
Abstract
Patient participation is considered important for the safety and quality of care. The patient’s perception of actually being able to participate in healthcare, namely, the sense of participation, may influence patient satisfaction (PS). This study aimed to quantitatively determine the relationship between sense of participation to healthcare and PS. A questionnaire survey was conducted among 100 inpatients from each of the 5 target hospitals. The questionnaire included 6 PS items and 4 patient achievement goals, which were indicators of whether the patients had a sense of participation. The response rate was 60.6% (303/500). Patients who perceived that they could choose a treatment that reflected their values and wishes had significantly higher scores on all PS items. Patients who achieved the goal of “I want to be a member of the medical team and participate actively in treatment and safety activities” showed significantly higher PS related to coping to reduce pain and symptoms. Additionally, patients who achieved the goal of “I believe I am able to voluntarily learn about the disease/treatment and use it to make decisions” had significantly higher PS related to psychological support. Sense of participation may improve PS in a wide range of areas. Hospitals and healthcare workers are expected to empower patients to develop a sense of participation.
Keywords
Although several findings have shown that hospital initiatives regarding patient-centered care and shared decision-making increase patient satisfaction, no studies have demonstrated a relationship between “sense of participation” and satisfaction.
This study provides quantitative data on the relationship between patient participation and patient satisfaction for as many as 303 participants; specifically, there has been no previous finding that a patient’s sense of participation, rather than hospital activities or patient experience, improves patient satisfaction.
It was suggested that hospitals and healthcare providers could help patients develop a sense of participation, which could attract hospital customers, improve patient adherence to treatment, and ultimately improve treatment outcomes.
Introduction
Recently, there has been a growing focus on the importance of patient and family participation in healthcare.1-5 The Tokyo Declaration on Patient Safety, adopted at the third Global Ministerial Summit on Patient Safety in April 2018, indicated the importance of engaging and empowering patients and families in the delivery of safe and quality care and all aspects of healthcare. 6 According to the often-cited definition by Carman et al, patient participation is the active partnership of patients, families, their representatives, and healthcare workers at various levels across the health care system—direct care, organizational design and governance, and policy making—to improve health and health care. 1 The scope of patient participation is broad and includes participation in healthcare safety, hospital administration, and policy making.1,3,7-10 In this article, the term “patient participation” is used primarily; however, the term “patient engagement” is often used with the same meaning.10,11
Patient satisfaction (PS) is a tool widely used to measure the quality of care. One of the benefits of patient participation is said to be increased PS. Actually, previous studies on the relationship between patient participation and PS have shown that PS improves when hospitals implement activities related to shared decision-making and patient-centered care.12,13 PS is expected to play a role in increasing the patient involvement in the healthcare process as well as in the hospital’s customer acquisition and business success objectives. 14 It has also been suggested that higher PS improves patient adherence to treatment. 15
The AHRQ report cites self-efficacy as a factor that promotes patient participation, in addition to the provision of information and invitation and support for participation by healthcare workers. 16 In this article, we refer to a patient’s self-efficacy regarding their participation in healthcare, that is, the perception that he or she has the ability to achieve, or has actually achieved, participation in healthcare, as “sense of participation.” Although there were studies that measured the relationship between PS and the implementation of services provided by hospitals and patients’ experience of participating in healthcare,17-22 there were no studies that showed a relationship between PS and the sense of participation. PS may increase by giving patients the sense of participation. This study aimed to quantitatively determine the impact of whether or not patients have the sense of participation on PS by a questionnaire survey.
Methods
Study Design
This exploratory research project on patient participation, targeting inpatients in Japan, ran from April 2021 to March 2022. We conducted a questionnaire survey among patients admitted to a hospital in January 2022. Written informed consent was obtained from participants at the time the survey was administered. This study was supported by the Health Labour Sciences Research grant number JPMH20IA1009. There are no other conflicts of interest in this study. This study was approved by the Ethics Committee of the All Japan Hospital Association (approval number: R2-001; December 13, 2021).
Study Population
A total of 500 inpatients (100 each) from 5 Japanese hospitals were included in the study. Sample size was not calculated in this study. The target hospitals were selected for convenience from members of the All Japan Hospital Association, of which approximately a quarter of the 8372 hospitals in Japan were members, mainly private hospitals. Hospitals with more than 200 beds, functioning as acute-care hospitals, and actively engaged in activities to promote patient safety were approached individually to obtain their consent. Eligible patients were those admitted to the general ward of the target hospitals who were able to understand and respond to the questionnaire, either by themselves or through a proxy. Patients admitted long-term care wards, psychiatric wards, and infectious disease wards, as well as those deemed unable to understand or complete the questionnaire, were excluded. The selection of patients to respond to and the methods of distribution were left to the hospitals. When collecting the questionnaires, the patients sealed them in envelopes, and only a predetermined person in charge opened the envelopes and tabulated the data.
Questionnaire
A questionnaire was developed for inpatients that asked about PS and the success or failure of achieving the “Patient Achievement Goals” for the sense of participation. The items on PS and patient achievement goals are listed in Table 1.
The List of Questionnaire Items.

Answer on a 4-point Likert scale: “Agree,” “Somewhat agree,” “Somewhat disagree” and “disagree.”
Compliant with the “Patient Satisfaction Survey” by the Japan Council for Quality Health Care. Except for S6, answer on a 5-point Likert.
Overall satisfaction. Answer on a 5-point Likert scale: “Recommend,” “Somewhat recommend,” “Neutral,” “Somewhat do not recommend” and “Do not recommend.”
Four patient achievement goals were established based on previous studies1-5,7-9 as the state in which the patient obtained the preferred sense of participation. Carman et al cite patient participation at the direct care level as the patients receive appropriate information, make their own decisions, and are active partners in the medical team. 1 Therefore, the former was set as patient achievement goals G1 “I was able to choose a treatment plan that reflected my values and wishes,” and the latter as G2 “I want to be a member of the medical team and participate actively in treatment and safety activities.” In addition, G3 “I believe I am able to voluntarily learn about the disease/treatment and use it to make decisions” was set as a state in which the patients voluntarily learn about their own disease and treatment in order to participate in healthcare, and G4 “I can speak up if I feel something is dangerous” was set as a state in which the patients can communicate risks to healthcare workers when they become risk discoverers.
PS was measured using the “Patient Satisfaction Survey” provided by the Japan Council for Quality Health Care (JQ), a not-for-profit organization that provides hospital accreditation programs and maintains nationwide incident reporting systems for patient safety. The “Patient Satisfaction Survey” is being widely used in Japanese hospitals to assess the quality of care. 23 The “Patient Satisfaction Survey” has an inpatient survey and an outpatient survey, and the inpatient survey was used in this study. The “Patient Satisfaction Survey” is supposed to be used by hospitals to select up to 20 items from a list of 60 items. In particular, the JQ has been conducting a benchmark survey of 11 basic items, allowing for comparison with the results of other Japanese hospitals. Among the basic items, 6 items (S1-S6 in Table 1) considered relevant to patient participation were selected and used as PS for this study. The items “Recommend this hospital to a friend,” which corresponds to S6 in this study, is regarded as an item that measures the overall satisfaction.
The questionnaire was designed to allow respondents to answer on a 4-point Likert scale (“4: Agree”–“1: Disagree”) whether they felt they had achieved the 4 patient achievement goals. PS followed the “Patient Satisfaction Survey” response format specified by the JQ: the participants responded to S6, the overall satisfaction, on a 5-point Likert scale (“5: Recommend”–”“1: Do not recommend”) and to all other items on a 5-point Likert scale (“5: Strongly satisfied”–”“1: Strongly dissatisfied”).
The PS results were not only simply tabulated, but also evaluated on mean scores on a 5-point Likert scale to compare with the results of the “Patient Satisfaction Survey” benchmarking project provided by the JQ, in which 293 Japanese hospitals participate.
Statistical Analysis
A binomial logistic regression analysis was performed to examine the relationship between PS and patient achievement goals. For analysis, both patient achievement goals and PS were categorized into 2 groups of responses and treated as categorical variables. The items for patient achievement goals were categorized as “Achieved” for “4: Agree” and “3: Somewhat agree,” and “Unachieved” for “2: Somewhat disagree” and “1: Disagree.” S6 of PS, which is the overall satisfaction, was categorized as “satisfied” for “5: Recommend ” and “4: Somewhat recommend,” and “dissatisfied” for “3: Neutral,” “2: Somewhat do not recommend,” and “1: Do not recommend.” PS other than S6 was categorized as “Satisfied” for “5: Strongly satisfied” and “4: Satisfied,” and “Unsatisfied” for “3: Neutral,” “2: Dissatisfied,” and “1: Strongly dissatisfied.” “No use of the service” was excluded from the analysis. The PS items (satisfied/dissatisfied) were set as objective variables, patient achievement goals (achieved/unachieved) were explanatory variables, and hospital, patient sex, and age were adjusted variables. Respondents under 20 years of age were excluded. The significance level was set at P < 5%.
Results
Hospitals and Participants
The 5 surveyed hospitals had a minimum of 224 beds and maximum of 331 beds, with 4 acute-care hospitals and 1 hospital with both acute and chronic functions. These hospitals were located: 1 in Tokyo, 3 in small- and medium-sized cities in the suburbs around Tokyo (two in Saitama Prefecture, and one in Ibaraki Prefecture), and 1 in a residential area near Nagoya, Aichi Prefecture. The questionnaire response rate was 60.6% (303/500). The characteristics of the participants are shown in Table 2.
Characteristics of the Participants.

Percentages are presented as values excluding “No answer.”
Patient Achievement Goals and PS Scores
Table 3 shows the simple tabulation of the responses regarding the achievement of patient achievement goals for a sense of participation. The percentages were calculated excluding “Not answered” responses. Approximately 80% of patients responded “4: Agree” or “3: Somewhat agree” to all 4 patient achievement goals. Table 4 presents the simple tabulation of the responses to PS. The percentages were calculated excluding “No use of the service” and “Not answered” responses. Approximately 85% of the respondents were “5: Strongly satisfied” or “4: Satisfied” with S1, “Examination and treatment by physicians,” S2, “Dialog with physicians,” S3, “Support by nurses,” and S4, “Coping to reduce pain and symptoms. S5, “Psychological support,” was also answered positively by 75.6% of the respondents. In S6, “Recommend this hospital to family and friends,” the overall satisfaction, 78.6% of the respondents answered “”5: Recommend” or “4: Somewhat recommend,” 19.1% answered “3: Neutral,” and 1.4% answered “2: Somewhat do not recommend” or “1: Do not recommend.” On the 5-point Likert scale, the mean scores were 4.43 in S1, 4.35 in S2, 4.48 in S3, 4.34 in S4, 4.20 in S5, and 4.23 in S6, respectively.
Results of the Questionnaire Survey: Patient Achievement Goals for Sense of Participation (n = 303).
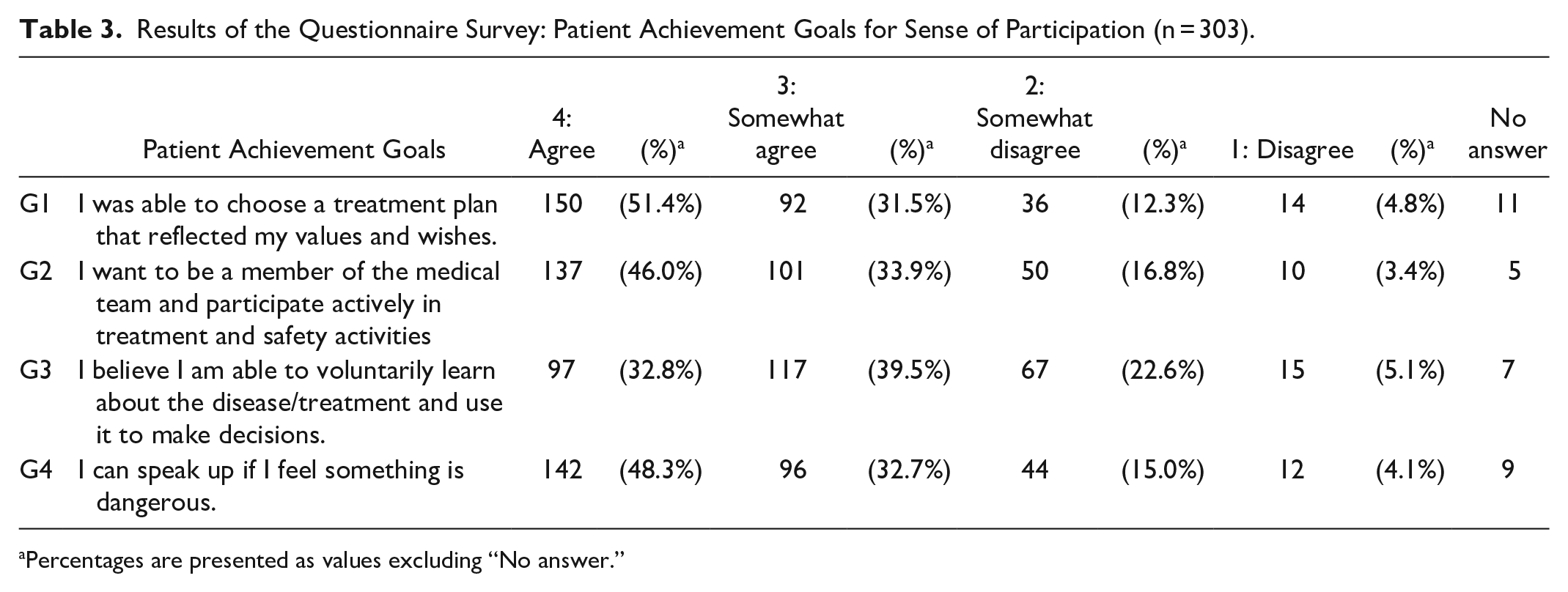
Percentages are presented as values excluding “No answer.”
Results of the Questionnaire Survey: Patient Satisfaction (PS) in This Survey of Five Hospitals (n = 303).
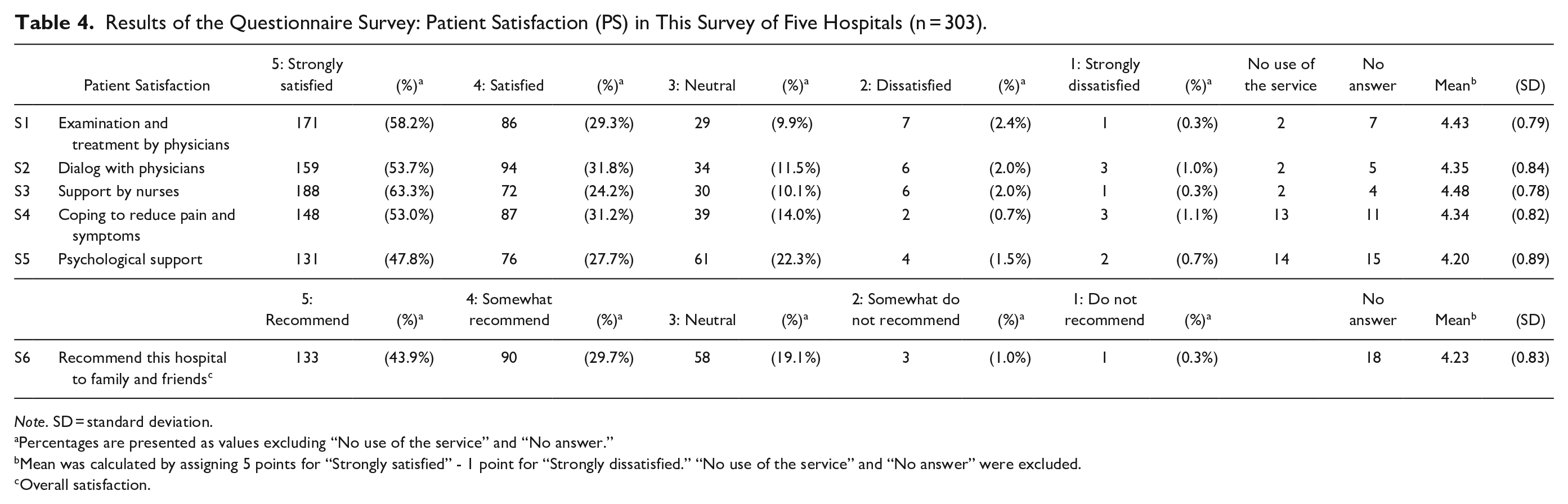
Note. SD = standard deviation.
Percentages are presented as values excluding “No use of the service” and “No answer.”
Mean was calculated by assigning 5 points for “Strongly satisfied” - 1 point for “Strongly dissatisfied.” “No use of the service” and “No answer” were excluded.
Overall satisfaction.
Relationship Between Patient Achievement Goals and PS
The results of the binomial logistic regression analysis of patient achievement goals for the sense of participation and PS are shown in Table 5. Patient achievement goal G1 “I was able to choose a treatment plan that reflected my values and wishes” was significantly associated with “satisfied” in all PS items. In particular, the odds ratio between G1 and S1/S2 was high (S1, adjusted odds ratio (aOR) = 16.73; S2, aOR = 13.67). G2 “I want to be a member of the medical team and participate actively in treatment and safety activities” was significantly related to S4 “Coping to reduce pain and symptoms” (aOR = 4.08). G3 “I believe I am able to voluntarily learn about the disease/treatment and use it to make decisions” was significantly related to S5 “Psychological support” (aOR = 2.46).
Binomial Logistic Regression Analysis: Relationship Between Patient Achievement Goals for Sense of Participation and Patient Satisfaction (PS).
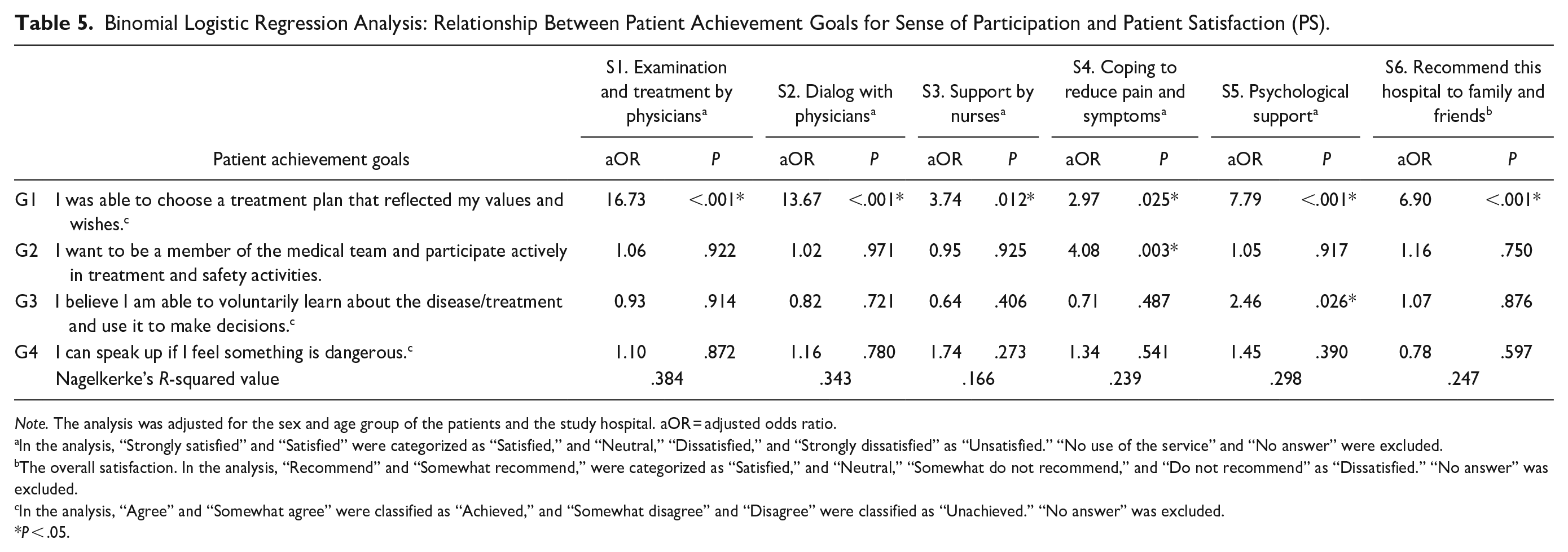
Note. The analysis was adjusted for the sex and age group of the patients and the study hospital. aOR = adjusted odds ratio.
In the analysis, “Strongly satisfied” and “Satisfied” were categorized as “Satisfied,” and “Neutral,” “Dissatisfied,” and “Strongly dissatisfied” as “Unsatisfied.” “No use of the service” and “No answer” were excluded.
The overall satisfaction. In the analysis, “Recommend” and “Somewhat recommend,” were categorized as “Satisfied,” and “Neutral,” “Somewhat do not recommend,” and “Do not recommend” as “Dissatisfied.” “No answer” was excluded.
In the analysis, “Agree” and “Somewhat agree” were classified as “Achieved,” and “Somewhat disagree” and “Disagree” were classified as “Unachieved.” “No answer” was excluded.
P < .05.
Discussion
This questionnaire survey of inpatients at 5 hospitals revealed a positive and significant relationship between PS and several patient achievement goals for a sense of participation. In particular, patients who were aware that they could have chosen a treatment plan that reflected their values and wishes rated all PS items surveyed in this study with high scores.
In a simple tabulation of PS, most respondents chose “5: Strongly satisfied” or “4: Satisfied” in all items. While caution must be exercised when comparing these results directly to those of countries other than Japan, 24 PS surveys in other countries have also reported higher mean scores. 25 In the benchmark project for the “Patient Satisfaction Survey” 2021 provided by JQ, the mean scores for the category that includes the hospitals in this survey were 4.6 points for items corresponding to S1, 4.6 points for S2, 4.7 points for S3, 4.4 points for S4, 4.4 points for S5, and 4.5 points for S6. 23 Although the PS results of this study were slightly lower than the mean scores for the benchmark project, the trends were generally consistent.
In a simple tabulation of the achievement status of patient achievement goals for the sense of participation, approximately 80% of respondents answered “4: Agree” or “3: Somewhat agree” for G1, G2, and G4. G3 was slightly lower, approximately 70%, and unlike the other 3 items, “3: Somewhat agree” was more common than “4: Agree.” It is possible that the percentage for G3 was slightly lower than for G1, G2, and G4 because patients need to learn spontaneously about their disease and its treatment in order to answer “Achieved” for G3. It should be noted that the patient achievement goals are indicators that reflect whether patients have the sense of participation, which may be at a discrepancy with whether they actually achieve participation in healthcare.
The patient achievement goal G1 was significantly positively related to all PS items, including S6, overall satisfaction. This indicates that the realization of appropriate self-determination by patients themselves has a wide-ranging impact on PS. The achievement of G1 has a strong positive impact on S1, again indicating that patients are satisfied with their treatment when they feel that they have made decisions that reflect their values and wishes. Notably, a significant relationship with G1 was found for S4 (coping with pain and symptoms) and S5 (psychological support) as well. It is not necessarily the case that pain and psychological distress will be reduced simply because a treatment plan that reflects values and wishes has been chosen, nor can the degree of pain and psychological distress be compared to the failure to make appropriate choices. Nevertheless, these relationships were observed, perhaps due to the patients’ perception that they were able to reflect their own will brought a sense of acceptance of the treatment. The implementation of activities and the creation of an environment that enables appropriate self-determination by patients themselves would contribute to improving the PS. Previous studies by our group have shown that it is useful for hospitals to promote explanations of treatment options to achieve G1. 26
S4 was observed to be positively correlated with G2. Achieving G2 means that the patients believe that they can communicate interactively with healthcare workers as members of the medical team and that they have the ability to permeate their own will throughout the treatment process. Previous studies have shown that patients with higher self-efficacy are more actively engaged in their own treatment27,28; Patients with self-efficacy, such as G2, may be more satisfied with their care in the face of distress because they are proactive in their own treatment as members of the healthcare team and take responsibility for the outcomes of their treatment.
S5 and G3 were also observed to be positively correlated. The patients’ confidence in their ability to self-learn and apply self-learning to decision making may complement their satisfaction with the psychological support provided by healthcare workers. In addition to the self-efficacy mechanism of having the means to dispel anxiety caused by a lack of knowledge about the disease and its treatment, it is also possible that the patient’s positive attitude toward learning makes the psychological support of healthcare workers more effective. Hospitals should encourage and provide opportunities for patients to self-learning. In our previous studies on the differences between the perception of healthcare workers toward the implementation of activities promoting patient participation and the perception of patients concerning their experiences, the provision of decision support tools is an activity that few patients feel they have “experienced,” contrary to the healthcare workers’ perception that it is being implemented. 29 It has also been noted that there is a lack of practical support for patients using these tools, 2 and hospitals should work on the resolution of these issues.
As an exploratory study, this study has several limitations. No sample size calculations were made, and sampling was done for convenience. Only 5 hospitals, mostly acute-care hospitals, were included in this study and were selected for convenience. Results may be influenced by factors such as the size, location, and proactiveness in patient safety of the hospitals surveyed. Results may also differ in chronic-care hospitals, where patients are hospitalized for longer periods of time and have more opportunities to form perceptions and participate in healthcare. With regard to outpatients and home care patients, maintaining treatment adherence is more important and may require a different perspective. In addition, the selection of patients was left to each hospital. Participating patients were not representative of inpatients at each hospital, and the possibility cannot be ruled out that there may have been a bias toward patients who were in good condition or willing to cooperate, or that patients who were critical or dissatisfied with the hospital were excluded. Actually, the participants in this study had a smaller proportion of elderly women compared to hospitalized patients in Japan as a whole. 30 Although there are numerous hospitalized elderly women in Japan, it is possible that hospital staff were hesitant to include them in the survey because many of them have cognitive impairment. The impact of this difference between the composition of the participants and the actual population on the results needs further study. Furthermore, the 4 patient achievement goals for the sense of participation used in this study have not been validated. They were developed by the authors based on previous studies.
Despite these limitations, this study suggests with quantitative data that patients with a sense of participation may have higher PS across a broad spectrum. Hospitals and healthcare workers should encourage patients to have perceptions similar to some of the patient achievement goals for a sense of participation presented in this study. These efforts are expected to improve the quality of care and attract customers to the hospital. 14 Higher PS scores may improve the patient adherence to treatment, which in turn, may have a positive impact on the treatment outcomes.14,27
One of the advantages of this study is its focus on the patients’ sense of participation, rather than hospital activities or the patients’ experiences with them. In the area of hospitality-related initiatives and services, the activities provided by the hospital are perceived by patients as experiences, and whether these experiences are at the level they expect and anticipate is directly reflected in their PS. 14 In recent years, there has also been a movement toward directly measuring the patient experience (PX), which is a more objective measure than PS.31,32 However, the results of this study suggest that simply examining the presence or absence of activity in a hospital or measuring PX may not be sufficient to explain the relationship between patient participation and PS. The quality indicators for healthcare regarding patient participation should incorporate evaluation methods that consider the impact of the sense of participation. The patient achievement goals used in this study are more specific than PS; however, they encompass internal perceptions of the sense of participation, which may be helpful in developing new evaluation methods for the implementation status of patient participation.
This study suggests that hospitals and healthcare workers should empower patients to engage in a sense of participation. Although there are many hospitals that have a philosophy related to patient participation, it would be good to set a goal of “we want patients to have the sense of participation” rather than just “we provide this kind of service with regard to patient participation.”
Conclusions
This study suggests that patients with a sense of participation have higher PS across a broad spectrum. In particular, the feeling that patients were able to make decisions that reflected their values and wishes was positively related to all PS items asked in the study, including overall satisfaction. The results also suggest that a sense of participation may improve PS not only with the consultation, but also with specific procedures, such as coping to reduce pain and symptoms and psychological support. Patients’ sense of participation is an important factor in increasing PS. Empowering patients to have a sense of participation may improve the quality of care and increase the popularity of hospitals.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241278986 – Supplemental material for Relationship Between Patients’ “Sense of Participation” in Healthcare and Their Satisfaction A Survey of 5 Hospitals
Supplemental material, sj-docx-1-inq-10.1177_00469580241278986 for Relationship Between Patients’ “Sense of Participation” in Healthcare and Their Satisfaction A Survey of 5 Hospitals by Koki Hirata, Yosuke Hatakeyama, Ryo Onishi, Kanako Seto, Kunichika Matsumoto, Shigeru Fujita, Yoji Nagai, Shuhei Iida, and Tomonori Hasegawa, in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We thank all the participants in this study.
Author Contribution Statements
Koki Hirata oversaw this section of the study design and wrote the manuscript; Yoji Nagai, Shuhei Iida, and Tomonori Hasegawa were the overall planners and managers of the broader study design; Koki Hirata, Yosuke Hatakeyama, Ryo Onishi, Kanako Seto, Shigeru Fujita, and Tomonori Hasegawa developed the questionnaire; Yosuke Hatakeyama, Ryo Onishi, and Kanako Seto were the primary data compilers; Statistical analysis was conducted by Koki Hirata, Yosuke Hatakeyama, Ryo Onishi, and Kunichika Matsumoto.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed receipt of the following financial support for the research, authorship, and publication of this article: This work was supported by the Health Labour Sciences Research Grant [grant number JPMH20IA1009].
Ethical/Consent Statement
This study was approved by the Ethics Committee of the All Japan Hospital Association (approval number: R2-001; December 13, 2021).
Consent Statement
All participants were informed and consented to the study in writing.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.