
Abstract
This study aimed to assess the current status of gestational diabetes mellitus (GDM) diagnosis and management, and the demand for a digital healthcare system, in order to develop an optimal digital-based management model for GDM. An anonymous online survey was conducted targeting pregnant/postpartum women (Group W), internal medicine physicians (Group P), and obstetricians (group O) from September 6, 2022 to December 31, 2022. The survey assessed the women’s knowledge of GDM and gathered information about healthcare professionals’ (HCPs) current GDM management practices. All groups were asked about their acceptance of and demands for a digital healthcare system for GDM. Statistical comparisons between groups were conducted using the chi-square test or Fisher’s exact test where appropriate. A total of 168 participants were in Group W, 185 in Group P, and 256 in Group O. Participants from all groups recognized the need for a digital healthcare system for GDM (Group W: 95.8%, Group P: 85.9%, Group O: 60%). However, HCPs showed less willingness to integrate these systems into their clinics than pregnant/postpartum women. Essential features identified were recording blood glucose levels and insulin, along with automatic data linkage from self-monitoring devices. Group W showed a higher preference for lab test access, search functionality, and fetal weight assessment than groups P and O (all P < .0001), while Groups P and O had a greater preference for recording insulin and maternal body weight compared to Group W (P = .0141 and .0023, respectively). Both pregnant/postpartum women and HCPs acknowledged the benefits of utilizing a digital healthcare system for managing GDM. However, there were differences in perspectives among these groups.
There are many digital-based management models for GDM, but there is still a lack of standardization.
This study aims to understand the current status of digital-based management for GDM and to assist in the development of an optimal model.
An optimal digital-based management model for GDM would standardize GDM management.
Introduction
Gestational diabetes mellitus (GDM) is a major pregnancy complication associated with other obstetric complications, such as preeclampsia, cesarean delivery, and shoulder dystocia. It is also a major risk factor for long-term complications such as future type 2 diabetes, obesity, and cardiovascular disease in mothers and offspring.1 -4 Its incidence in South Korea has been steadily increasing every year between 2012 and 2016, with an annual increase rate of 11.1%. 5 This trend is attributed to older maternal ages and increased use of assisted reproductive technologies. 6 With these trends, the number of GDM pregnancies is expected to continue to rise in South Korea, similarly to international trends.5,6
Optimal management of GDM requires women’s involvement in the self-monitoring of blood glucose, adequate education, and review of health data records by doctors.1,7 Some countries, including Germany, have management systems for GDM patients, such as GDM registries or postpartum follow-up programs for women with a history of GDM, through either government-led initiatives or research-based programs.8,9 However, there is still a lack of international consensus on the diagnosis of GDM, and a standardized, comprehensive, and systematic management model for GDM patients has not yet been established in Korea or other countries. 1 In Korea, the Korean Diabetes Association (KDA) has established diagnostic criteria and treatment guidelines for GDM.10,11 However, 2 diagnostic criteria are being used interchangeably. 1 In addition, there are limitations to the treatment of GDM, such as an imbalance in the quality of medical care between regions, a lack of GDM experts, and a lack of a capable and efficient education system, making it difficult to deliver proper diagnosis and management in clinical settings.
In recent studies, various institutions implemented digital healthcare interventions in GDM and postpartum management to support women’s self-care and obtained favorable clinical outcomes.12 -14 These studies remotely monitored blood glucose levels, provided feedback on blood glucose levels, and provided several educational messages. Although there were differences in the intervals and methods, digital health care showed moderate certainty evidence supporting the results in improving blood glucose control and reducing cesarean sections. The American Diabetes Association (ADA) mentioned that technology combined with online coaching can be beneficial. 15 Even though many researchers have tried to develop a GDM management model for Korea using digital health technologies, its use still has many limitations. For proper care system planning, it is essential to investigate perspectives and demands regarding digital healthcare among women and healthcare professionals (HCPs) who are potential users.
This study aimed to understand the current status of diagnosis and management of GDM and investigate the need required by pregnant women and HCPs for a digital healthcare system to develop an optimal digital-based management model for GDM during pregnancy and after delivery.
Methods
Study Design
This research conducted a cross-sectional survey to assess the current status of GDM diagnosis and management and to evaluate the demand for a digital healthcare system, aiming to develop an optimal digital-based management model for GDM. The participants were categorized into 3 groups: pregnant/postpartum women (Group W), internal medicine physicians (Group P), and obstetricians (Group O). Data collection was conducted from September 6, 2022, to December 31, 2022, with each group receiving a different version of the questionnaire.
Study Setting
The study was conducted at the Obstetrics and Gynecology outpatient clinic, where pregnant/postpartum women were recruited. The survey for these participants was facilitated through a written guide explaining the purpose and procedure of the survey. An anonymous online survey was conducted using a QR code. For HCPs, including physicians and obstetricians, anonymous questionnaires were distributed via email to those registered with the KDA or the Korean Society of Obstetrics and Gynecology. All participants responded to the survey voluntarily. Participants who completed the questionnaires were provided with a mobile drink coupon.
Study Subjects
All pregnant/postpartum women, either currently expecting or within 1 year post-delivery, who visited the Obstetrics and Gynecology outpatient clinic during the study period, were eligible to participate. HCPs qualified for the study if they had experience managing pregnancies or GDM. However, individuals lacking experience in managing GDM or pregnancies in the past 5 years were excluded. Participants who reviewed the provided leaflet (for pregnant/postpartum women) or the email (for HCPs) containing research details, and voluntarily agreed to participate, and completed the survey, were included in this study.
Survey Questionnaires
The questionnaire was developed by researchers based on previous studies.16 -18 Preliminary pilot testing with 20 participants from each group was conducted to identify and address any necessary modifications or enhancements for better understanding of respondents. Following these adjustments, the questionnaire was specifically designed for online administration, enabling automatic calculation of scores. An independent statistician organized and analyzed the collected data.
Three versions of the questionnaire, tailored to the participant groups, are available in Supplemental Material 2. For pregnant/postpartum women, the questionnaire comprised 3 parts: demographic information, including lifestyle and eating habits; knowledge of GDM; and perspectives on the digital healthcare system regarding GDM. For HCPs, the questionnaire covered demographics, characteristics of their place of employment (including whether they worked in clinics or hospitals, and if these were private or public institutions), clinical experience, and practices for antenatal and postpartum management of pregnant women with GDM or DM. It also requested their views on the digital healthcare system regarding GDM.
Women’s demographic information included age, height, weight, pre-pregnancy body mass index (BMI), gestational age, parity, family history of DM, monthly family income, and education level. Lifestyle and eating habits, covering topics such as the number of meals consumed per day, the frequency of breakfast consumption per week, the frequency of ordering delivery food, and the amount of physical activity were included.
HCPs’ information included their medical specialty, the characteristics of their employing hospital, years of clinical practice, and how often they see patients with diabetes or gestational diabetes. Physicians received questions aligned with their experience in managing GDM or DM, while obstetricians were given questions focusing on the diagnosis of GDM during pregnancy.
A knowledge assessment for pregnant/postpartum women regarding GDM consisted of 14 questions (Supplemental Table S1). Participants were required to respond with “yes” or “no.” Examples of questions are as follows:
GDM occurs during pregnancy due to the influence of placental hormones, which is different from diabetes.
GDM appears only in the later stages of pregnancy (after 24 weeks).
Any insulin can cross the placenta and affect the fetus; therefore, it should not be used during pregnancy.
Follow-up is not necessary, when the oral glucose tolerance test is normal after delivery.
In the first section of the survey on perspectives regarding a digital healthcare system for GDM, all participants provided their opinions on the essential information to be incorporated into the digital healthcare system for GDM. The second section gathered participants’ opinions on the necessity of features listed, which were identified from prior research on digital healthcare applications for diabetes management. 16 In the third section, participants selected additional features they would like to include in the system. Responses were provided with a 4-point scale, ranging from “definitely necessary,” “moderately necessary,” “slightly necessary,” to. For analysis purposes, we simplified them into 2 (combining “definitely necessary” and “moderately necessary”) and “unnecessary” (combining “slightly necessary” and “unnecessary”).
All participants were asked about their perspectives on a digital healthcare system in GDM. HCPs answered about their intention to use the program in their clinics, including reasons for their responses.
Sample Size Calculation
The sample size was determined using PASS 16, a sample calculation program, for the survey with a 95% confidence interval and alpha of 0.05. The Korean birth number in 2021 was 260 500, with an expected delivery count of 125 000 for 6 months. Approximately 90% of pregnant/postpartum women were estimated to agree to participate in the digital-based GDM management program. The calculated sample size was 139. Considering a non-response or incomplete response rate of 50%, the final estimated sample size for pregnant/postpartum women was 278. In Korea, according to statistics released by the National Statistical Office, there were 17 606 internal medicine physicians in January 2022, including 7681 primary care physicians. Assuming that 50% of primary clinic physicians and 5% of secondary or tertiary clinic physicians would treat GDM patients, this corresponds to an estimated number of approximately 4000 physicians expected to manage GDM cases. Approximately 85% of physicians were assumed to agree to participate in the GDM management program, resulting in an estimated required sample size of 187. Considering a non-response or incomplete response rate of 10%, the final estimated sample size for pregnant/postpartum women was 208. There were approximately 2600 obstetricians involved in treating pregnant women. 19 Assuming that 85% of obstetricians would agree to develop the digital-based GDM management program, the calculated sample size was 183. Considering a non-response or incomplete response rate of 10%, the final estimated sample size was 204.
Statistical Analysis
Participants’ baseline characteristics and clinical experience are presented as numbers (%) for categorical variables and as the mean and standard deviation (SD) for continuous variables. Group comparisons were performed using the chi-square or Fisher’s exact test where appropriate. All statistical analyses were performed using SAS software, version 9.4 (SAS Institute Inc., Cary, NC, USA). Statistical significance was set at P < .05.
Ethical Considerations
Ethical approval for protocol and questionnaires was approved by the Institutional Review Board (IRB) of Seoul St, Mary’s Hospital, the Catholic University of Korea (approval number: XC23OIDI0012). Written informed consent was waived by the Institutional Review Board/Ethics Committee, and participation in this survey implied participant consent. The study was conducted in accordance with the Declaration of Helsinki.
Results
Baseline Characteristics
Pregnant/postpartum women
A total of 168 women (Group W) completed the questionnaires, with an average age of 34.3 years. Their mean BMI before pregnancy was 22.0 ± 3.5 kg/m2. Among them, 79.2% were pregnant with a mean gestational age of 24.5 weeks and 29.8% were diagnosed with 1 type of diabetes during pregnancy. In addition, 57.1% had experience using a mobile application related to health management and 58% responded that eating habits were unhealthy, including skipping breakfast, eating out frequently, and overeating. The rate of regular exercise was only 28% (Table 1).
Baseline Characteristics of Pregnant/Postpartum Women.

Note. Values are expressed as mean ± standard deviation, or number (%).
BMI = body mass index; GDM = gestational diabetes mellitus; T1DM = type 1 diabetes mellitus; T2DM = type 2 diabetes mellitus.
Health care professionals (HCPs)
A total of 185 internal medicine physicians (Group P) and 256 obstetricians (Group O) completed the questionnaires. The mean age was 44 ± 8 years in Group P and 45 ± 9 years in Group O. It was found that 82.7% of Group P and 62.9% of Group O participants worked at the hospital level, whereas the rest worked at the clinic level. In addition, 57.3% of Group P participants and 57.8% of Group O participants worked in metropolitan areas. Among patients seen by Group P, 62.3% had diabetes, and among them, 21.1% were women of reproductive age. About 90% of Group O participants answered that less than 15% of treated pregnant women had gestational diabetes or diabetes in the last 3 years (Table 2).
Baseline Characteristics of HCPs.

Note. Values are expressed as mean ± standard deviation, or number (%).
HCP = healthcare professional; N/A = not available.
Current status in diagnosis and management of GDM by HCPs
Among obstetricians, 68.4% responded that they had screened high-risk women for GDM before 20 weeks of gestational age (GA) (early pregnancy), as shown in Table 3. The top 3 risk factors for early diagnosis were a history of GDM during the previous pregnancy (21.9%), BMI over 25 before pregnancy (13.0%), and detection of glucose in urine (11.4%). For the diagnosis of GDM in early pregnancy, 2-step approach through a 100g oral glucose tolerance test (OGTT) was mainly used (65.9%), followed by fasting blood glucose (12.9%) or 1-step approach through a 75 g OGTT (11.3%) were used alternatively. Regarding the diagnostic test for GDM during the second trimester (GA 24-28 weeks), most obstetricians (87.5%) used 2-step approach. Although the screening tests for GDM in the second trimester was negative, 31.3% performed GDM diagnostic test in the third trimester for those with suspected LGA in ultrasound scans twice or more and those with abnormal blood sugar levels discovered incidentally. For diagnostic criteria of the 100 g OGTT, 22.3% of obstetricians selected the National Diabetes Data Group (NDDG) standards, and 77.7% chose the Carpenter-Coustan criteria, respectively.
Diagnosis and Management of GDM in HCPs.

Note. Values are expressed as number (%).
DM = diabetes mellitus; Etc. = and other things; GDM = gestational diabetes mellitus; IM = internal medicine; NDDG = the National Diabetes Data Group; OGTT = oral glucose tolerance test; SMBG = self-monitoring blood glucose; Tx = treatment.
To manage mothers diagnosed with GDM, approximately 30% of both physicians and obstetricians directly provided diet, exercise, and self-monitoring of blood glucose (SMBG) education. For postpartum management, 92.4% of physicians and 84.4% of obstetricians advised on the necessity of undergoing a glucose tolerance test within 4 to 12 weeks after childbirth. Also, 96.8% of physicians and 75.4% of obstetricians recommended that patients with GDM undergo annual diabetes check-ups, even if their post-delivery glucose tolerance tests returned normal results.
Pregnant/postpartum women’s knowledge of GDM
The average score for knowledge-assessment questions on GDM by participating women was 83.2 ± 12.2 points out of 100 points. The rates of correct answers related to the use of glycemic control drugs including insulin during pregnancy, knowledge of the long-term risk of GDM, and knowledge of postpartum care after GDM were lower than 80%. Full 14-questions with results are shown in Supplemental Table S1.
Perspectives and usages of digital healthcare systems in GDM
About 95.8% of women said that they would use an application that could manage GDM or pre-pregnancy diabetes, and 66.3% of physicians answered that they would use the digital system during patients’ pregnancy. Among obstetricians, 58.6% showed a positive inclination to use a digital system during patients’ pregnancy. In addition, 85.9% of the physicians agreed or strongly agreed the use of digital applications to manage diabetes during pregnancy (Figure 1).

Agreement of using a digital healthcare system in GDM management.
Features required by participants in a digital healthcare system
Essential Information
Dietary guidelines for GDM, food recommendations for GDM, dietary guidelines when treated with insulin, nutrition information about food, and information about the relationship between food and blood glucose levels were answered as the top 5 essential information in the system, by all 3 groups (Figure 2).
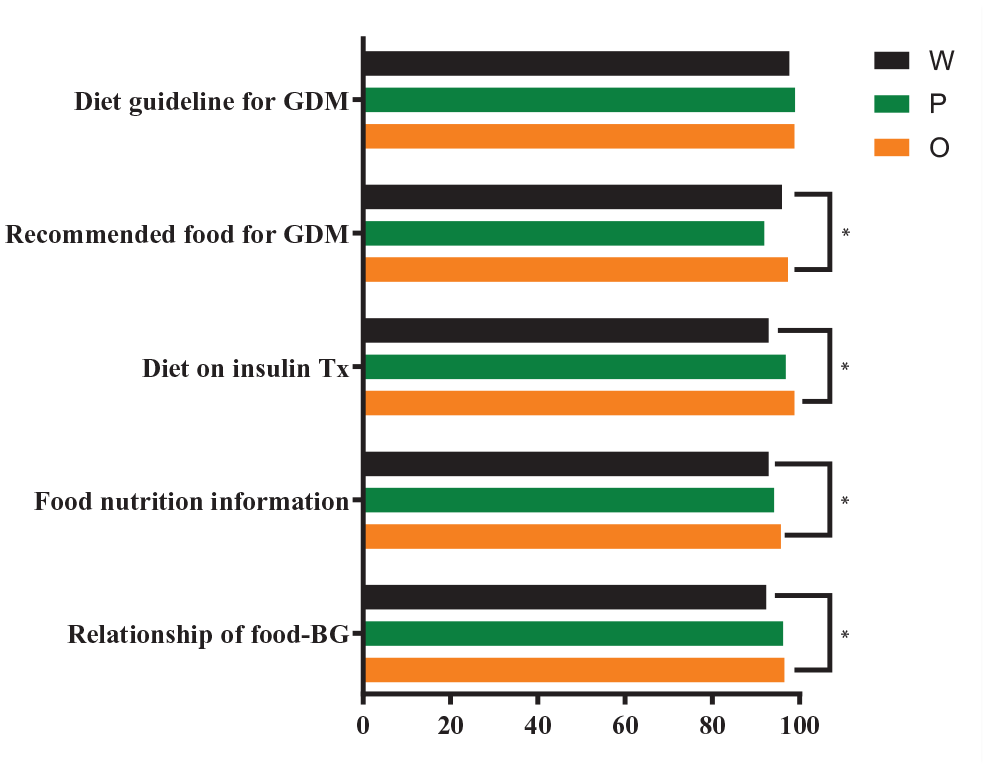
Essential Information about GDM required by participants in digital health systems.
Preferred mobile application features
Among listed features of mobile applications, “blood glucose log,” “insulin log,” “lab test retrieve function,” “meal diary,” and “fetal weight assessment” were most preferred by women. The requirement for recording blood glucose was highest in all 3 groups, followed by the requirement for recording insulin dose (Figure 3A). More physicians required recording insulin logs than women (Group W vs Group P: 92.3% vs 98.4%, p = .0141). Obstetricians’ requirements for recording maternal body weight were also higher than women’s (82.3% vs 93.0%, p = .0023 in Group W vs Group O) (Figure 4A and B).
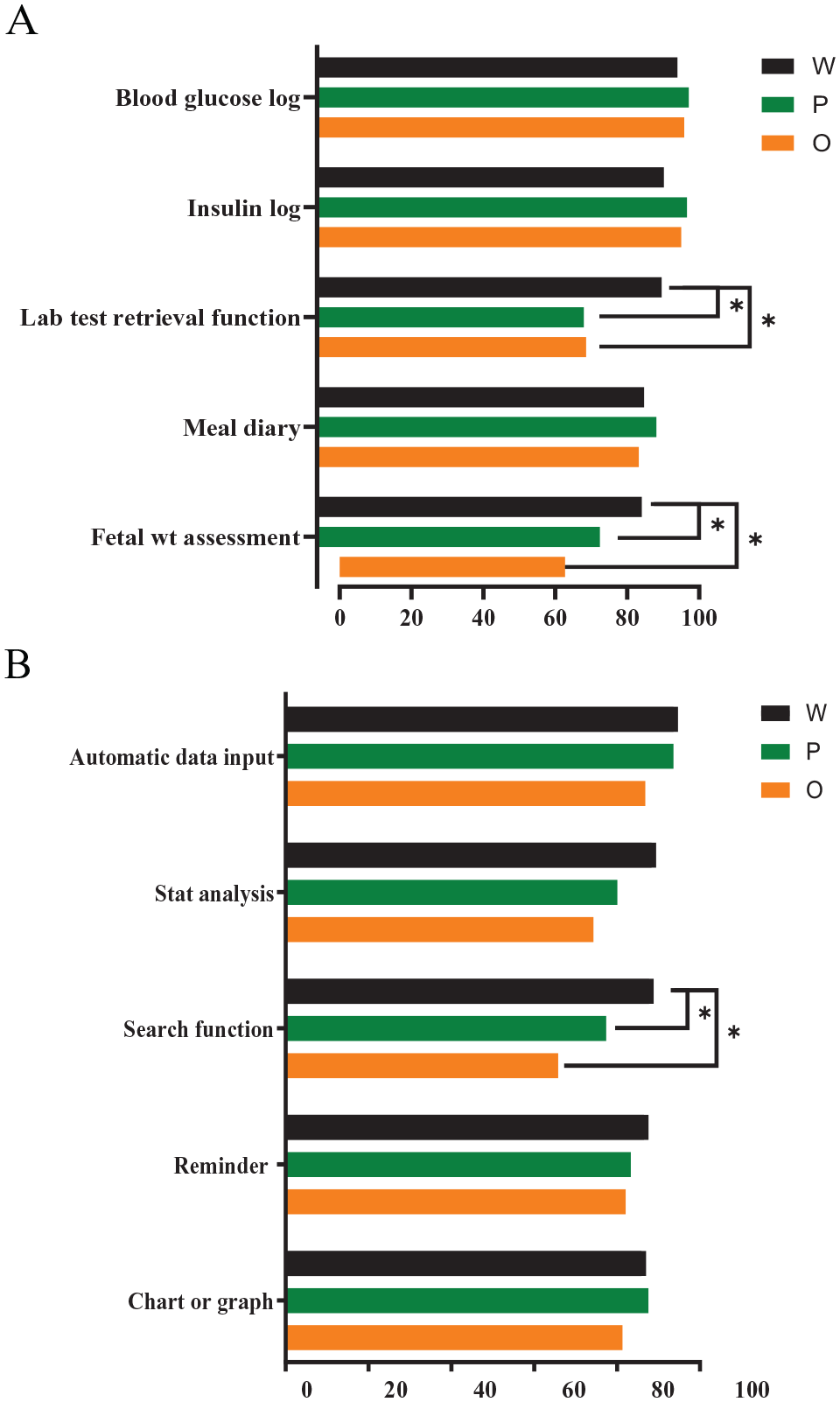
Preferred mobile application features by participants in digital health systems: (A) listed features based on previous study and (B) additional features preferred to be incorporated into the system.

Differences between preference of mobile application features by groups: (A) features with higher demand in women than HCPs and (B) features with higher demand in HCPs than women.
Among the additional features of the mobile application listed in the questionnaires, automatic data links from self-monitoring devices were highly required by all 3 groups (Figure 3B). The functions of statistical analysis of data, searching, reminders, and charting or graphing were highly required by women. Women required more automatic laboratory data result retrieval function than HCPs (Group W vs Groups P and O: 91.7% vs 71.0% and 71.6%, respectively, both p < .0001). In addition, “search and find function,” “assessing fetal weight,” “connection to the hospital when an emergency,” “personalized advice,” “direct communication with doctors,” “Q&A,” “recording the baby’s condition after delivery,” and “recording uterine contraction during pregnancy” were required more by women than by HCPs, showing significant differences in preferences between women and HCPs.
Discussion
In this study, both pregnant/postpartum women and HCPs recognized benefits of a digital healthcare system for pregnant women with GDM. However, preferences for features within the digital health system differed among the groups, and HCPs had a lower willingness to use this system in their clinics compared to pregnant/postpartum women.
Recent studies on digital health for managing GDM have shown that meeting the needs and preferences of both pregnant women and HCPs is important for the adoption and use of digital tools.20,21 Particularly, a cross-sectional survey conducted in Australia, found that about 80% of women with a history of GDM stated they would be open to using a health care application in the future if it were recommended by their HCP. 20 Differing from previous studies, our research provided details on specific application features to more effectively assess demand, thus addressing the specific needs of each group more precisely.
As expected, the most essential features for all groups were blood glucose log, insulin log, and automated glucose input. Pregnant/postpartum women needed an automatic function that could allow users to conveniently input their glucose levels without needing manual data entry. In a previous study, HCPs have also expressed positive feedback about this feature as it eliminates the need for paper diaries and enables faster decision-making by reviewing glucose levels before patient visits. 22 Furthermore, the use of an automated glucose input can improve user satisfaction and enhance patient compliance with self-measurement as demonstrated by a previous survey of patients using a mobile application with Bluetooth-enabled glucometer monitoring. 14 The prior systematic literature review also emphasizes that automated features, such as glucose logging, not only simplify patient monitoring but also strengthen self-management practices, ultimately aiding in achieving the overarching goal of improving health outcomes for both mothers and infants. 15
In this study, pregnant/postpartum women showed an active attitude toward self-management connected to healthcare by using healthcare mobile applications. Compared to HCPs, they expressed a stronger preference for certain features, such as lab test access, search functionality, emergency hospital connectivity, personalized advice, direct communication with doctors, and Q&A forums. They showed a strong willingness to take a proactive approach to managing their own health. They wanted to utilize digital healthcare system actively by monitor their health status, accessed updated information quickly and conveniently, easily communicated with doctors, and received expert opinions.
Pregnant/postpartum women also expressed a greater demand than HCPs for features related to their specific pregnancy aspects, such as assessing fetal weight, recording uterine contractions, and neonatal status. This indicates the importance of addressing their specific needs during pregnancy beyond just managing diabetes. Since this study includes the development of an application that covers management from early pregnancy to the postpartum period, it is anticipated to effectively meet the diverse needs of pregnant/postpartum women.
HCPs were more likely to consider tracking maternal body weight as an essential feature than pregnant/postpartum women. HCPs might place greater emphasis on proper weight gain during pregnancy as excessive or insufficient gestational weight gain is associated with an increased risk of adverse pregnancy outcomes, including macrosomia, LGA, neonatal hypoglycemia, cesarean delivery, and preterm birth. 23
Evaluating pregnant/postpartum women’s knowledge of GDM revealed high rates of correct answers regarding basic concepts, risk factors, and complications associated with GDM. However, their understanding of specific aspects related to GDM management, including the use of hypoglycemic agents, gestational weight gain, and postpartum diabetes care, was relatively low. A previous study has indicated that pregnant women commonly rely on digital sources for information, although they perceive them as less useful and trustworthy compared to professional sources. 24 It is important that pregnant women have access to accurate and reliable information to effectively manage their conditions during pregnancy. Providing comprehensive and easily accessible educational resources through a digital healthcare system, pregnant and postpartum women can be equipped with the knowledge necessary for successful GDM management.
Using questionnaires concerning the diagnosis and management of GDM among HCPs, it was found that a higher percentage of internal medicine physicians provided explanations regarding the need for screening postpartum diabetes and performing regular check-ups for GDM patients compared to obstetricians. This difference could be attributed to the fact that obstetricians primarily focus on GDM screening and management during pregnancy, while internal medicine physicians are more concerned about future development of diabetes in women with GDM than obstetricians.
Among group W, features identified as essential by participants who had prior experience of using healthcare applications were similar to those chosen by participants without such experience. However, the proportion of those who selected these features as “definitely need to provide” was higher among experienced users (data not shown). This suggests that individuals who have used healthcare applications in the past have a greater awareness of the importance and necessity of these digital healthcare features.
Digital healthcare system is experiencing rapid growth in many countries. It is expected to continue expanding significantly in the future. 25 Recently, several meta-analyses have shown the effectiveness of digital health interventions in managing GDM.12,26,27 As a result, the 2023 ADA guidelines now state that telehealth visits in the management of GDM can lead to better clinical outcomes than traditional in-person care. 28 These advancements indicate that the demand and usefulness of digital healthcare in GDM are expected to continue increasing.
However, HCPs showed less willingness to integrate these systems into their clinics than pregnant/postpartum women who wish to manage their health using digital health care system. This discrepancy is believed to be influenced by demographic characteristics: pregnant/postpartum women, with an average age of 34.3 years, are generally more accustomed to digital systems. In contrast, HCPs, who have an average age of 44 to 45 years, belong to a broader and more diverse age group, encompassing individuals who may not be as proficient with digital technology. This aligns with previous research indicating that many HCPs still perceive digital healthcare systems as relatively new and unfamiliar. 29 Additionally, while pregnant/postpartum women often need immediate medical assistance in urgent situations, HCPs might face psychological and time constraints when providing medical consultations outside of standard clinic hours. Similar concerns were reflected in other studies, where HCPs expressed worries about the extra time needed to use these systems and the potential for an increased workload.29 -31 Additionally, in the current state of undeveloped digital care in the domestic setting, HCPs may encounter challenges related to billing and taking responsibility in the event of issues.
In recent years, there has been a positive shift in perspective in the United States. The percentage of physicians who recognize the benefits of digital health tools for patient care has increased from 85% in 2016 to 93% in 2022. 30 Furthermore, the adoption of digital tools has seen a significant growth among all physicians. The average number of tools used had increased from 2.2 in 2016 to 3.8 in 2022. This indicates that more physicians now recognize the clear advantages of incorporating digital health systems into their medical practices. According to the American Medical Association (AMA) Digital Health Research 2022, primary factors driving physician interest in digital health systems are improved clinical outcomes and enhanced work efficiency. The most significant requirements for adopting digital healthcare tools are liability coverage, integration with their electronic health records (EHR), and ensuring data privacy. Furthermore, 1 study highlighted the necessity for further efforts to more effectively involve HCPs in the design and development of technology to enhance their engagement. 18
Therefore, a significant strength of this study is its approach to the development of digital healthcare for GDM management. By gathering opinions from not only pregnant/postpartum women but also obstetricians and internal medicine physicians who are currently involved in managing GDM, the study identifies the specific application features they require, and offers a comprehensive perspective on managing GDM. Also, the involvement of a considerable number of participants, approximately 600 individuals, strengthened this study.
However, this study had several limitations. First, there might be a selection bias. Participants might have been more motivated and expressed more positive attitudes compared to nonparticipants. In addition, selected participants might not have represented all pregnant/postpartum women and HCPs in general. About 70% of the women in Group W had no prior experience with diabetes, potentially impacting the relevance of their responses to detailed aspects of a potential digital health applications. However, the survey was conducted anonymously, allowing participants to freely express their opinions.
This study has demonstrated that both pregnant/postpartum women and HCPs show positive attitudes toward the use of digital tools in the management of GDM. Additionally, it identified which functionalities both pregnant/postpartum women and healthcare providers consider important within the digital health system. These findings emphasize the need for HCPs to actively incorporate digital tools in managing GDM and to provide personalized education and management plans. Additionally, future research should further assess the effectiveness of digital tools and investigate the impact of specific features on patient health outcomes.
Conclusion
Both pregnant/postpartum women and HCPs acknowledged the benefits of utilizing a digital healthcare system for managing GDM. This study showed differences in perspectives among these groups, as well as the current status of GDM screening and management among HCPs. These findings provide valuable guidance for the development of a digital-based GDM management system aimed at improving short- and long-term outcomes of GDM. Future research could focus on developing a GDM digital healthcare system based on these findings and evaluating its effectiveness, user satisfaction, and clinical outcomes among pregnant/postpartum women and HCPs.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241252569 – Supplemental material for Demand and Requirements for a Digital Healthcare System to Manage Gestational Diabetes in Patients and Healthcare Professionals: A Cross-sectional Survey
Supplemental material, sj-docx-1-inq-10.1177_00469580241252569 for Demand and Requirements for a Digital Healthcare System to Manage Gestational Diabetes in Patients and Healthcare Professionals: A Cross-sectional Survey by Jin Yu, Oyoung Kim, Byung Soo Kang, Seon Ui Lee, Youn Ju Lee, Han Sung Hwang, Seung Mi Lee, Seung Chul Kim, Yoon-Hee Choi and Hyun Sun Ko in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580241252569 – Supplemental material for Demand and Requirements for a Digital Healthcare System to Manage Gestational Diabetes in Patients and Healthcare Professionals: A Cross-sectional Survey
Supplemental material, sj-docx-2-inq-10.1177_00469580241252569 for Demand and Requirements for a Digital Healthcare System to Manage Gestational Diabetes in Patients and Healthcare Professionals: A Cross-sectional Survey by Jin Yu, Oyoung Kim, Byung Soo Kang, Seon Ui Lee, Youn Ju Lee, Han Sung Hwang, Seung Mi Lee, Seung Chul Kim, Yoon-Hee Choi and Hyun Sun Ko in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
Statistical analysis was performed by biostatisticians(Hana Kim) employed by a contract research organization, Medical Excellence Inc. A portion of this study was presented as an abstract form at the 36th Spring Conference of the Korean Diabetes Association, May 11 to 13, Gwangju, Korea and at the 29th Conference of Korean Society of Maternal Fetal Medicine, June 3, Seoul, Korea. The authors would like to thank all participating women and healthcare professionals. We also thank the members of Gestational Diabetes Research group in Korean Society of the Maternal-Fetal Medicine, Korean Diabetic Association, Korean Society of Obstetrics and Gynecology.
Author Contributions
Conception or design: J.Y., O.K., B.S.K., H.S.K., Y.H.C. Acquisition, analysis, or interpretation of data: J.Y., O.K., B.S.K., S.U.L., Y.L., H.S.K., Y.H.C. Drafting the work or revising J.Y., O.K., H.S.K., Y.H.C. Review and approval of the manuscript J.Y., O.K., B.S.K., S.U.L., Y.L., H.S.H, S.M.L., S.C.K., H.S.K., Y.H.C. Final approval of the manuscript: J.Y., O.K., H.S.K., Y.H.C.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by the “National Institute of Health”(No. 22ER080800).
Ethical Approval
Institutional Review Board (IRB) of Seoul St, Mary’s Hospital, the Catholic University of Korea (approval number: XC23OIDI0012).
Guarantor
H.S.K
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.