar Sheekha, Noelle Rohatinsky, Jacob Albin Korem Alhassan, Dennis Kendel, Carmen Levandoski, Jeff Dmytrowich, Tenille Lafontaine, Matthew Cardinal and Juan Nicolás Peña-Sánchez in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We thank each of the health care providers in Saskatchewan who participated in the study. This study was unfunded. Although, the graduate student of the project received funding from the College of Medicine Graduate Award (CoMGRAD), University of Saskatchewan.
Author Contributions
JNPS and NR conceptualized and designed the study; JNPS and NR collected the data; TAS and JNPS analyzed the data; TAS, JNPS, NR, and JAKA interpreted the data; TAS and JNPS drafted the manuscript; and all the authors revised and approved the final manuscript for submission.
Data availability statement
The data of this study could be shared on reasonable request to the corresponding author. This data cannot be shared publicly to protect the privacy of the study participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and informed consent statements
Ethics approval was obtained from the University of Saskatchewan Behavioural Research Ethics Board (Beh-REB 3051) on November 9, 2021. Informed consent was obtained digitally from each participant at the beginning of the online survey. The completion and submission of the online survey were taken as implied consent.
Consent for publication
Not applicable
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.