
Abstract
This study investigated the perceptions of Iraqi patients regarding Electronic Healthcare Records (EHRs) in terms of trust and propensity to share and exchange medical and personal information and data within the healthcare ecosystem. During the period of April to June 2022, a researcher-assisted questionnaire was disseminated to adult Iraqi patients attending public or private healthcare facilities in a subset of Iraqi governorates. Data collection was followed by descriptive and inferential analyses. In total, 552 respondents filled out the questionnaire. The findings revealed that 71.6% of respondents were conversant with EHRs and trusted them as data collection and storage systems. In addition, 10% of respondents did not want their EHRs to be shared between healthcare professionals and institutions. However, only 3.6% of participants were willing to share all of their personal information with healthcare professionals. Female respondents were considerably more willing to share their full names with healthcare professionals than male respondents, despite the society’s reputation for conservatism. The findings of this study highlighted the necessity of tailoring initiatives to enhance patients’ trust in EHRs and their interactions with healthcare professionals other than medical physicians.
Little is known about patients’ perspectives and experiences with Iraq’s healthcare information system.
To the authors’ knowledge, this is the first study to explore Iraqi patients’ perceptions and trust toward EHRs.
The general impression indicated that work still needs to be done to investigate the Iraqi population’s perceptions toward the privacy and security of EHRs.
Introduction
Historically, capturing and recording patient-related data and information has always been a part of medical practice.1,2 Over the years, medical data documentation has evolved from Hippocratic case reports to Al-Razi’s method of didactic case histories to the current systematic medical data collection and documentation approach. 2 In the 1920s, health records were fully integrated into medical practice. 1 In the United States, the Regenstein Institute was the first medical institution to transition from papyrus to electronic health records in 1972. 3 The early EHRs were influenced by Dr. Lawrence Weed’s Problem-Oriented Medical Records (POMR).4,5
When discussing electronic health records, 3 key terminology must be defined and distinguished: electronic health records (EHRs), electronic medical records (EMRs), and personal health records (PHRs). EHRs are patient-centered, real-time records that give quick and secure information to authorized users. EHRs often include a patient’s medical history, diagnoses and treatment, medications, allergies, immunizations, radiological pictures, and lab results. 6 Conversely, EMRs are partial health records maintained by a healthcare provider(s) that contain a portion of a person’s essential health information across their lifetime. Personal medical records that are provider-centric or health-organization-centric are known as EMRs. Finally, personal health records (PHRs) are complete or partial health records held by an individual (eg, a patient or family member) that contain all or portion of that person’s pertinent health information.7,8
EHRs are the most comprehensive health records. EHRs contain all pertinent health information about a person over the course of their life. Many healthcare practitioners, organizations, and institutions can access and use EHRs. Furthermore, EHRs, unlike EMRs, can be accessed and used by practitioners outside of healthcare organizations. As a result, EHRs are critical in healthcare policy development and implementation.6,9
EHR systems include a multitude of capabilities that can greatly enhance care quality, reduce operational costs, and increase patient satisfaction with given care and services.10,11 The capabilities of EHR systems are connected to clinical decision-making support, computerizing doctor orders, and communicating health information and data. 12 There are numerous advantages and benefits of integrating EHR technology into medical practice. EHRs provide multidimensional value since they benefit patients, practitioners, organizations, national healthcare systems, and society. 13
At the level of an individual patient, EHRs provide fast and comprehensive documentation of the patient’s medical history. 14 EHRs give practitioners with rapid, accessible, and timely access to patient records and medical charts. 15 Furthermore, EHRs have the potential to improve the efficiency of healthcare processes and procedures because they enable fast and accurate communication between different levels and facilities of healthcare systems, including primary, secondary, and tertiary care.6,15,16 Finally, thorough and accurate EHR integration could give the necessary data and knowledge to develop suitable and effective national health policies and initiatives.6,16
Clinical outcomes have shown that EHRs reduce medical errors by using computerized prescription entry, predicting drug interactions and displaying a warning for the healthcare provider, assisting clinicians in reconciling patient medications, and, most importantly, maintaining a detailed and legible medical record. 17 In terms of organizational elements, EHRs could help to increase and maximize total profitability and revenues, improve cash flow, assist clinicians in appropriately documenting patient charges on time, and boost overall organizational efficiency.18 -20 Finally, the societal benefits of EHR systems include faster research, contributions to public health campaigns and initiatives, and improved patient care.13,21
While EHR systems have numerous benefits, they also have a number of drawbacks and flaws. These drawbacks are related to financial concerns, workflow changes, temporary loss of productivity associated with EHR adoption, privacy and security concerns, and a number of unforeseen consequences.13,19,22
Since 2003, the Iraqi healthcare system has faced numerous obstacles that have hampered patients’ access to healthcare, the quality of care offered, and overall clinical outcomes. As a result, healthcare system regulators have implemented a number of initiatives to address these issues. Integrating and installing EHR systems is one of the recently adopted interventions, it was introduced in 2014. Adoption of EHR systems in Iraqi healthcare systems necessitates extensive research and understanding of their clinical, organizational, and societal outcomes. Patients’ acceptance, attitudes, and experiences with EHR systems are among the societal effects. According to the available research and literature, successful EHR integration is heavily dependent on patients’ acceptance, views, and experiences with these systems.23,24 Little is known about patients’ perspectives and experiences with Iraq’s healthcare information system. To the best of the authors’ knowledge, no empirical study has analyzed or investigated Iraqi patients’ perceptions of and trust in EHR systems. As a result, it is critical to comprehend Iraqi patients’ perceptions of the privacy and confidentiality of EHR systems.
The Study’s Aim and Objectives
The purpose of this research is to determine how patients in Iraq feel about and trust EHRs. The study also looks into how open Iraqi patients are to sharing their medical and personal data with doctors and hospitals.
Methods
Study Design and Sample Size
This cross-sectional study targeted adult Iraqi patients referred to and treated in Iraqi public and private healthcare facilities. As there is no accurate estimate of patients referring to healthcare facilities, the minimal sample of 377 participants was considered needed for this study; the sample size was calculated using the Raosoft software sample size calculator. 25 The sample size was calculated based on a 50% expected frequency and a 5% confidence limit. This minimal sample would give adequate power for bivariate, multivariable analysis to be carried out. Estimating a dropout factor of 30% (the possibility that some approached pharmacists will decline to participate in the study or drop out during it), a minimum sample of 550 patients will be targeted and approached.
Eligible Participants’ Identification and Recruitment
The research team approached eligible participants directly in order to identify and recruit them. Participants who were approached were given a concise explanation of the study, its purpose and objectives, its procedures, and what was expected of them. Before approaching eligible participants, the necessary permissions and approvals were obtained from the management team. In addition, the research team identified and recruited potential participants through personal contacts and networking.
Survey Design
The study’s goal and objectives informed the creation of a questionnaire that surveyed Iraqi patients’ attitudes and confidence in EHRs. Six professionals in the fields of health service management, digital marketing, cyber security, and information systems reviewed the initial survey version. The reviewers were tasked with assessing the reliability and construct and face validity of the survey. In response to the feedback and suggestions of the reviewers, the questionnaire has been revised and improved. The modified questionnaire was then piloted on a sample of 62 people who were selected because they were similar to the study’s target population. The purpose of the trial run was to test the legibility and comprehension of the final survey. At last, the evaluation from the pilot was taken into account, and any changes that were required were made.
There are a total of 13 questions spread across 3 sections in the final survey instrument. The first portion focuses on the demographics and personalities of the participants. Second, participants’ medical histories; third, participants’ confidence in and openness to the healthcare information system and their own individual health records. In the final portion, respondents rated how trustworthy they felt the experiment was on a Likert scale.
Data Collection Tool and Study Instrument
The research team used a face-to-face researcher-administered method to assure the eligibility of the targeted participants and achieve a high response rate. In addition, this format allowed participants to clarify ambiguous or unclear queries and responses.
After ethical approval, survey design, and validation, the research team requested permission from the Iraqi Ministry of Health and healthcare facilities in the targeted governorates to use their facilities as recruitment sites. Adult Iraqi patients referring to private and public healthcare facilities in targeted governorates will be directly approached and recruited by research assistants who have been adequately trained to collect data and respond to any questions from the approached participants.
In total, 900 eligible individuals were invited to participate in this investigation between April and June 2022. Eligible individuals were given a participant information sheet and a consent form. Consenting participants were given a copy of the survey, which requires 10 to 15 min to complete.
Statistical Analysis
After data collection, data logging, cleaning, coding and grouping were completed using an Excel® workbook (Microsoft Office MS, 2013).
Descriptive analysis in the form of frequencies, percentages and standard deviation, when applicable, was carried out. Z-test was considered to compare male and female participants. Moreover, logistic regression was used to determine factors associated with participants’ trust in EHRs. Influencing factors were determined based on the study’s aim and objectives, and available literature. Data analysis was carried out using STATA® data analysis and statistical software (StataCorp, 2016).
Ethical Consideration
In April 2022, the Institutional Review Board-Scientific Research and Graduate Studies Deanship at Yarmouk University reviewed and approved this study (Ethic Identifier Number: RD/119/12).
Results
Participants’ Demographics and Characteristics
Out of the 900 approached individuals, 656 agreed to participate (the response rate was 72.9%). Out of the 656 participants, 552 provided completed survey forms that were considered for analysis. The study sample fairly represented the Iraqi population, with almost 50% of the participants being females, a ratio equal to the official sex ratio of Iraq. 26 In addition, one-third of the participants were between 29 and 39 years old, and almost 60% held a university degree. Table 1 summarizes participants’ demographics and characteristics.
Participants’ Demographics and Characteristics.

Note. EHR = Electronic Healthcare Record; N = number.
There is a statistically significant difference between the 2 groups (P-value < .05).
Medical History
While most of the study respondents perceived themselves to have good health, 84.1% declared being diagnosed and treated for at least 1 chronic disease, mainly diabetes and hypertension. In addition, results showed that a significantly higher percentage of female respondents (44%) reported having a good health status than male respondents (30.7%) (P-value = .001). In terms of the healthcare sector, more than 70% received healthcare services at private sector facilities and providers. Additionally, approximately one-third of the respondents used healthcare services 3 to 5 times in the last 6 months. Table 1 summarizes the study participants’ medical history.
Perceptions and Trust Toward EHRs
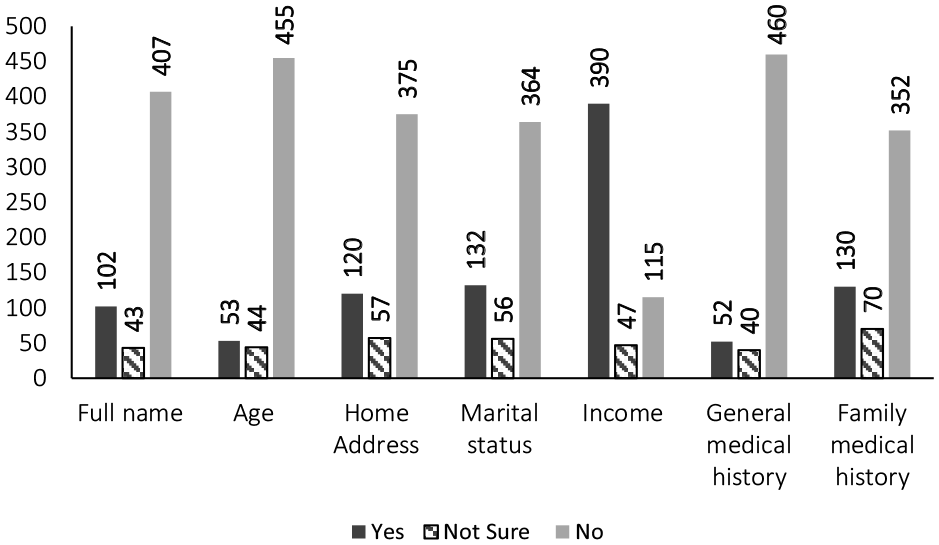
Results showed that the vast majority of the respondents were familiar with the concept of EHRs, and trusted these records as data collection and storage systems. Furthermore, almost 50% of the research participants reported media platforms, whether traditional or social media, as their source of information regarding EHRs. On the other hand, only 58 (10%) of the respondents preferred not to have their EHRs exchanged among healthcare professionals and institutions. Moreover, while 253 (45.8%) of the study respondents agreed to share their complete records with physicians and nurses, only 124 (22.5%) trusted pharmaceutical companies enough to share their completed records. Interestingly, despite being known as a conservative society, female respondents were significantly more willing to share their full names with healthcare professionals than male respondents. Finally, only 20 (3.6%) participants were comfortable sharing all their personal information with healthcare professionals. Table 2 and Figure 1 summarize perceptions and trust toward EHRs.
Participants’ Perceived Rusts in EHRs and Willingness to Share Information and Data.

Note. EHR = Electronic Healthcare Record; HCP = Healthcare Professional; N = number.
Total number of participants is 552, out of which 275 were females, and 277 were males.
Out of those who are familiar with electronic healthcare records.
Respondents were allowed to choose more than 1 answer.
Participants’ willingness to share personal information and details.
Predictors of Trusting EHRs
Predictors that could influence participants’ trust in EHRs were identified and investigated based on the study’s aim and objectives, available literature and collected data. The influence of gender and familiarity with EHRs and the healthcare sector (private or public) was assessed. Ordered logistic regression showed no significant associations between all investigated factors and participants’ trust in EHRs. Table 3 shows the output of the ordered logistic regression.
Ordered Logistic Regression Outputs of Trusting EHRs.

Note. CI = confidence interval; Co = coefficient; N = number; P = probability value; SE = standard error.
Discussion
This study assessed Iraqi patients’ trust in EHRs and willingness to share personal and medical information with healthcare professionals. The research team captured the perception and the feedback from 552 participants referring to private and public healthcare facilities and providers in Iraq. Participants’ perceptions were captured using a validated questionnaire instrument. The instrument included items related to participants’ demographic and characteristics, medical history, trust in the healthcare information system and willingness to share personal and medical data.
Eligible participants, Iraqi patients referring to private and public healthcare facilities, were identified and recruited using venue-based sampling. Agreeing participants were interviewed using the face-to-face researcher-administered mode of data collection. These 2 strategies had increased response rate, limited cases of missing data, and allowed the respondents to ask for clarifications. This was evident in securing a high response rate (72.9%) of the approached eligible participant and the absence of missing data and incomplete surveys. Nevertheless, the followed sampling technique limited the possibility of achieving a diverse sample. This was apparent as the majority of the participants were suffering from chronic diseases.
The recent integration of EHRs in Iraqi healthcare facilities, and the alarming rates of digital illiteracy among the Iraqi population, especially among women and youth,27,28 might suggest that only a minority would be familiar with EHRs. However, results showed that more than 70% of the study participants were aware of EHRs. The relatively high percentage of awareness could be attributed to the fact that more than 70% of the participants were younger than 50 years old and might have been exposed to records and database management systems such as social media platforms, banking systems and other governmental electronic systems. Additionally, the majority of the participants are reported to be treated for chronic diseases. Patients with chronic diseases are, in general, heavy users of healthcare services and frequent visitors to healthcare facilities. Therefore, these patients are more likely to be familiar with EHRs or share their data with healthcare professionals and administrators. Lastly, as the questionnaire instrument only assessed participants’ familiarity with the term EHRs, it was not possible to assess if the participants’ truly understood EHRs functionalities, operations, related procedures and potential privacy and security threats.
Patients’ control over medical records, including EHRs, is manifested by 3 dimensions: the nature of shared data, data management, and the healthcare ecosystem (Figure 2). In addition to investigating familiarity, the current study explored the participants’ perceptions toward the type of shared data, willingness to grant access to healthcare professionals and acceptance to share and exchange EHRs among healthcare professionals and healthcare facilities.

Patients control over medical records.
In different public service areas, integrating information technology in service delivery has facilitated the interaction between service providers and users. 29 In healthcare services, E-systems, including EHRs, have been proven to improve healthcare quality and achieve patient satisfaction.10,11 Smooth and efficient integration of E-systems depends on several factors, including system quality, service quality, net benefit and trust. 30 Trust refers to the extent to which the end-users perceive the trustworthiness of E-systems and their management. 31 Previous studies indicated trust is integral to end-users overall satisfaction with E-systems. 31
Despite the frequently reported concerns regarding the security, integrity and privacy of EHRs, especially by healthcare professionals and patients in developing countries,32 -34 the current study showed that the majority of the surveyed participants generally trusted EHRs. However, only 29 of the trusting participants were willing to share personal identifiers; full name, address and age. The reluctance and hesitance toward sharing personal identifiers and data are consistent with the conservative nature of Iraqi society, a Middle Eastern society.
The EHR systems are well recognized for their role in improving the quality of provided service and minimizing operational costs.10,11 Healthcare services’ quality depends on the availability of timely, complete and accurate medical records, including personal and sociographical data. 35 Therefore, EHRs should be as complete and as comprehensive as possible. Consequently, the incompleteness of medical records could jeopardize patients’ health and hinder healthcare professionals from delivering patient-centered care.
Information technology and applications, including those used in the healthcare ecosystem, are vulnerable to cyber-security challenges such as attacks and illegal and unethical practices.34,36 Available literature highlights patients’ and healthcare professionals’ concerns regarding EHRs’ overall security, including personnel’s privacy and data confidentiality. 13 Moreover, as patients become more familiar with EHRs, they demand a more active role in managing and controlling their records.37,38 Patients want to know who has access to their data, for what reason, when and where.37 -39
The Healthcare ecosystem comprises a network of healthcare providers collaborating in delivering healthcare services. As a system, it includes hospitals, care centers, clinics, healthcare professionals and other healthcare organizations and facilities. 40 Sharing and exchanging medical records, including EHRs, between healthcare professionals and organizations is a privacy and security threat.41,42 This study explored the participants’ attitudes toward EHRs sharing within the Iraqi healthcare ecosystem.
Similar to Hoerbst et al study, most participants supported the notion of sharing and exchanging their EHRs and related data between healthcare professionals and organizations. 39 Moreover, results showed that most research participants were willing to share and grant full access to their medical and personal data to physicians, medical doctors. On the other hand, only a shy majority were willing to share their data with other healthcare professionals, such as nurses and pharmacists. Medical staff’s incompliance with ethical and legal standards when handling medical records, including EHRs, is a commonly reported challenge. In their review, Ghazvini and Shukur argued that human error and illegal behaviors are among the major threats to the privacy and security of EHRs. 43 Patients’ willingness to share their medical and personal data with healthcare professionals might reflect what extent they trust healthcare professionals. 44 Moreover, the completeness and comprehensiveness of medical records depend on the dynamics between patients and healthcare professionals. The significant difference among healthcare professionals might indicate that Iraqi patients trust medical doctors more than other healthcare professionals.
To the authors’ knowledge, this is the first study to explore Iraqi patients’ perceptions and trust toward EHRs. The general impression indicated that work still needs to be done to investigate the Iraqi population’s perceptions toward the privacy and security of EHRs.
Conclusion
Integrating EHRs into the healthcare ecosystem would be greatly aided by patients who are willing, cooperative, and trusting. Patients, medical staff, and organizational framework all play crucial roles in realizing EHRs’ full potential for increasing healthcare quality, boosting efficiency, and cutting costs.
In addition, legislators and regulators may need to take steps to boost patients’ confidence in EHRs and enhance their interactions with non-medical healthcare staff.
Footnotes
Acknowledgements
The research team would like to thank all the study participants for their participation and support of this study.
Author Contributions
Saja Alnahar: Survey & study design, Acquisition of data, interpretation of data, drafting original and final submission, preparing figures and tables. Mahmoud Alkailani: Survey & study design, Acquisition of data, interpretation of data, drafting original and final submission. Ammar Abdulhasan: Survey & study design, collected data and carried out the analysis. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was conducted to fulfill a master’s degree that Al Qadisiyah University-Iraq sponsored.
Ethical Consideration
In April 2022, the Institutional Review Board-Scientific Research and Graduate Studies Deanship at Yarmouk University reviewed and approved this study (Ethic Identifier Number: RD/119/12).