
Abstract
The application of social marketing to public health activities has recently garnered attention. This study aimed to identify high-priority segments for salt reduction interventions using the TARPARE model in a rural Japanese city. This cross-sectional study used convenient sampling. Scored indicators of the TARPARE model were used, and data was collected from 1874 adults to establish the priority order of target segments for promoting salt reduction. The model considers the total number of individuals (T), at-risk persons (AR), persuasibility (P), accessibility (A), resources required (R), and equity (E). For T, the salt content was evaluated using spot urine, and the salt check sheet was scored for each segment according to sex and age in the city’s population. AR was the individuals who were overweight. P was determined by the behavior modification stage of salt reduction, unknown recommended salt reduction goals, and lack of knowledge in at least one aspect of salt reduction. A and R were characterized by communication with family or friends and family support, respectively. E was considered an education up to high school. The average aggregated score was 19.9 (standard deviation = 14.0), with higher scores in segments that consistently subjectively restrict salt intake but have a high objective salt intake. The highest priority was given to women in their 60s (49.3 points) and 70s (54.4 points). This study identified high-priority populations for salt reduction in a rural city in Japan. Our priority segments offer guidance for efficient and targeted interventions for salt reduction initiatives.
While the theory of social marketing is beneficial as a population-based approach to reducing salt intake, there have been no reported implementations in Japan, where salt intake is relatively high.
This study identified target populations for effective interventions to reduce salt intake using the TARPARE model in social marketing theory.
By identifying groups with high priority for interventions to reduce salt intake, this study provided evidence contributing to high-quality health policies and practices for salt reduction.
Introduction
As a modifiable behavior, salt reduction decreases blood pressure.1,2 The World Health Organization recommends a maximum daily salt intake of 5.0 g for adults. 3 For the Japanese population, the Japanese Society of Hypertension recommends reducing salt intake to <6.0 g per day. 4 In addition, the Government of Japan has published salt intake goals of <7.5–8.0 g and <6.5–7.0 g daily for men and women, respectively, based on the 2020 edition of the Dietary Reference Intakes for Japanese People. 5 Therefore, to prevent hypertension, promoting advocacy and achieving adherence to these national salt reduction targets is crucial in public health activities.
Social marketing emerged in 1971 to address social problems, including public health and has since gained significant attention as a population approach. 6 Social marketing is the application of commercial marketing technologies to the analysis, planning, execution, and evaluation of programs designed to influence the voluntary behavior of target audiences to improve their welfare and that of society. 7 Social marketing is widely used to influence health behaviors as a framework for population approaches. 8 The Pan American Health Organization reported on supporting national, regional, and local social marketing strategies for salt reduction, 9 enabling the consideration of population-level strategies for salt reduction. Many studies use social marketing interventions for salt reduction10 -14; however, such studies are yet to be conducted in Japan.
In social marketing, segmenting the target group helps select the intervention target group and develop tailored intervention methods to promote healthy eating behaviors. 15 Identifying a specific target group has the potential to enhance the effectiveness of interventions, such as salt reduction, by concentrating resources more intensively. Therefore, it is necessary to first identify the target group for interventions in the social marketing process. This approach identifies specific individuals or groups as target audiences, analyzes the target group’s behavior, and devises effective intervention strategies. In public health, the TARPARE model has been reportedly used to identify target groups.16,17 The TARPARE model is a practical and adaptable framework for comprehending segments within a target population and for assessing the potential effectiveness of interventions aimed at each segment. The assessment of each segment can be allocated both qualitatively and quantitatively through scoring. Out of five studies using social marketing, all identified the segment characteristics of the intervention targets.10 -14 The effect of the intervention has been reported by a reduction in the intervention group in three studies that evaluated salt intake.10,11,14 However, to the best of our knowledge, there have been no studies that reported the use of the TARPARE model to identify high-priority segments for salt reduction interventions.
Therefore, in this study, we primarily aimed to identify a target group that needs the prioritization of salt reduction interventions by utilizing the TARPARE model.
Methods
Study Participants
This cross-sectional study conducted data sampling using a convenience sampling method on participants who underwent health examinations between August and November 2019 and August and November 2022. Municipalities administer annual health examinations at health centers in communities, which are available yearly for residents aged ≥40 years who are covered by the National Health Insurance. We sought voluntary participation from residents who underwent health examinations without offering any incentives. Written informed consent was obtained from all participants before study enrollment. The inclusion criteria included engagement in a health examination and consent to contribute to our survey and excluded those who did not provide consent. This study included 1874 adults (750 and 1124 participants comprising 48.8% and 44.1% men in 2022 and 2019, respectively).
This study followed the Declaration of Helsinki and received approval from the Medical Research Ethics Committee of the Shimane University Faculty of Medicine (Approval number: 20051214-3).
Salt Intake Parameters
Data regarding salt intake were collected from an additional health survey during the health examinations. The salt intake (estimated 24-h salt intake) was calculated using the formula proposed by Tanaka et al, 18 which was developed for large epidemiological studies. The computation revealed a weak correlation between estimated sodium on spot urine analysis and actual sodium excretion measured using the 24-h urine collection analysis. The target salt intake of ≤8 g for men and women recommended by the Shimane prefecture government agency was adopted as the cutoff, 19 as often used by Japanese municipalities.
A high-salt diet and eating behavior were assessed using the salt check sheet.20,21 Thirteen questions were scored from 0 to 3 points per question, totaling 35 points. Participants were categorized as having low-salt behaviors (≤13 points) or high-salt behaviors (≥14 points) based on a previous study. 20
The behavior modification stage of salt reduction was determined based on the questions of Prochaska et al 22 and Tamaki et al 23 The questionnaire asked, “Are you currently trying to reduce the amount of salt in your diet?” Participants responded on a scale of 1 to 4 (1 = “definitely no” to 4 = “definitely yes”). Those who selected responses 1 to 3 and indicated that they were “not planning to start salt reduction in the next 6 months or more” were classified as “pre-contemplation.” If they intended to start the reduction within the next 6 months, they were considered “contemplation.” “Preparation” was defined as “intending to begin within the next month.” For those who responded 4, we inquired about the duration. “Having done so for <6 months” was classified as “action” and “≥6 months” as “maintenance.”
Regarding social support for salt reduction,24,25 participants were asked, “Does your family support a low-salt intake?” The evaluation was made on a 5-point scale from “because they will not do it” to “they will do it.” As a measure of communication regarding salt reduction, participants were asked, “Have you ever talked about salt reduction with your family or friends?” Moreover, it was evaluated on a 5-point scale from “no” to “yes.” Regarding knowledge about salt reduction, we assessed the following questions based on a previous study 26 ; “Do you know the recommended amount of salt intake per day for adults?” Participants answered with either a “yes” or a “no.” In addition, participants were asked 7 questions individually developed regarding specific knowledge of salt reduction, which included the following: “Do you know you get most of your daily salt intake from seasonings?”; “Do you know that [salt equivalent] is listed on many foods?”; “Do you know that eating vegetables helps to expel salt from your body?”; “Do you know that even if you reduce the amount of salt, it tastes good?”; “Do you know that ‘usukuchi’ (light) soy sauce contains more salt than ‘koikuchi’ (dark) soy sauce?”; “Do you know that even a light taste can increase the amount of salt if you eat a lot?”; and “Do you know that dashi stock contains salt?” All questions were answered with either “yes” or “no.” In this study, we calculated the number of “yes” answers among the 7 salt reduction questions and categorized the participants into 2 groups based on whether they had knowledge about all the questions asked.
Additional Parameters
This study collected information on sex, age, and body mass index (BMI) from the health examinations. Data on sex (men or women), age (years, continuous), and BMI were included in the 2022 survey. Educational attainment data were included in our own survey conducted in 2019 in accordance with health examinations. Although educational attainment was not included in the 2022 survey, the most recent data was collected in 2019. Therefore, data from that year were used for the analysis. The BMI was calculated from recorded height and weight (kg/m2), dividing participants into 2 groups (underweight and normal weight: <24.9 kg/m2 and overweight: ≥25.0 kg/m2). This study used BMI as a surrogate variable for total energy intake. Educational attainment was categorized into 2 groups (high school graduates and above).
Statistical Analysis
Descriptive statistics were calculated for all variables. Categorical variables are expressed as numbers and percentages.
The TARPARE model was used for scoring using the following parameters (Table 1). 17 The total number of individuals in the segment (T) was calculated using the 2021 Unnan city demographic information. This study was performed to identify priority segments for salt reduction interventions among the population of Unnan City, Shimane Prefecture, Japan, which consists of 11 495 men and 12 214 women aged 40 to 89 years. The segments were divided based on sex and 10-year units for age; in the population aged 40 to 89 years, 11 495 men and 12 214 women were included. The estimated proportion in each population segment was statistically inferred from the proportion of parameters (salt behavior, salt intake, being overweight, preparation, unknown salt reduction goals, unknown salt reduction knowledge, family support, communication about salt reduction with family or friends, and lower educational attainment). The items corresponding to each model were selected from the data we collected. The proportion of each parameter within the segment was calculated after excluding the missing data.
Items in TAPARE Methods and This Study Parameters.
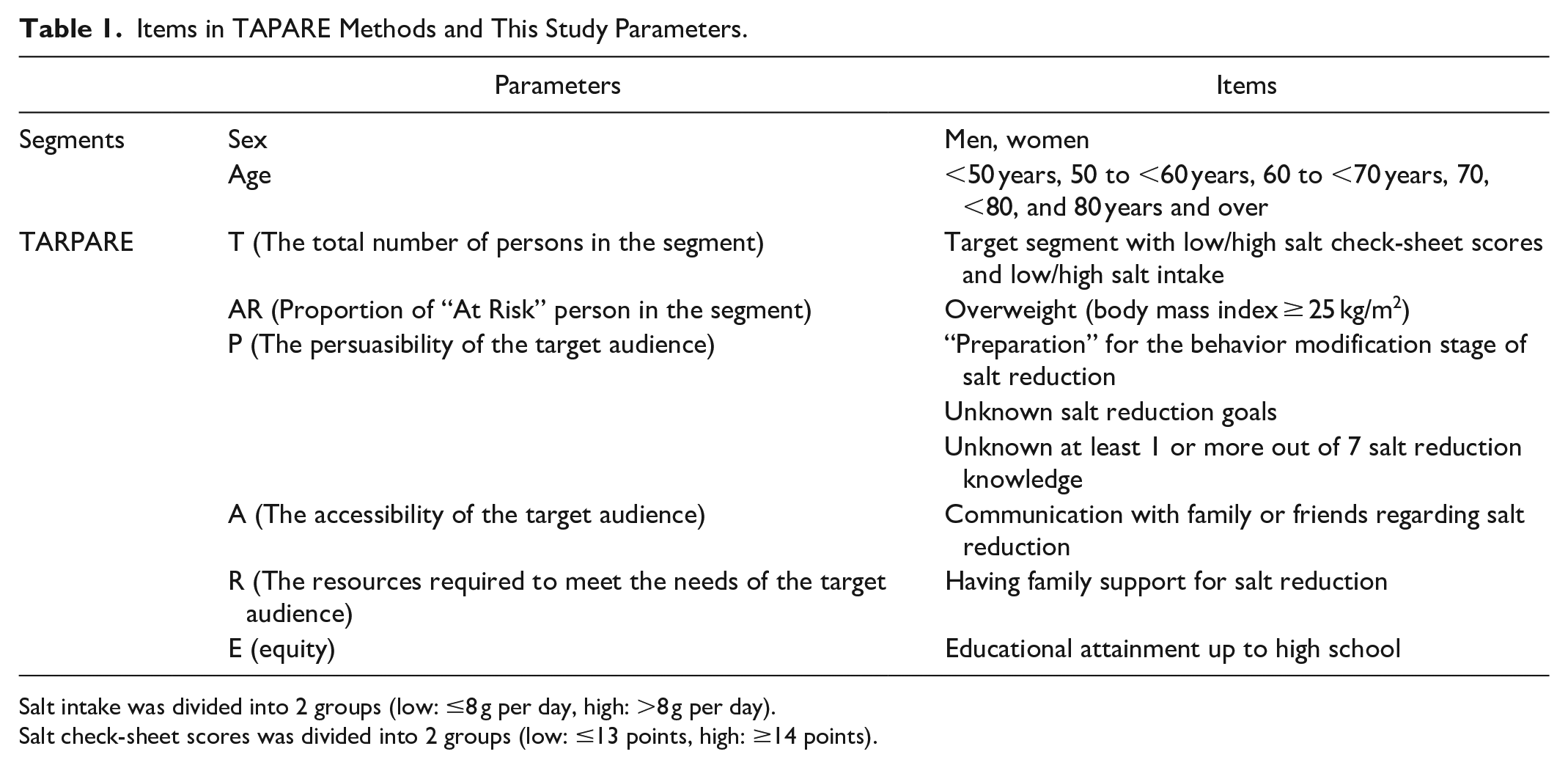
Salt intake was divided into 2 groups (low: ≤8 g per day, high: >8 g per day).
Salt check-sheet scores was divided into 2 groups (low: ≤13 points, high: ≥14 points).
The following are the items used for the TARPARE score calculation in this study. First, a previous study has reported a gap between perception and action, wherein approximately >60% of individuals attempted to reduce their current salt intake, but only 13% believed that they were consuming salt excessively. 27 Thus, we created a combination variable for groups with high or low scores on the salt check sheet (four groups), investigated whether the estimated salt intake met the Shimane Prefecture’s target goal of ≤8 g/day, and examined each segment’s proportion. The proportion of “At Risk” persons in the segment (AR) was calculated using the overweight factor. The persuasibility of the target audience (P) was used as the “preparation” for the behavior modification stage for salt reduction, unknown recommended salt reduction goals, and unknown salt reduction knowledge. For the accessibility of the target audience (A), communication with family or friends regarding salt reduction was considered. Regarding the human resources required to meet the needs of the segment, the resources required to meet the needs of the target audience (R) were associated with family support for salt reduction. Based on a previous study indicating that low education status as socioeconomic status was associated with high salt intake, 28 educational backgrounds up to high school were considered for equity (E).
The segment priority score was calculated using the following formula:

While the specific weight (w) for each parameter was not explicitly provided, in this study, w1 was assigned a value of 4, w2 a value of 3, and w3 to w5 were each set to 1. The segment priority score was calculated based on all of these items and their weighted formulas, encompassing the total points. From the segments with high total points, we identified the groups with a high priority for salt reduction interventions.
Results
Table 2 represents the characteristics of the study participants. A total of 222 (29.6%) participants had a high salt intake based on the salt check-sheet score, and 522 (69.6%) had a salt intake >8 g based on spot urine measurements. In total, 350 participants had low salt behaviors and high salt intakes (46.7%).
Characteristics of the Study Participants.

Educational attainment was data (n = 1124) from survey in 2019.
Table 3 and Supplemental Table 1 represent the results obtained using the TARPARE model. The average aggregated segment priority score (standard deviation) was 19.9 (14.0), with higher scores in segments that consistently subjectively restrict salt intake but have a high objective salt intake. The findings can be summarized as follows: the group with the highest segment priority score (54.4 points) comprised women in their 60s, specifically those with high salt intakes and low scores on the salt check sheet. The second-highest group (segment priority score = 49.3 points) included women in their 70s with high salt intakes and low scores on the salt check sheet. The third-highest group (segment priority score = 44.7 points) included men in their 60s, who had high salt intakes and low scores on the salt check sheet.
Population Priorities for Salt Reduction Interventions Assessed by the TARPARE Model.

From the segments with high total points, we identified the groups with a high priority for salt reduction interventions.
Discussion
This study identified women in their 60s and 70s as the target group using the TARPARE model. This underscores the need to prioritize salt reduction interventions within this specific group. This finding aligns with that of previous research on middle-aged and older women in a social marketing-based salt reduction intervention study. In Japan’s population pyramid, individuals in their 60s and 70s belong to the first baby boom generation, making up a relatively significant proportion of the population. 29 Targeting this specific demographic through a population-based approach can potentially have an impact at the community level. A previous study examining the effects of a social marketing theory-based diet education program on the dietary status of older women showed reduced sodium intakes within the intervention group. 10 This study used 2 diet education materials developed based on the preferences of older adults. Therefore, it is crucial to employ materials that effectively resonate with the intended population. Moreover, with their traditional roles and responsibilities, mothers and housewives may have personal motivations to provide healthy meals for their families,12,29 thereby affecting family health. Therefore, interventions directed toward women in their 60s and 70s to reduce salt intake may have secondary benefits that extend to larger populations, including families.
The National Social Marketing Centre has proposed 8 benchmark criteria to understand how to use core social marketing concepts effectively, including behavior, customer orientation, theory, insight, exchange, competition, segmentation, and mixed methods. 30 Our study applied the TARPARE model, based on segmentation following these social marketing benchmark criteria. 17 Implementing salt reduction interventions in communities should consider these 8 criteria and social marketing strategies. Focusing on specific eating behaviors has been highlighted in previous reviews of behavioral changes associated with social marketing. 15 When considering behavioral changes regarding salt reduction, the specific behavior of the target population should be examined. Thus, the upcoming challenge is to gain a comprehensive understanding of salt reduction behavior and its related products, prices, locations, and promotions based on the social marketing mix among the target population by combining qualitative and quantitative data.9,31 As for previous studies applying social marketing to reduce salt, 2 studies qualitatively defined the segment characteristics based on demographic variables through interviews,10,12 1 study categorized it into behavior change stages using a questionnaire, 13 and 2 studies identified it both qualitatively and quantitatively.11,14 All of them conducted a KAP Study (Knowledge, Attitude and Practices Study) for quantitative evaluation, 32 not the TARPARE method. In this study, the TARPARE model was used for quantitative evaluation, and one of its indicators used the behavior change stage, which is common. Among the 3 studies that evaluated salt intake as an intervention effect, 2 studies using quantitative and qualitative evaluation recognized a decrease in the intervention group and an interaction with the control group.11,14 A previous study using qualitative evaluation reported a decrease in the intervention group. 10 Since we did not perform qualitative evaluation through interviews, the next step involves exploring the target through quantitative and qualitative research. Furthermore, employing social marketing to formulate strategies for a population-based approach to reduce salt intake is essential.
This study used objective (spot urine tests) and subjective (salt intake check sheets) indicators to assess salt intake. By combining these indicators, we focused on individuals who believed they were reducing their salt intake but did not meet objective targets. Bridging the gap between perception and action is essential, 27 and future studies should explore methods to achieve this, such as delivering tailored salt reduction messages based on individual characteristics. 13 The cutoff value for salt intake was set at ≤8 g for adults aged 20 to 79 years, following the health promotion plan of Shimane Prefecture, 19 the region of interest. Considering approximately 30% of the participants have achieved a salt intake of ≤8 g in this study area, achieving these targets poses challenges that require additional efforts. Consequently, if the new targets proposed by Healthy Japan 21 (Third Term) starting in 2024 (7 g), the World Health Organization (5 g), or the Japanese Society of Hypertension (6 g) were adopted as the cutoff values,3,4,33 there is a possibility that the target population segment would change. In future interventional studies, it will be necessary to conduct a segmented analysis based on the targeted levels of dietary salt intake. Moreover, adhering to the recommended salt intake levels to prevent cardiovascular diseases such as hypertension is crucial. However, considering the current average salt intake for Japanese individuals aged ≥20 years of 10.1 g. 34
This study had several limitations. First, due to the cross-sectional study design, this study could not explain causal relationships. Second, we used data gathered from participants who were residents of a single local city and those who underwent health examinations using convenient sampling, which restricted the generalizability of our findings. After completing the data collection, we calculated the sample size and observed that the size of our study samples was smaller than the calculated sample size (see Supplemental Table 2). Consequently, this discrepancy could potentially lead to an underestimation or overestimation of the proportions within each segment. In particular, the limited number of participants aged <60 years resulted in significant variation in the obtained results, and the small sample size may have affected the reliability of the research findings. Therefore, when interpreting the results, it is crucial to acknowledge the limitations imposed by the small number of participants aged <60 years and exercise appropriate caution. Third, this study utilized data acquired in 2022 for many variables, except educational background, for which data from 2019 were used. This decision was made considering that socioeconomic factors can influence participants’ eating behaviors. Data from 2022 were used to determine the most recent status of participants as much as possible; however, it is essential to be mindful of the ongoing coronavirus disease 2019 pandemic when interpreting these results. Fourth, the measurement error for salt intake was considerable due to the use of spot urine samples. However, conducting a 24-h urine collection at the population level can be challenging; therefore, this study adopted a more convenient approach. Fifth, the questionnaire (see Supplemental File) used in this study lacked validation for reliability and validity, which may have affected its consistency during repeated measurements and with content validity in relation to the survey objectives. Therefore, these points should be considered when interpreting the survey results. Sixth, although we could not consider unmeasured factors (blood pressure, types and medications, and history of serious diseases and their durations). Finally, the items corresponding to the TARPARE model were selected from the data we collected. Potential confounders may influence the salt reduction behaviors.
Conclusions
The TARPARE model was used to identify the high-priority populations for salt reduction. Women in their 60s and 70s were given the highest priority. Therefore, developing strategies based on social marketing theory will be necessary in future studies on salt reduction interventions.
Implications for Practice
As a global public health issue, promoting salt reduction is crucial for preventing hypertension. In this study, we examined a target group for a population-based approach to salt reduction in community settings. Specifically, we investigated which target group should be the focus of intervention using the TARAPARE model. The results indicated that targeting 60- and 70-year-old women residing in Japanese community areas would be beneficial for promoting salt reduction. This practical approach has the potential to efficiently allocate resources. Furthermore, by advocating evidence-based policies, we can contribute to future community intervention research on salt reduction.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241282776 – Supplemental material for Identifying High-Priority Populations for Dietary Salt Reduction Using the TARPARE Model: A Cross-Sectional Study
Supplemental material, sj-docx-1-inq-10.1177_00469580241282776 for Identifying High-Priority Populations for Dietary Salt Reduction Using the TARPARE Model: A Cross-Sectional Study by Takafumi Abe, Jun Kitayuguchi, Tsuyoshi Hamano, Masayuki Yamasaki, Shozo Yano and Minoru Isomura in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-xlsx-1-inq-10.1177_00469580241282776 – Supplemental material for Identifying High-Priority Populations for Dietary Salt Reduction Using the TARPARE Model: A Cross-Sectional Study
Supplemental material, sj-xlsx-1-inq-10.1177_00469580241282776 for Identifying High-Priority Populations for Dietary Salt Reduction Using the TARPARE Model: A Cross-Sectional Study by Takafumi Abe, Jun Kitayuguchi, Tsuyoshi Hamano, Masayuki Yamasaki, Shozo Yano and Minoru Isomura in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-xlsx-2-inq-10.1177_00469580241282776 – Supplemental material for Identifying High-Priority Populations for Dietary Salt Reduction Using the TARPARE Model: A Cross-Sectional Study
Supplemental material, sj-xlsx-2-inq-10.1177_00469580241282776 for Identifying High-Priority Populations for Dietary Salt Reduction Using the TARPARE Model: A Cross-Sectional Study by Takafumi Abe, Jun Kitayuguchi, Tsuyoshi Hamano, Masayuki Yamasaki, Shozo Yano and Minoru Isomura in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors greatly appreciate the cooperation of the study participants and Shimane CoHRE study members for their assistance. We would like to express our heartfelt gratitude to all health officials at Unnan City Hall for their tremendous support.
Author Contribution
TA and JK designed the study. TA, MY, and MI collected the data. TA drafted the manuscript and analyzed the data. JK, TH, and SY reviewed the paper. All authors reviewed and approved the manuscript.
Data Availability
This study’s protocol, including the consent of the subjects, was approved by the ethics committee of Shimane University. The consent of the participants did not include a provision for the data to be shared publicly.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Statement
This study followed the Declaration of Helsinki and received approval from the Medical Research Ethics Committee of the Shimane University Faculty of Medicine (Approval number: 20051214-3, Date: August 28, 2020). Written informed consent was obtained from all participants before study enrollment.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.