
Abstract
Introduction
The International Diabetes Federation has identified the emergence of gestational diabetes mellitus (DM) (GDM) as an underappreciated threat to maternal and child health. Adequate knowledge, a positive attitude towards prevention, and a positive perception of its danger could motivate pregnant women to take preventive measures. However, there is a dearth of literature on these among women attending antenatal clinics at UCH. This study, therefore aimed to assess pregnant women’s knowledge about GDM, report their attitudes and determine their perception towards GDM.
Methods
A cross-sectional study assessed the knowledge, attitude and perception towards GDM. A total of 300 pregnant women registered with and attending the antenatal clinic in University College Hospital (UCH), were selected using a random sampling technique. A self-structured questionnaire using a GDM Knowledge Questionnaire and previous research questions on Perception and Attitude was used to collect data from participants. Data were analysed using Statistical Package for Social Sciences 20.0 and hypotheses were tested using chi-square at 0.05 level of significance.
Results
The mean age of the pregnant women was 30.60 ± 5.88 years. A little over one-fifth of the participants were knowledgeable about GDM. Three-quarters of the participants demonstrated a positive attitude while just a little over half had a positive perception of GDM. A significant association exists between participants’ knowledge about GDM and belief about screening for diabetes during pregnancy (p = .006). There was a significant association between participants’ attitude and their perception of GDM (p = .000). A direct significant association was also found between participants’ knowledge and their perceived risk of developing GDM (p = .000).
Discussion
While most of the pregnant women had poor knowledge about GDM, more than half of the pregnant women had positive attitudes towards GDM. A little over average possesses a positive perception towards GDM. Healthcare providers should intensify efforts in formulating appropriate methods to increase awareness with emphasis on the risks associated with GDM.
Introduction
Diabetes mellitus (DM) is a chronic metabolic condition caused by a lack of insulin synthesis by the pancreas due to an inherited or acquired deficiency, or by the ineffectiveness of the insulin generated. 1 It is characterised by high glucose levels in the blood, which harm many of the body’s systems, including the blood vessels and neurons. 1 DM has progressively become a widespread occurrence. A condition that occurs during pregnancy, gestational DM (GDM) is a subtype of DM. It is diagnosed when women without any history of DM exhibit high blood glucose levels during pregnancy, especially during the third trimester. 2
GDM is any degree of glucose intolerance that results in a hyperglycaemic state of variable severity, with its first occurrence during pregnancy, no matter the treatment required or postpartum evolution. 3 This definition includes DM that predates pregnancy. The International Diabetes Federation has identified the emergence of DM for the first time during pregnancy, also known as GDM, as a severe and underappreciated threat to maternal and child health. 4 GDM is any degree of glucose intolerance with onset or first recognition during pregnancy. 5 Over the past decade, the prevalence of GDM has been accelerating worldwide constituting a rising public health concern. In 2017, an estimated 21.3 million (16.2%) live births had hyperglycaemia during pregnancy, of which GDM contribution was 85.1%. 4
Globally, DM is one of the top 10 leading causes of mortality among women causing 2.1 million deaths per annum. 4 DM in pregnancy has become a great concern to medical practice globally. Its complications for the mother and foetus/baby are leading causes of maternal and perinatal mortality. 6 It seriously affects the patient, immediate family members, and the entire community. It is pertinent to diagnose and effectively manage DM during pregnancy as it raises the danger of maternal and postnatal morbidity.7, 8
The prevalence of DM especially during pregnancy is increasing worldwide hence, current data shows that the prevalence rate of DM in pregnancy is 15%. 9 The prevalence rate of GDM varies from 5.4% in Europe 10 to 11.5% in Asia. 11 Also, the pooled prevalence of GDM in Africa was 13.61% and 14.28% in the sub-Saharan African region. A review using different screening and diagnostic criteria revealed the incidence of GDM in sub-Saharan Africa to be 14% 12 with that of Middle East and North Africa ranging from 8.4% to 24.5%. 13 The occurrence of GDM was highest in Central Africa with a percentage of 20.4%, and with the lowest in Northern Africa sub-regions, 7.57%. 14 In Nigeria, the prevalence of DM in pregnancy was 13.6%. 15 Existing data within Nigeria revealed that Lagos has the highest prevalence of DM in pregnancy (23.2%). 16
Hyperglycaemia caused by GDM or a history of diabetes is linked with various maternal and foetal pregnancy complications. The complications include increased incidence of caesarean section, gestational hypertension, pre-eclampsia, foetal macrosomia, sudden intrauterine death, birth trauma and increased neonatal morbidity. 17 The risk is high, incessant, and has important significance for public health. The majority of these occurrences of hyperglycaemia in pregnancy were reported in low- and middle-income countries, where health workers are ill-equipped to deal with such situations and maternal health services are still underutilised. 4
A study to assess gestational diabetes awareness among Saudi women revealed a fair knowledge about GDM amongst the majority of the women (54.8%). 8 Also, regarding the correct knowledge of GDM, Elmekresh et al. discovered that awareness was generally poor in a study carried out among women of childbearing age. 18 Only a few of the pregnant women attending antenatal clinics in the Western Province of Sri Lanka had good knowledge (20%) about GDM, however, more than 50% showed a positive attitude towards the management of GDM. 19 A keen awareness and a positive attitude of pregnant women towards gestational diabetes will be effective in early detection, disease prevention and lesser complications. 20 With the appropriate knowledge, adequate perception and positive attitude towards GDM manifested as healthy eating habits, weight control and regular exercise, the complications of GDM can be prevented, permitting mothers to live a better life with their offspring. 21
Akinwaare et al. in a study to determine the perception of risk and knowledge of preventive measures among pregnant women found out that even though the majority of the pregnant women had poor knowledge of GDM as well as it preventive measures, most of the women perceived themselves to be at low risk. 22 Knowledge of any condition is only complete if the individual can comprehend all the associated factors of the particular condition. Meanwhile, poor awareness about GDM results in poor preventive and management strategies. 23 Within the context of the increasing prevalence of GDM, knowledge regarding its management, prevention and control has a critical role. 24 GDM is associated with many morbidities, cognisance of the dangers and prompt screening of mothers could be beneficial in abating the complications that present with diabetes in pregnancy. 25 A better understanding of GDM among pregnant women will assist in planning interventions that would promote a healthy lifestyle among the women and improve practices of better health-seeking behaviours. Consequently, it is necessary to step up efforts to enhance and improve knowledge and perception of DM among pregnant women in Ibadan, Nigeria.
Good knowledge about DM in pregnancy could assist diabetic pregnant women in coping and adjusting well to their medical condition. 8 Although studies have reported a high prevalence of DM in pregnancy in Nigeria (especially South Western Nigeria), Nigeria has little data on the level of knowledge about DM in pregnancy. 2 The University College Hospital, Ibadan is one of the largest hospitals in Nigeria. Many women, particularly the elite attend the clinic and it was observed that quite a number of women attending the University College Hospital’s ante-natal clinic appear obese. This might pose a risk of developing diabetes during pregnancy. This study, therefore seeks to determine the knowledge, attitude and perception of pregnant women towards GDM.
Objectives of the Study
The specific objectives of the study are:
To assess knowledge of GDM among pregnant women attending antenatal clinics in University College Hospital (UCH). To report the attitude towards GDM among pregnant women attending antenatal clinics in UCH. To determine the perception of GDM among pregnant women attending antenatal clinics in UCH.
Method
Study Design
A cross-sectional study aimed at assessing the knowledge, attitude and perception towards GDM among pregnant women attending the antenatal clinic in University College Hospital, Ibadan.
Population
This study’s population comprises of 300 pregnant women randomly selected during ante-natal clinic days at University College Hospital, Ibadan.
Inclusion criteria: Pregnant women registered and attending UCH ante-natal clinic.
Exclusion criteria: Pregnant women too ill to participate, pregnant women with mental disability.
Sampling Technique
The University College Hospital conducts its ante-natal clinic two days in a week and a booking day every week. On the ante-natal clinic days, different pregnant women are scheduled to come for ante-natal check-ups while new pregnant women come for registration on the booking day. The hospital was visited on ante-natal days and booking days. Using a simple random sampling method, 300 pregnant women who met the inclusion criteria were randomly selected and questionnaires were administered until the sample size was met.
Instrumentation and Procedure
A self-structured questionnaire using a GDM Knowledge Questionnaire (GDMKQ) and previous research questions on Perception and Attitude was used to collect data from participants to assess their knowledge, attitude and perception of GDM. It consisted of four sections. Section to elicit data on the demographic variables, Section B to assess knowledge of GDM among participants, Section C to determine the perception of GDM among participants and Section D to report the participants’ attitude towards GDM. The knowledge score of participants below the 75th percentile of 12 was categorised as not knowledgeable. The mean value score was used to categorise positive and negative attitudes among participants. The perception score of the participants above the mean score was categorized as positive perception.
Validity of Instrument
The questionnaire was constructed using a GDMKQ as a guide and based on information from literature review and empirical findings, using the objectives of the study as a guide. The questionnaire was submitted to the research supervisor and an expert in the field of study for a thorough assessment of the instruments’ content and face validity.
Procedure for Data Collection
An official letter of introduction and permission to collect data was obtained from the Head of Nursing Department, University of Ibadan. Ethical permission was obtained from the UI/UCH Health Ethical Review Committee. On arriving at the ante-natal clinic on clinic day, the nurses on duty were informed about the data collection process and for a proper introduction to the pregnant women. After the routine health talk, the women were informed and implored to be a willing participant in the data collection process. Subsequently, pregnant women were approached personally with a detailed explanation of the purpose of the research study and willing women filled out the questionnaire. The administration of questionnaires was within the hours of 9–11 a.m. during the visit to the clinic. This is to ensure that the women were well-rested and composed after their arrival. Participation was voluntary and questionnaires were administered to those participants who met the inclusion criteria. The respondents were given questionnaires and expected to fill within 10–15 minutes and then return the questionnaire on the spot. This was done after consent had been given.
Ethical Considerations
A summary of the study protocol was submitted to the University of Ibadan/University College Hospital Health Ethical Review Committee to seek permission to carry out this study and approval was given with approval number UI/EC/21/0356. Consent was obtained from participants before the study. Privacy, confidentiality and anonymity were ensured. The scientific objectivity of the study was maintained with honesty and impartiality.
Data Analysis
Data collected were analysed using SPSS version 20.0 (Statistical Package for Social Sciences 20.0). Descriptive statistics such as percentage representations, charts, tables and figures were used to present results, while inferential statistics, with the use of Chi-square and Fisher’s exact tests, was used to determine the significant relationship between independent and dependent variables and results.
A total of 12 questions were used to assess the knowledge of GDM among participants. The cumulative score of each respondent was summed up, with a maximum obtainable score of 24. The 75th percentile of 12.0 was used as a cut-off mark for good or poor knowledge.
For attitude towards GDM, respondents’ responses on attitude are provided using a 3-point Likert scale, the scoring of the scale was: 1 = strongly agree, 0 = neutral, 0 = strongly disagree with a maximum obtainable score of five. The lower score of the mean value was used to categorize positive and negative attitudes in the study following analysis.
A total of eight questions were used to assess the perception of GDM among participants with a maximum obtainable score of seven. The mean score obtained was then used as the cut-off mark to determine negative and positive perceptions.
Results
Table 1 shows that the majority of the participants 53.3% were below or equal to age 30, 52.7% were Higher National Diploma (HND) holders and 74.7% had no family history of diabetes.
Socio-demographic Information of Study Participants.
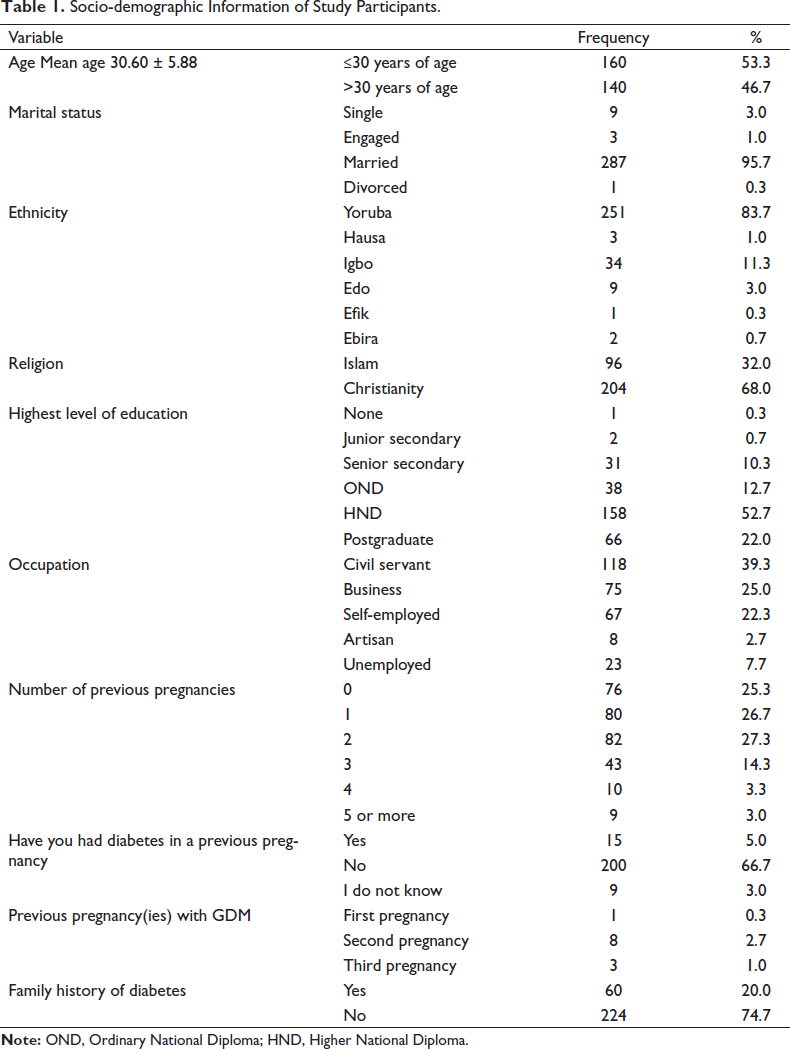
Table 2 shows that the majority of the participants (75.7%) had heard about GDM with health workers constituting the major source of information (29.7%). It also shows that 147(49%) knew that GDM is diagnosed during pregnancy.
Knowledge of GDM Among Participants.
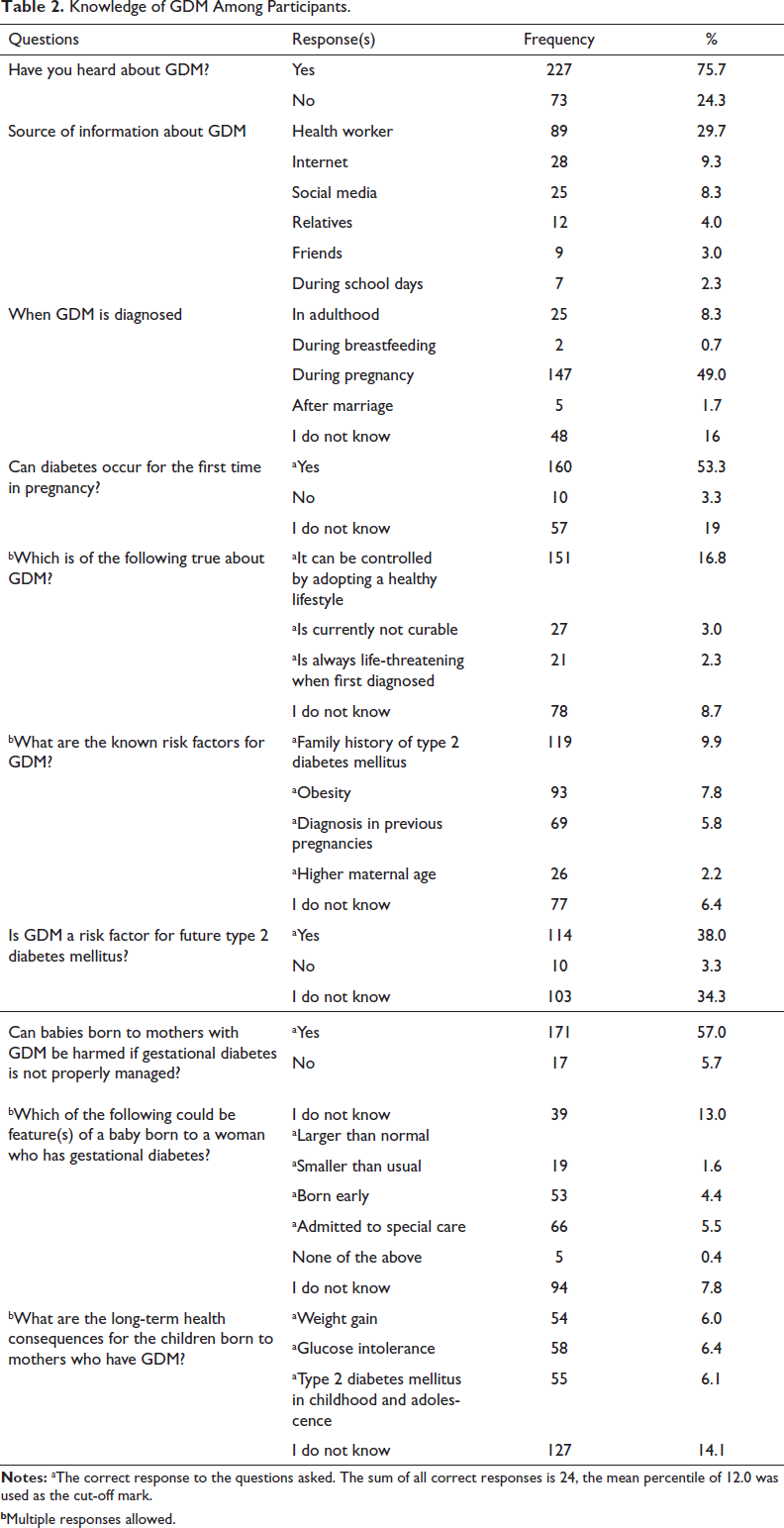
bMultiple responses allowed.
Descriptive statistics on knowledge level about GDM reveal that 78.7% (236) of participants were not knowledgeable about GDM while 21.3% (64) were. This is demonstrated in Figure 1.
Level of Knowledge About GDM Among Participants.
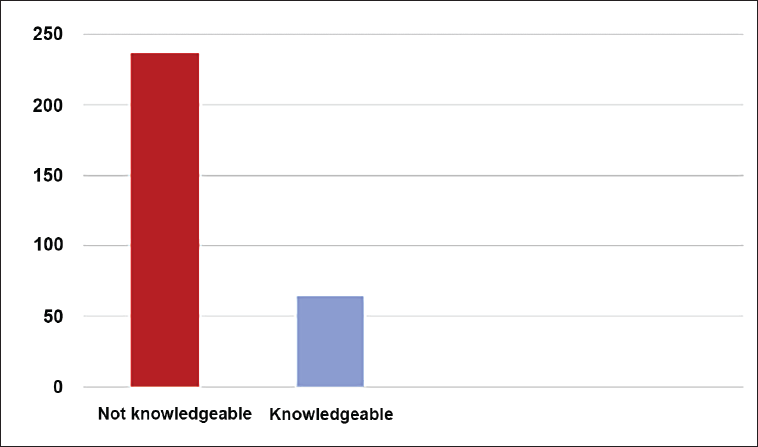
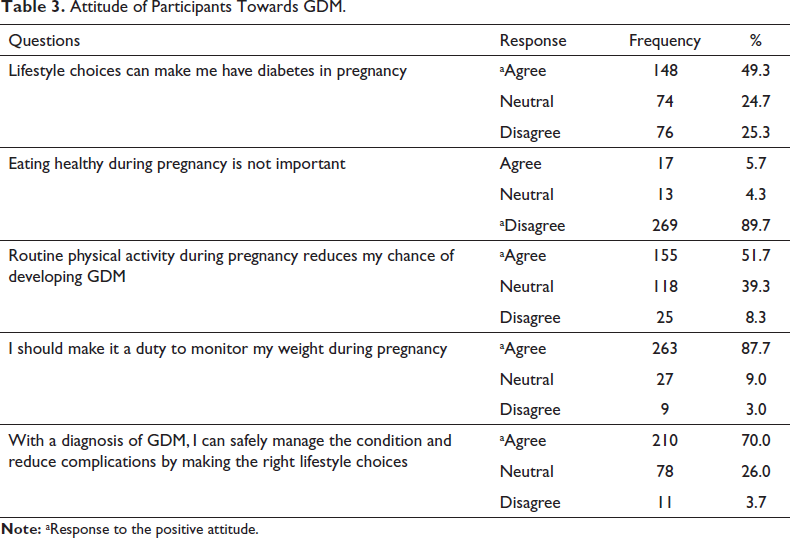
Table 3 shows that the majority of the participants 87.7% agreed that it should be a duty to monitor weight during pregnancy. The majority (70%) also agreed that by making the right lifestyle choices, one can safely manage the condition and reduce complications with a diagnosis of GDM.
Attitude of Participants Towards GDM.
Descriptive statistics on attitude towards GDM (Figure 2) reveal that the majority of participants 75% (225) showed a positive attitude towards GDM meanwhile 25% (75) demonstrated a negative attitude.
Participants’ Attitude Towards GDM.
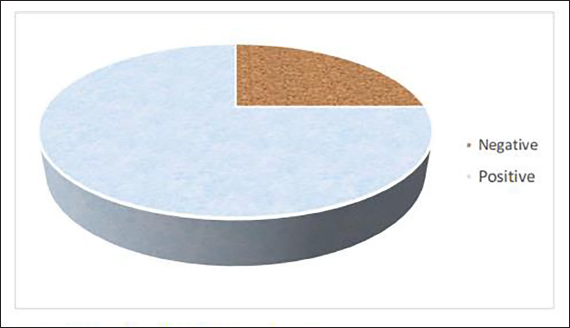
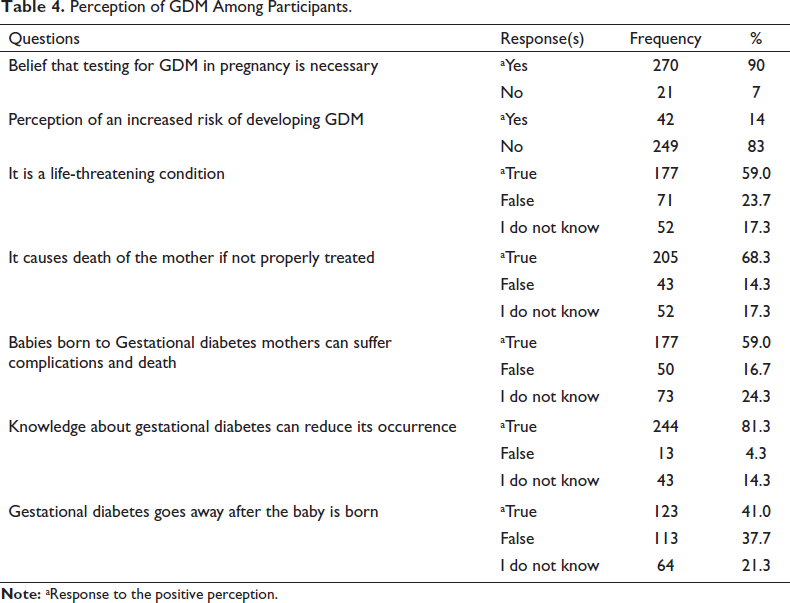
Table 4 above shows that only 42 (14%) of respondents perceive themselves at an increased risk of developing GDM while 249 (83%) do not, and 59% of participants believe GDM is a life-threatening condition.
Perception of GDM Among Participants.
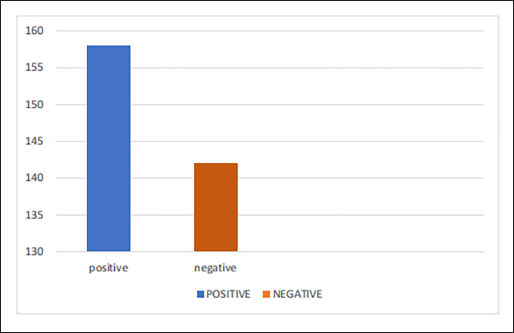
Descriptive statistics on the perception of GDM (Figure 3) reveal that a little over half of the participants 52.7% (158) had a positive perception of GDM meanwhile 47.3% (142) had a negative perception.
Perception Towards GDM Among Participants.
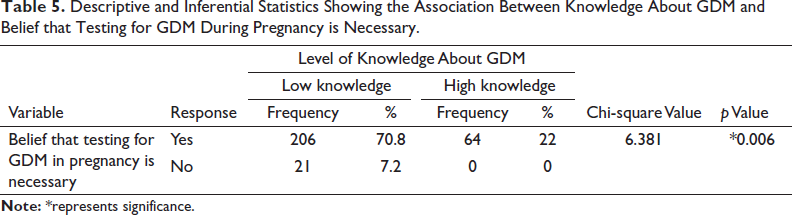
Results reveal that there was a significant association between the level of knowledge about GDM and their belief that testing for GDM during pregnancy to be necessary with a p value <.05 (0.006, X 2 = 6.381) (Table 5).
Descriptive and Inferential Statistics Showing the Association Between Knowledge About GDM and Belief that Testing for GDM During Pregnancy is Necessary.
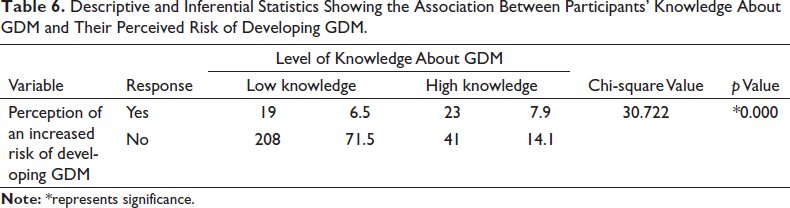
Results reveal that there was a significant association between the level of knowledge about GDM and their perceived risk of developing GDM with a p value <.05 (0.000, X 2 = 30.722) (Table 6).
Descriptive and Inferential Statistics Showing the Association Between Participants’ Knowledge About GDM and Their Perceived Risk of Developing GDM.
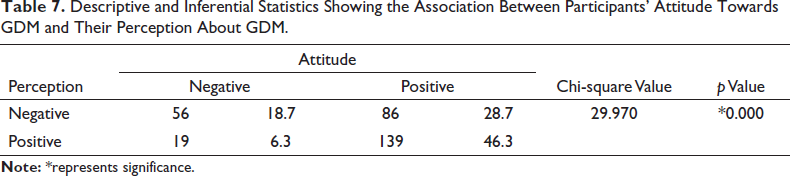
Results reveal that there was a significant association between participants’ attitude towards GDM and their perception about GDM with a p value <.05 (0.000, X 2 = 29.970) (Table 7).
Descriptive and Inferential Statistics Showing the Association Between Participants’ Attitude Towards GDM and Their Perception About GDM.
Discussion
This study reported that over three-quarters of the respondents were not knowledgeable about GDM. Consequently, this is reflected in participants’ knowledge of GDM risk factors, complications suffered by the baby, its prevention and management. This finding is not too different from that of Elmekresh et al. 18 where the majority of the participants’ GDM knowledge was graded as fair. Also, Lakshmi et al. 26 in a study to assess the knowledge about GDM among antenatal mothers in urban Chidambaram also found out that only one-fifth of its participants had adequate knowledge about GDM.
Results from Ogu et al. 2 showed that the majority of women of reproductive age in five local government areas in Rivers State had heard about DM with the major source of information on GDM being friends and health workers respectively. Similar to Ogu et al.’s study, health workers constituted one-third of the major sources of information on GDM among respondents in this study. This reveals that health workers are and can continue to be major change agents regarding increasing awareness and knowledge of GDM. Also, this study revealed that about half of the respondents knew that diabetes could occur for the first time during pregnancy, which is different from the study of Ogu et al., where just over a third of participants were aware of this. This can be related to the fact that the majority of the women in the latter study received their information from friends; hence it may not be as detailed compared to information obtained from a health worker.
The distribution of participants’ sources of information about GDM from this study showed that most of the participants that have heard about GDM obtained their information from health workers, followed by the internet with the least source to be during school days. The finding is consistent with that of Price et al. 27 to investigate the awareness of GDM and its risk factors among pregnant women, where doctors constituted a greater percentage as the source of information about GDM. Conclusively, both findings reveal very little impact of the role of the medical professionals as the overall knowledge about GDM still remains poor among the respondents. This only implies that health workers have not adequately impacted knowledge about GDM to pregnant women attending antenatal clinics.
The majority of the pregnant women in this study had poor knowledge about GDM, yet more than half of the participants perceived the condition to be life-threatening. According to Katavic et al., 28 illness perceptions are created by integrating medical information into pre-existing understanding, experiences and memories of health and illness. Hence, despite uncertainty about what GDM is all about, the majority of the women incorporated their understanding of medical diagnosis to develop a positive risk perception towards GDM. Furthermore, factors influencing the way the public views and perceives health risks may vary especially if the risk in the question evokes feelings of dread, if the issue is not well understood, whether the issue involves a lot of uncertainty, if it is subject to personal control or if it is familiar. 29 This study also reported that over one-third of pregnant women believe GDM to go away after the baby is born. Similarly, findings from a study conducted by Elamurugan and Arounassalame 30 to determine the awareness of GDM among antenatal mothers, revealed that very few of the mothers believed that GDM disappears after pregnancy.
This study was conducted in a tertiary hospital located in an urban area with educated patients. Findings reported that the majority of the pregnant women attending the antenatal clinics the hospital had a positive attitude towards GDM. Davoodi et al. 20 in his study also recorded a good attitude towards GDM among pregnant women referred to health centres in a city in Iran. When asked about their attitude towards eating healthy and routine physical activity during pregnancy, this study showed that a good percentage of the pregnant women agreed that eating healthy during pregnancy is essential while a little over half agreed with routine physical activity reducing their chances of developing GDM. Monir et al. 31 while assessing the attitude of pregnant women towards eating healthy and routine physical activity during pregnancy, found out that more than half of the pregnant women maintained a meal plan during pregnancy while a little below half of them carried out physical exercise during pregnancy. Also, Price et al. 27 showed that most women recognized eating a healthy diet and regular physical activity as appropriate lifestyle changes to help prevent GDM.
The study revealed a positive perception of a little over average about GDM among pregnant women attending antenatal clinics in UCH. This is supported by the large number of participants who believe in testing for diabetes in pregnancy, perceive it as threatening to the mother and baby, and believe that knowledge about it can reduce its occurrence. This finding is, however, different from that of Akinwaare et al. (2020) conducted among different selected health facilities in Ibadan where a little over half of the participants had a low perception of risk of diabetes in pregnancy. Akinwaare et al. conducted the study in the year 2017 across selected health facilities of different levels of institutions, and pregnant women attending antenatal clinics in UCH (tertiary hospital) constituted only about a third of the study population.
There was a statistically significant association between knowledge about GDM among pregnant women attending the antenatal clinic in University College Hospital, Ibadan and their belief about testing for diabetes during pregnancy to be necessary. The majority of the women exhibited poor knowledge about the condition and at the same time majority considered testing for diabetes to be necessary in pregnancy. This finding is consistent with that of Bhavadharini et al. 32 to evaluate the knowledge of GDM amongst pregnant women in South Tamil Nadu and Ogu et al. 2 study to determine GDM knowledge among women of reproductive age in southern Nigeria. In both studies, majority of the women exhibited poor overall knowledge about GDM, yet a greater percentage considered testing for diabetes in pregnancy to be essential. Logically, most of the women in the above-cited studies possessed vague knowledge on what GDM is, however, most of the women are well-educated enough to understand the threat the condition poses and automatically they all believe that screening for the condition is vital.
A statistically significant association between knowledge about GDM among pregnant women attending antenatal clinics in University College Hospital, Ibadan and their perceived risk of developing GDM. This is consistent with that of Akinwaare et al. 22 in a primary healthcare centre which also reported poor knowledge of GDM among more than half of the participants and a good perception of the risk of developing diabetes in pregnancy amongst the minority. There is a statistically significant association between the attitude of pregnant women attending antenatal clinics in UCH towards GDM and their perception of GDM. According to Weinman and Petrie, 33 the way in which patients perceive their illness is a key factor in the type of psychological reaction they have to the illness and subsequent behaviour and attitude towards it.
Limitation of the Study
Due to inadequate funding and time constraints, only pregnant women attending the antenatal clinic at University College Hospital, just one of the many antenatal clinics, were sampled. This might limit the generalisability of the findings from this study.
Conclusion
Based on the results, the majority of pregnant women attending the antenatal clinics in University College Hospital, Ibadan were not knowledgeable about GDM. Findings from the study also showed that the majority of the pregnant women attending the antenatal clinic in University College Hospital, Ibadan have heard about GDM, mostly from health workers.
Also, more than half of the pregnant women had a positive attitude towards GDM, as the majority agree that making the right lifestyle choices can safely manage a diagnosis of GDM and reduce complications. The study also reported a little over the average positive perception towards GDM with most participants believing they are at a lesser risk of developing GDM.
Recommendations
Based on the findings of this study, the following recommendations will be put forward for policy implementation:
Findings from this study report knowledge about GDM is poor amongst pregnant women attending antenatal clinic in UCH with little knowledge attributed to information from health workers. It is recommended that healthcare professionals should be proactive and further intensify efforts on the education of pregnant women about GDM. The most significant proportion of women received information about GDM from health workers. Thus adequate clinic time should be dedicated to educate the women attending the antenatal clinic. Findings from the study can help healthcare providers in the successful implementation of activities of GDM programs and in formulating appropriate techniques.
Also, the positive effects of the mass media should be explored and the media as a tool to intensify and spread information about GDM with emphasis on the causes, risk factors and complications associated with GDM. Early education before pregnancy can also be done. Women of reproductive ages can be educated beforehand about DM in pregnancy so that appropriate measures can be taken throughout pregnancy and pregnant women can easily adapt to and comply with positive health-promoting behaviours during pregnancy.
Footnotes
Acknowledgements
This article was supported by Salako Abdulbaqhi, Salman Aonat, Kazeem Aisha, Adebimpe Ibukunoluwa and Jegede Christianah. The authors also thank Bunmi Olatoye for her timely input to the study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical Approval
Ethical approval was sought and gotten from University of Ibadan/University College Hospital Health Ethical Review Committee (Approval number- UI/EC/21/0356).
Funding
The research was self-funded.
Informed Consent
Informed consent was obtained from participants prior to the study.