
Abstract
The COVID-19 pandemic has caused a lot of stress for healthcare personnel. They are subjected to arduous and stressful working hours and may contract infection. The objectives of this study were to (i) assess the level of occupational stress and the prevalence of burnout among healthcare workers (HCWs) in the Kingdom of Saudi Arabia during the COVID-19 pandemic and (ii) to identify some sociodemographic characteristics and work-related factors that may influence the level of stress and burnout among such HCWs. An online survey was distributed on social media websites and groups of HCWs in KSA. The survey depended on the stress domain of Depression, Anxiety, and Stress Scale-21 (DASS-21) and the work-related burnout domain of Copenhagen Burnout Inventory (CBI). Data were collected using a Google form and then analyzed. Among 478 respondents, 37.7% of studied HCWs reported mild to extremely severe stress, and 47.9% of them reported work-related burnout. Occupational stress and burnout were more prevalent among front-line HCWs (43.9% and 55%) than among second-line HCWs (31.2% and 40.8%). The mean scores of occupational stress and burnout were significantly much higher among frontline physicians and nurses particularly those who are females, of younger age (≤40 years), with few years of work experience (≤15 years), being married, having chronic disease, and those previously infected by COVID-19. HCWs reported a high prevalence of occupational stress and burnout during the COVID-19 pandemic. Establishing policies and guidelines, enhancing working conditions, and providing continuous psychological support and assurance to HCWs are recommended to improve their resilience and increase their coping capacities toward pandemics.
Rare previous studies conducted in the Kingdom of Saudi Arabia (KSA) to evaluate the occupational stress and of burnout in HCWs working during the COVID-19 pandemic.
This study sheds light on the increased prevalence of occupational stress and burnout among healthcare workers in the Kingdom of Saudi Arabia during COVID-19. In addition, it determines some sociodemographic and work-related factors that influence occupational stress and burnout during such pandemics.
These research findings will help decision-makers establish policies and guidelines, enhance working conditions, and implement interventions targeting the reduction of stress and burnout among healthcare workers during future pandemics.
Introduction
The coronavirus pandemic (COVID-19, formerly known as nCoV-2019) started in late December 2019 and was first reported in Wuhan, China. Since then the virus has spread to more than 60 countries all around the world. 1 In Saudi Arabia, from Mar 2 to 17 June 2020, there have been 141 234 confirmed cases of COVID-19 with 1091 deaths and since the end of March 2020, the Kingdom of Saudi Arabia (KSA) adopted a massive lockdown to decrease the spread of the virus. 2 Early Italian study has documented the adverse psychological impact of this lockdown decision on healthcare workers (HCWs) and the general population. About one-third of participants showed moderate to severe depression, anxiety and stress. 3
Burnout was first defined in the mid-1970s, by Freudenberger and Maslach as a state of physical, emotional, and mental exhaustion that results from long-term involvement in work situations that are emotionally demanding. It is a multidimensional syndrome comprising emotional exhaustion, depersonalization, and reduced personal accomplishment. 4 Burnout has been recognized globally as a major health problem, affecting both the physical and mental well-being of HCWs. During the current COVID-19 pandemic, the closing down of international and state borders, and strict city and area lockdowns have adverse effects on HCWs and their families as well, causing excessive stress and psychological effects. 5
The medical professions are particularly burdened with a high risk of negative effects from their professional life. The phenomenon of occupational burnout deserves special attention. It is characterized by many symptoms that are difficult to diagnose and are often mistaken for temporary fatigue. 6 Healthcare workers play a critical role in taking care of the infected patient, which could be challenging due to the consistent contact with the infected patients. Widespread infection and mortality among healthcare workers have been known previously for MERS, SARS, and current COVID-19 disease, leading to social and mental pressure on the healthcare workers and their families such as fear, anxiety, and even stigma as reported previously by healthcare workers during MERS and SARS outbreaks. 7
Previous research showed that HCWs and those who survived infectious disease outbreaks tend to experience job pressure, burnout, and symptoms of stress, depression, and anxiety, along with post-traumatic stress disorder.5,8,9 Burnout, apart from being personally harmful, can lead to suboptimal patient care. 10
A Chinese study conducted by Lai et al 11 revealed that frontline HCWs caring for COVID-19 patients were at increased risk of having symptoms of stress, anxiety, and depression. Xiao et al 12 studied the effect of social support on improving the mental health of physicians and nurses, caring for COVID-19 patients, at Wuhan University School of Medicine Hospital. They noticed that HCW respondents had high levels of anxiety, stress, and self-efficacy, which depended on the quality of sleep and social support. Another study was conducted by Alqahtani et al 13 to explore the magnitude and determinants of burnout among emergency physicians and nurses working at emergency departments of hospitals in Abha and Khamis Mushait cities (Saudi Arabia). The overall prevalence of burnout among healthcare professionals was 16.3% with the male healthcare professionals at higher three- risk for developing burnout compared to females.
The World Health Organization (WHO) has recognized the risk of psychological impact among HCWs during COVID-19 and has released a document about its psychosocial consideration. However, few steps are being taken by healthcare organizations’ administrators to reduce the effect of occupational stress on HCWs. 14 Results of a recent study highlighted the need for psychological aid interventions with anxiety and fear of contagion representing the main concern for both healthcare workers and the general population. 15
Burnout and occupational stress affect one’s well-being and are associated with medical errors in the case of HCWs. Since the outbreak, HCWs have been under an extensive workload, which is important to protect the workforce and insure providing good quality services to the patients. 16 Moreover, rare previous studies in the Kingdom of Saudi Arabia (KSA) have been conducted to evaluate the occupational stress and prevalence of burnout in HCWs working during the COVID-19 pandemic. Maslach et al 4 first described Maslach Burnout Inventory (MBI) in 1981. The MBI defines burnout based on 3 facets, presence of emotional exhaustion, depersonalization, and lack of personal fulfillment. Kristensen et al questioned the reliability of MBI, with many arguments and to overcome the drawbacks of MBI, introduced the Copenhagen Burnout Inventory (CBI).5,17 Therefore, this study was carried out using Depression, Anxiety, and Stress Scale-21 (DASS-21) 18 and Copenhagen Burnout Inventory (CBI) 17 to assess the level of occupational stress and the prevalence of burnout among HCWs in KSA during such pandemic, and then to identify some sociodemographic characteristics and work-related factors that may influence the level of stress and burnout among these HCWs. Our research findings would help decision-makers in KSA establish policies and guidelines, enhance working conditions, and implement interventions targeting the reduction of stress and burnout among healthcare workers during future pandemics.
Methods
Study Design and Population
This descriptive cross-sectional study was conducted in the Kingdom of Saudi Arabia during the period between 24 January and 28 April 2022. The study targeted HCWs working in different regions in the Kingdom of Saudi Arabia during the COVID-19 pandemic (Primary healthcare workers and those involved in the management of suspected/confirmed COVID-19 cases). The inclusion criteria were being a healthcare worker in KSA and employed during the lockdown consequent to the COVID-19 outbreak with a full-time governmental contract. No exclusion criteria were applied. The sample size was calculated to be 384 using OpenEPI program at a 95% confidence interval, power of 80%, and margin of error of ±5%. A sample of 485 HCWs, including doctors, nurses, and technicians participated in this study through an online survey. Due to missing data, 7 participants were eliminated, leaving 478 HCWs included in the final analysis.
Instruments and Measurements
The data was collected using an online survey depending on a pre-validated, self-administered structured questionnaire that assesses occupational stress and burnout. The survey was distributed online, using Google form, through various social media websites and groups of different HCWs’ on Facebook, and WhatsApp in Saudi Arabia. Participants were invited to participate in the study by agreeing on an online informed consent form and filling out the survey questionnaire (Supplemental Material). The first page was designed to obtain informed consent from the participants: if he/she agreed, the questionnaire would move forward to the next page, otherwise, it would end. To avoid data duplication and ensure the accuracy of the data, each device was allowed to fill in the questionnaire once only using an email address, we activated the Limit to 1 response option and do not allow response editing after submitting. The questionnaire takes an average of 15 min to fill.
The questionnaire comprised 3 partitions: socio-demographic and work-related data, the stress domain of the Depression, Anxiety, Stress Scale (DASS-21) questionnaire, 18 and the work-related burnout domain in the Copenhagen Burnout Inventory (CBI). 17 These questionnaires were previously validated and have been used in many previous studies. Regarding overall reliability of the current study, Cronbach’s alpha was .85 for the DASS-21 (stress domain) and .84 for the CBI (work-related burnout domain), indicating excellent internal consistency. The English version of these questionnaires was used.
Sociodemographic and occupational characteristics partition included age, gender, marital status, income level, nationality, comorbidities, job title, years of experience, job position in relation to COVID-19 (front-line or second-line), and if they have been infected by CIVID-19.
The occupational stress partition used the stress domain in DASS-21, developed by Lovibond and Lovibond 18 in 1995, to measure the stress level. The DASS-21 stress domain encompasses 7 questions that evaluate difficulty relaxing, persistent arousal, and being easily upset, agitated, irritable, over-reactive, or impatient. For each item, the score is an integer number between 0 (it does not apply to me at all) and 3 (it applies to me exactly). The final score was calculated by summing up the scores of the 7 questions and then multiplied by 2. The severity of stress was rated as follows; normal (0-14), mild (15-18), moderate (16-25), severe (26-33), and extremely severe (34+). Studies revealed adequate levels of reliability for all 3 subscales of the DASS-21 questionnaire with the highest reliability in the stress subscale (Stress, α = .87).19,20
Burnout partition included the second domain (Work-related burnout) in CBI, which consists of 7 items. Each item has 5 response categories in the Likert scale and was assigned a score between 0 (never/almost never) and 100 (Always). If less than 3 questions had been answered, the respondent was classified as a non-responder. The average total score was then calculated with a cutoff point of 50. A total score >50 was interpreted as engagement with job burnout. 17 CBI was designed to be applied in different domains and was found to have very high internal reliability. 21 Studies concluded that the work-related burnout scale from the CBI offers adequate validity and reliability to study job burnout among HCWs.17,22
Statistical Analysis
The collected data were retrieved from the Google form and analyzed by SPSS software (version 21). 23 Nominal Variables were summarized using proportions and expressed as frequencies and percentages while quantitative variables (DASS-21 stress and CBI scores) were summarized as (mean ± SD). Statistical differences between proportions were tested using the Chi-square test, 24 while comparisons between means were done using student t-tests. 25 For ordinal scale and non-parametric data, the Mann-Whitney U test 26 and the Kruskal-Wallis test 27 were used to test the difference. Spearman-rho correlation was utilized for conducting correlational analysis between age, years of experience, stress, and burnout scores. 28 Univariate analysis was done to look for an association between demographic characteristics and work profile with occupational stress and burnout. Results were considered to be statistically significant if (P ≤ .05).
Ethics Approval
The study protocol and instrument were revised and approved by the Institutional Research Board of King Saud Medical City in Riyadh (H1RI-22-Nov21-03). We confirm that all procedures of the research comply with the Declaration of Helsinki. An online informed consent to participate in the study was included at the beginning of the online survey. The participants were informed about the aim of the study, that their participation was voluntary, and that collected data would be used only for the purpose of the study. Participation in this study was optional and anonymous. Confidentiality of the data was ensured.
Results
Our study analyzed the responses from 478 HCWs (178 physicians, 135 nurses, and 165 technicians) working in health care services in Saudi Arabia during the COVID-19 pandemic and measured their stress and burnout status during the pandemic. The majority of participants were females (63.6%) and most of them were Saudis (91.2%) aged ≤40 years (57.3%) with a mean age of (40.35 ± 7.9). Furthermore, the majority of participants were married (79.3%), almost 79.9% had a monthly income of more than 10 000 Saudi Riyals, and no history of chronic diseases among 78.1% of them. With regard to working positions during the COVID-19 pandemic, about half (50.2%) of participants were front-line HCWs who worked in high-risk settings, while 49.8% were second-line HCWs. Finally, over half (52.9%) of HCWs reported working experience of fewer than 15 years, and almost 63.6% of them were infected with COVID-19.
Figure 1 illustrates the percentage of HCWs in each of the 5 categories according to (DASS-21 Stress) scale. One hundred eighty participants (37.7%) of HCWs reported mild to extremely severe stress. The prevalence of stress was significantly much higher among front-line HCWs dealing with COVID-19 than among other second-line HCWs (P < .001). Mild, Moderate, severe, and extremely severe stress was reported by (13.8%, 13.8%, 10.0%, and 6.3%) of front-line HCWs versus (8.8%, 12.6%, 6.3%, and 3.8%) of second-line HCWs respectively.

Level of stress among the study participants by job position during the COVID-19 pandemic according to DASS-21 stress subscale (N = 478).
Table 1 displays the distribution of work-related burnout among participants in terms of the CBI scale using a 50-point cut-off in the mean burnout scores. The overall prevalence of work-related burnout among HCWs during the COVID-19 pandemic was 47.9%. The prevalence of burnout was significantly much higher among front-line HCWs dealing with COVID-19 than among other second-line HCWs (55% and 40.8% of participants, respectively) with a P < .01.
Burnout Distribution among the Study Participants According to Job Position During the COVID-19 Pandemic (N = 478).

P ≤ .05 is significant.
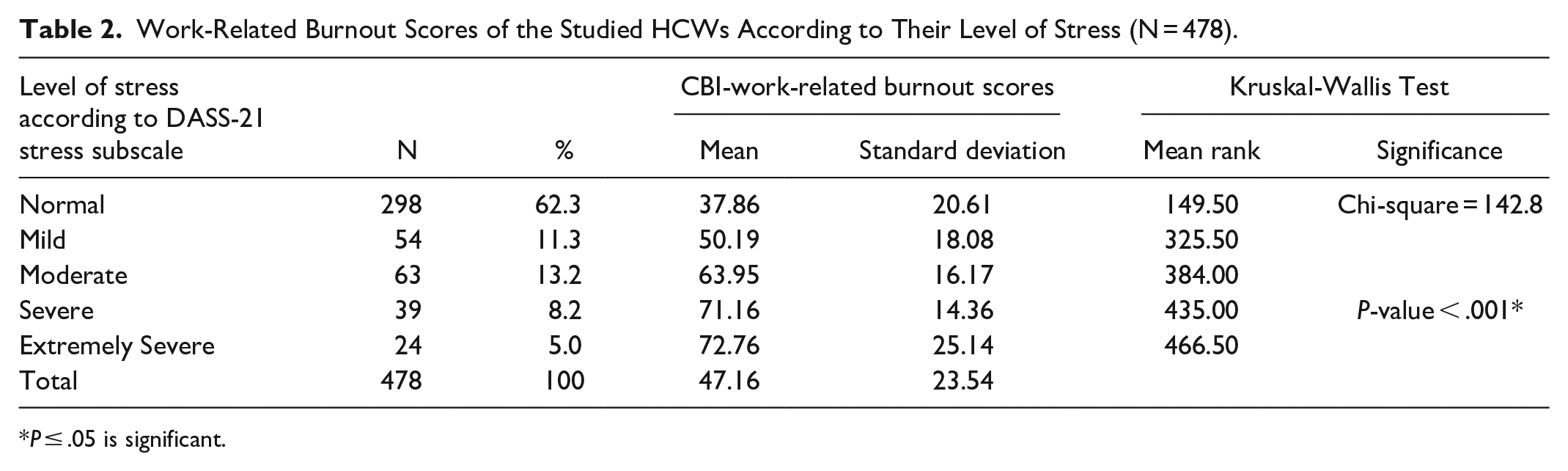
Using the CBI scale, the overall mean (±SD) score of work-related burnout among HCWs during the COVID-19 pandemic was 47.16 (±23.54). The mean burnout scores were significantly higher among HCWs with an increased level of stress (50.19 ± 18.08) in mild stress, (63.95 ± 16.17) in moderate stress, (71.16 ± 14.36) in severe stress, and (72.76 ± 25.14) in extremely severe stress, respectively. The differences between these burnout scores were statistically significant (P < .001) (Table 2).
Work-Related Burnout Scores of the Studied HCWs According to Their Level of Stress (N = 478).
P ≤ .05 is significant.
Table 3 shows the descriptive statistics and correlational analyses that determine the linear agreement between the CBI-work-related burnout scores and the observed DASS-21 stress scores, age, and years of work experience. Work-related burnout during the COVID-19 pandemic had a strong positive correlation with the observed DASS-21 stress scores (r = .57; P < .01). However, work-related burnout was negatively associated with age (r = −.36; P < .01) and years of work experience (r = −.41; P < .01), respectively. In addition, DASS-21 stress scores showed a negative correlation with age (r = −.22; P < .01) and years of work experience (r = −.29; P < .01), respectively.
Correlational Analyses Between CBI-Work-Related Burnout Scores, DASS-21 Stress Scores, Age, and Years of Work Experience (N = 478).

P ≤ .05 is significant.
We performed univariate analysis to determine the sociodemographic and work-related factors associated with the occurrence of stress and burnout among HCWs during the COVID-19 pandemic. The mean DASS-21 stress scores and CBI-work-related burnout scores were statistically significantly higher in HCWs in the younger age group ≤ 40 years (P < .001), female gender (P = .043 and <.001 respectively), married HCWs (P < .001), and those with chronic diseases (P < .001). Physicians and nurses exhibited significantly higher stress and burnout scores compared to technicians (P < .001). HCWs with medical experience of ≤15 years, reported significantly higher stress and burnout scores (P < .001). Other significant factors included front-line HCWs directly dealing with COVID-19 patients (P < .001) when compared to those working at second lines. In addition, HCWs who were infected by COVID-19 showed a significantly higher level of stress than those who were not infected (P = .022), with no significant difference in burnout scores. On the other hand, either no significant difference was detected in stress or burnout scores as regards nationality and income (Table 4).
Univariate Analysis of Sociodemographic and Work-Related Characteristics of the Study Participants on Developing Stress and Work-Related Burnout (N = 478).

P ≤ .05 is significant.
Discussion
During the Covid-19 pandemic, healthcare workers play a critical role that puts them at higher risk of experiencing anxiety and stress due to the overwhelming demands on the healthcare systems. 20 This study presents essential findings about the mental well-being of HCWs, which can assist in the development of effective coping mechanisms and strategies for addressing the challenges they face during the pandemic. Past studies suggest that the causes of burnout include administrative tasks, time constraints, autonomy in decision-making, and interactions with colleagues and patients. However, this study reveals significant levels of burnout among HCWs during the pandemic, consistent with previous research demonstrating a concerning prevalence of burnout, necessitating urgent action. 21 This study examined the level of occupational stress and prevalence of burnout among HCWs facing the COVID-19 outbreak and found out 38% of HCWs had experienced mild to extremely severe stress. Our findings are similar to Hathout et al 20 study, which their finding showed that 28% of HCWs have experienced stress during the COVID-19 pandemic. However, this finding is shown to be lower than that of Lai et al 29 who reported stress among 71.5% of HCWs working in Covid-19 hospitals in China. In addition, this study showed that burnout scores were significantly higher among HCWs with an increased level of stress. In our study, the prevalence of work-related burnout among HCWs during the COVID-19 pandemic was 47.9%. That is nearly similar to a recent Lebanese study that found around 47% prevalence of work-related burnout among HCWs. 30 On the other hand, our results were lower than the findings of a study conducted among HCWs in Saudi Arabia where 75% of Saudi HCWs were reported to suffer from burnout during the COVID-19 pandemic. 22 Moreover, the prevalence of burnout as determined in this article is similar to the study conducted among 60 countries, including Turkey, the United States, and Italy, where the prevalence of burnout was reported to be 51%. 31
The current work revealed statistically significant higher stress and burnout scores among HCWs younger than 40 years which may be attributed to the less practical experiences among younger HCWs compared to the older ones. This finding is supported by many studies which found that younger HCWs are at higher risk of developing mental stress. 21 One of the theories behind this is that younger age groups are more exposed to social media, which shares huge amounts of information regarding the crisis, and are more affected by the restrictions on outdoor activities during the lockdown, as they are more involved in such activities than older people are. 32 Another theory supported by an article on the knowledge of and attitudes toward COVID-19 is that older people can manage their stress as they are more knowledgeable regarding this pandemic than younger people. 33
Our research indicates that female healthcare workers have an elevated likelihood of experiencing burnout and experiencing high levels of stress. These findings align with other studies; for example, female physicians have been shown to exhibit more burnout symptoms than their male peers according to the Medscape National Physician Report. 34 Similarly, a survey conducted in Italy found that women under 30 working in healthcare reported greater levels of burnout. 35 Additionally, a systematic review revealed that female healthcare workers in the US tended to experience higher stress scores, possibly due to factors like their concentration in patient-facing roles, gender expectations in caregiving, and substantial workload outside of work. 36 The present study revealed that married HCWs exhibited a higher prevalence of both burnout and stress, which could be due to fear of transmitting the infection to their families at home as well as the additional family demands and responsibilities, particularly for women who are often expected to fulfill certain familial roles. 37
Healthcare workers with fewer years of experience in the medical field also had a higher likelihood of experiencing burnout, as observed in previous studies. 20 Our study revealed that the job category has a significant influence on experiencing both stress and burnout as physicians and nurses had significantly higher stress and burnout scores compared to technicians. These findings are partially consistent with Hathout et al 20 in Egypt, who revealed that physicians showed significantly higher stress and burnout scores compared to other participants of nurses or technicians. This may be attributed to the nature of the job, the increased risk of getting an infection and the lack of social support as physicians and nurses were mainly assigned to the frontline during the COVID-19 pandemic, however, the majority of technicians were working in the second-line.
The prevalence of stress in this study was significantly much higher among frontline HCWs dealing with COVID-19 than among other second-line HCWs. Those working on the front line are directly involved in the diagnosis and treatment of COVID-19 cases, with higher levels of personal and occupational burnout. This is supported by a study in China comparing healthcare workers in the front-line and second-line which also indicated a higher incidence and more severe symptoms of depression, anxiety, insomnia, and mental distress among frontline healthcare workers. 11
Limitations
This study has limitations, as data were collected through an online questionnaire distributed via social media using convenience sampling, potentially limiting the study’s reach and response rates as well as responses and selection bias could not be avoided. However, using an online questionnaire was necessary due to the lockdowns and the need for social distancing during the COVID-19 crisis. Another limitation is that this study used a cross-sectional design limits causal inferences, so we were unable to establish a causal association between the studied variables. We also did not ask about prolonged working hours and past psychiatric problems, which seem to have an influencing effect on stress and burnout scores. Nonetheless, nearly all HCWs during the COVID-19 pandemic worked extra hours and had extra workload.
Implications for Future Research
While burnout and stress are analyzed in our research, their correlation with workload, job satisfaction and moreover, with resilience, could be interesting to be investigated further. Later, in future research, it will be necessary to evaluate the long-term implications of the present pandemic. In addition, Follow-up studies and randomized controlled trials rather than cross-sectional studies should be conducted to determine the predictors and influencing factors of occupational stress and burnout during such pandemics and to evaluate the effectiveness of implemented interventions that target the affected HCWs. Moreover, as physicians and nurses exhibited significantly higher stress and burnout scores compared to technicians, they should be given special attention during future planning and interventions, and this point warrants more exploration in future research.
Conclusion
Healthcare workers reported varying degrees of occupational stress and a high prevalence of burnout during the COVID-19 pandemic. Occupational stress and burnout were more prevalent among frontline physicians and nurses particularly those who are females, of younger age with few years of work experience, being married, having chronic disease, and those previously infected by COVID-19. Special attention should be given to these influencing factors to reduce the prevalence of occupational stress and burnout among HCWs. Establishing policies and guidelines, enhancing working conditions, enforcing infection prevention training, the provision of continuous psychological support and assurance to HCWs, and regular assessment of their mental health are recommended to improve their resilience and increase their coping capacities toward pandemics.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241275328 – Supplemental material for Occupational Stress and Burnout Among Healthcare Workers in Saudi Arabia During the COVID-19 Pandemic
Supplemental material, sj-docx-1-inq-10.1177_00469580241275328 for Occupational Stress and Burnout Among Healthcare Workers in Saudi Arabia During the COVID-19 Pandemic by Amro Abdel-Azeem, Abdulmajeed Alshowair, Esam Alshora, Malak Alotaibi, Faisal Alruhaimi, Ali Tolba, Saad Alshahrani and Samar Amer in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors acknowledge all of the participants in the online survey that made this study possible.
Author Contributions
All authors made a significant contribution to this study whether in the conception, study design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The study protocol and instrument were revised and approved by the Institutional Research Board of King Saud Medical City in Riyadh (H1RI-22-Nov21-03). We confirm that all procedures of the research comply with the Declaration of Helsinki. An online informed consent to participate in the study was included at the beginning of the online survey. The participants were informed about the aim of the study, that their participation was voluntary, and that collected data would be used only for the purpose of the study. Participation in this study was optional and anonymous. Confidentiality of the data was ensured.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.