
Abstract
Nigeria is one of the developing countries with a major burden of non-communicable diseases (NCDs) without a disease self-management program in its healthcare system. Thus, this study was aimed to assess the baseline self-efficacy levels of Nigerian patients with chronic NCDs at tertiary level hospitals. This is a cross sectional study of 286 NCD patients attending tertiary level clinics from 26 July to 27 October 2023. Patients were interviewed on a 10 Self-Efficacy to Manage Chronic Disease (SEMCD) item scales that were considered suitable for the Nigerian population. The 10 SEMCD questions covered: (i) Exercise regularly scale, (ii) Help from community, family and friends scale, (iii) Communication with Physician scale, (iv) Manage disease scale and (v) Manage symptom self-efficacy domains. Data were analyzed both descriptively and statistically using Student’s t-tests and Chi-square tests as appropriate. The results showed that more female (59.4%) than males (40.6%) attended clinics during the study, and the mean age of the patients did not differ between gender (P > .05). About 40% of all the patients manage their NCDs with medications alone, a trend that is similar in male and female patients (P > .05). While all the patients had a relatively lower self-efficacy scores under regular exercise scale (52%-55%) and manage disease symptoms scale (53%-55%), they tended toward higher self-efficacy scores under getting assistance from community, family, and friends (79%-80%) and communication with attending physicians (81%-85%). It is concluded that Nigeria literate NCD patients registered at tertiary level institution routine clinics are less than optimal in disease self-management care. We recommend that this study population will benefit from introduction and implementation of disease self-management program in the healthcare system.
Keywords
Patients with multi-morbidity who demonstrated higher self-efficacy levels had high health-related quality of life than patients with lower self-efficacy scores.
This study contributed to this field from a population with a high prevalence of chronic non-communicable diseases yet with little knowledge of disease self-management.
The implications included but not limited to introduction of structured disease self-management education and making the same healthcare policy in all healthcare institutions in developing countries.
Introduction
Diabetes mellitus, cardiovascular diseases (heart disease and stroke), chronic kidney disease (CKD), cancer, and chronic respiratory diseases are non-communicable diseases (NCDs) that are of major public health concerns, and they account for about 3 quarters of all deaths in developed and developing countries. 1 Of the 17 million people who die of NCDs at age below 70 years every year, 86% of them are residents of low- and middle-income countries. 1 Nigeria is one of the countries with a great burden of NCDs in addition to communicable diseases. For example, of 2.12 million total deaths in Nigeria in 2016, 29% (617,300) was due to premature mortality from NCDs. 2 Of greater concern is that health-related expenditures in Nigeria is usually out of pocket expenses because of the absence of universal health insurance coverage. This might have indirectly contributed to the extreme poverty in Nigeria population as chronic illnesses tend to go hand in hand with poverty. 3 Indeed, a study in southwestern Nigeria have shown that NCD-related out of pocket health expenditures contributed to impoverishing the patients. 4
It is also important to note that there is significant disparities in the incidence, progression and complications between patients in industrialized and in developing countries. 5 These disparities are related to lower socioeconomic and educational status of the patients in developing countries. 5 For example, 80% of patients with diabetes reside in low- and middle-income countries, and morbidity and mortality arising from NCD are greater in developing countries. 6 Thus, it is widely accepted that NCDs require chronic self-management care, skills, and education on the part of the patients and the healthcare professionals to prevent complications that will lead to morbidity or mortality.7,8 In Nigeria, like other developing countries, there are no disease self-management programs and service frameworks to prevent NCD progression to morbidity and mortality.7,9 In contrast, many developed countries have institutionalized self-management program in their health care systems with the resultant effect of reduced mortality or morbidity from NCD complications.7 -10 We are of the view that the best approach toward stemming the tide of NCD-related morbidity and mortality in Nigeria and other developing countries would be increased efforts toward developing disease self-management programs with service framework that would progressively educate the patient population on activities and lifestyle behaviors that would assist in reducing the burden of frequent patients’ visits to the clinics/hospital, reduce excess medical expenses, and prevent disease progression to morbidity and mortality. 9 In this regard, this study was aimed to establish the baseline self-efficacy levels of the NCD patients registered at tertiary level routine clinics in Southeastern Nigeria. Southeastern Nigeria was chosen because it is a predominantly homogeneous ethnic group of Igbos with Igbo common language, common dietary pattern, and similar lifestyles. It is envisaged that the result from this study will provide information on baseline disease self-management strategies of the patients in southeastern region of Nigeria.
Design and Methods
Selection of Study Sites
This is a cross sectional structured interview-based study of 286 NCD patients on routine doctors’ appointment visits at 4 tertiary hospitals from 26 July to 27 October 2023 (3 months). To establish the baseline self-efficacy levels of the patients on different disease self-management activities, we selected four (4) tertiary hospitals in Anambra State, of south-eastern Nigeria. These hospitals were selected based on the high number of NCD patients registered at the clinics, existence of specialized NCD clinics, full compliments of specialist doctors, nurses and nutritionists. These criteria were necessary to ensure that the patients had received at least a minimal NCD health education to warrant assessment of disease self-management strategies. In addition to our teaching hospital, the following hospitals qualified based on the established inclusion criteria: -
(i) Chukwuemeka Odimegwu Ojukwu University Teaching Hospital, Awka
(ii) St Joseph Hospital Adazi-Nnukwu, and
(iii) St Charles Borromeo Specialist Hospital, Onitsha
These hospitals have specialized clinic days for different NCD patients, and the patients were interviewed only on their routine clinic appointment days. To avoid interviewing a patient twice, they were advised not to consent to any further interviews should they visit their doctors again before the end of October 2023. The study proposal was reviewed by our institutional research Ethics Committee (Ref. NAUTH/CS/66/VOL16/VER.3/168/2023/053) and subsequently institutional approvals were received from all the hospitals to conduct the interviews in their hospital facilities and NCD patients.
Selection of Study Questionnaire Tool
The “free to use without permission” Self-Efficacy to Manage Chronic Disease (SEMCD) original 33-item scale was sourced and downloaded from the website of Self-Management Resource Centre (SMRC). 8 We selected ten (10) questions from the Self-Efficacy to Manage Chronic Disease (SEMCD) original 33-item scale that were considered suitable for the Nigerian population. The 10 SEMCD questions selected covered the following self-efficacy domains: Exercise regularly scale, Help from community, family, friends scale, Communicate with Physician scale, Manage disease scale and Manage symptom scale.
All the questions were rated on a scale of Score 1 (not at all confident) to Score 10 (totally confident) as originally designed and validated. 9 The questionnaires were not validated locally because they were previously used and validated by other workers. 9 This is a pilot exploratory study which would serve as a baseline template for our phase 2 metabolic study on the same patients. We adopted patient-interviewer approach in administering the questionnaires because the recorded average literacy level in Nigeria in 2018 was about 62%. 11 Thus, to harmonize the administration of the questions, the 10-item questions were translated into central Igbo language. Central Igbo language is the commonly spoken accent used in Anambra State and it is homogeneous. The interviewers (CN, RA, AA, PO and B0) met about 5 times, read, and agreed that the translated versions of the original questions were the literarily and technically correct translation of the question as contained in SMRC (Self-Management Resource Centre Table 1). A rehearsal was conducted several times amongst the interviewers to harmonize on the strategy for asking the questions and eliciting the correct responses using the translated Igbo language version. A pictorial aid for the Score Scale (1-10) was also internally developed to assist the least educated patients in identifying the point on the scale at which they have confidence in performing specific tasks asked in the questionnaire (Figure 1).
English and Igbo Language Versions of Chronic Disease Self-Efficacy Questionnaire.


A pictorial aid of the CDSE score scale.
Study Protocol
The study team was given a space or private rooms in each of the tertiary hospitals for the conduct of the research interviews. None of the patients had prior contact with any member of the research team and had no prior educational training from our research group except whatever NCD education they received from their healthcare providers during their routine clinic visit. To seek the patient’s verbal consent on each study day, the patients were approached on individual’s basis and the general aim and objectives of the study (written as explanatory letter for ethical approval) were thoroughly explained to them in Igbo language and their voluntary consent solicited. Although the study was conducted only on specialized routine clinics days, patients were only qualified to participate in the study if they were previously diagnosed and registered as a patient with diabetes, hypertension, heart disease, kidney disease or any complication thereof. Those who gave their voluntary consent to participate in the study were taken to the allocated study room for the interview. Thus, the questionnaires were administered in absolute confidentiality in the private rooms/spaces provided. Patients who had difficulty with the SEMCD score scales were asked to indicate their confidence levels using the pictorial aid. Overall, it was reported that only 2 patients utilized the services of the pictorial aid. Indeed, most of the patients had no difficulty in understanding the questions asked in Igbo language. Thus, there were no reports of any linguistic challenges at any of the hospital study sites. After the interview, the patients were informed that the data collected might be published in a medical journal for the purpose of helping to improve medical services. The were informed that their identities would be preserved. No patient objected to potential publication of their responses to the research questions.
Data Analysis
The Statistical Package for the Social Sciences (SPSS, version 27) was used to analyze the quantitative and qualitative variables both descriptively and statistically. Then the student’s t-test was employed to analyze the self-efficacy scores (quantitative variables) between male and female patients while Chi-square was utilized (where needed) to analyze all categorical variables. All quantitative data are presented as mean ± standard deviation (SD) while all qualitative data are presented as numbers and percentages. A P-value less than .05 was considered as statistically significant at 2-tailed testing.
Results
The quantitative data are presented as mean ± SD while the qualitative data are presented as numbers and percentages. Table 2 shows the distribution of the different NCDs in the study hospital sites. Hypertension (43%) constituted the highest number of single NCD patients interviewed while about 31% of the patients interviewed had both hypertension and diabetes. Patients living with only diabetes were 44 (15%). Table 3 shows the sociodemographic characteristics of all, and the male and female patients interviewed. More females (59.4%) than males (40.6%) were on routine clinic visits during the study, and the mean age of the male and female patients did not differ (Table 3). Overall, about 38.5% of all the patients have had NCDs in the last five (5) years while 28.3% had lived with NCDs for more than 10 years, and the trend was similar in both male and female patients. Of all the 286 patients interviewed, only 3 female patients (1.0%) had no formal western education while 35.3% of all the patients had tertiary level education. Almost 50% of the patients interviewed were employed, 14.3% were not employed and 36% were retired. About 40.2% of all the patients interviewed indicated that they manage their NCDs with only medication, 34.3% with medication and diet alone and 18.9% manage their NCD with medication, diet, and exercise (Table 3). These management strategies are similar in male and female patients. Table 4 shows the baseline self-efficacy scores of all the NCD patients, and male and female patients. The mean self-efficacy scores of all the patients were relatively low under the themes of regular exercise scale (5.2 ± 3.0 and 5.5 ± 2.9: ~52% to 55%) and manage symptoms scale (5.3 ± 2.7 and 5.5 ± 2.7: ~53% to 55%, Table 4). These self-efficacy scores were similar in male and female patients (P > .05, Table 4). However, the female patient tends to have higher mean self-efficacy score than the male patients under manage disease scale (6.6 ± 2.2 vs 6.1 ± 2.5, P = .06, ~66% vs. 61%). Overall, all the patients tend to have the highest mean self-efficacy scores under the themes of “help from community, family and friends scale” (7.9 ± 2.4 and 8.0 ± 2.3, ~79% to 80%) and “communicate with physician scale” (8.5 ± 1.6 and 8.1 ± 2.2: ~81% to 85%, P > .05, Table 4).
Descriptive Analysis of the Numbers (%) of NCD Patients Interviewed at the 4 Hospital Study Sites.
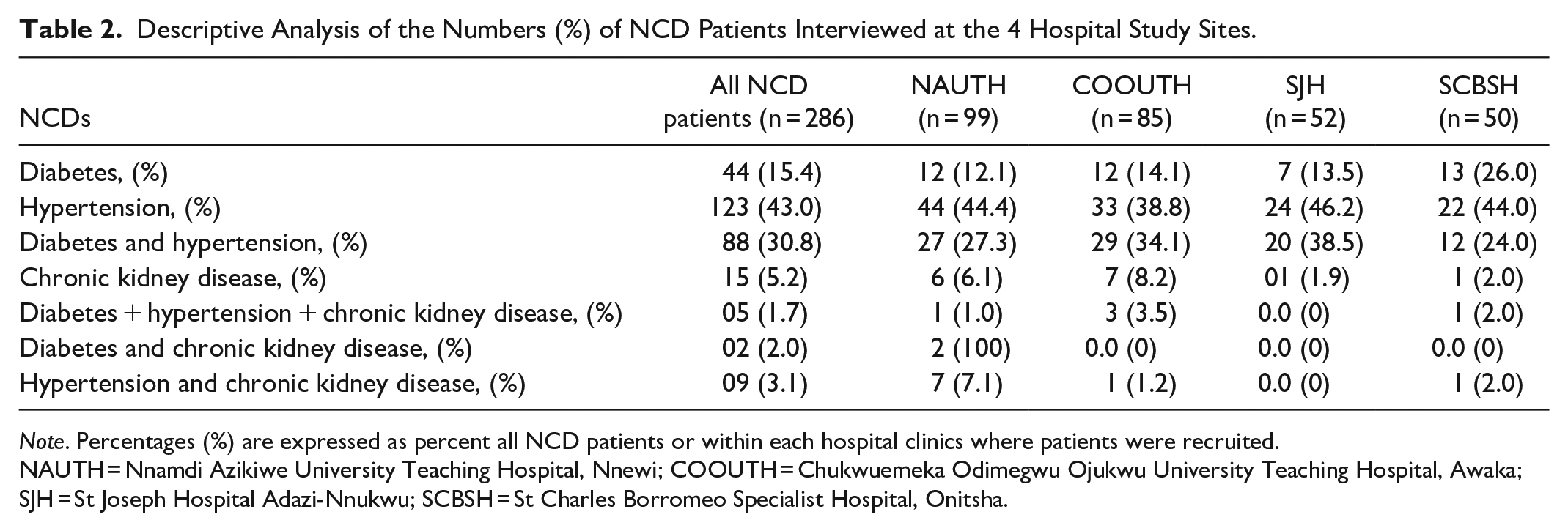
Note. Percentages (%) are expressed as percent all NCD patients or within each hospital clinics where patients were recruited.
NAUTH = Nnamdi Azikiwe University Teaching Hospital, Nnewi; COOUTH = Chukwuemeka Odimegwu Ojukwu University Teaching Hospital, Awaka; SJH = St Joseph Hospital Adazi-Nnukwu; SCBSH = St Charles Borromeo Specialist Hospital, Onitsha.
Gender-Related Comparisons in Age, Disease Duration, Disease Management Strategies, Employment, and Educational Status of the Patients.
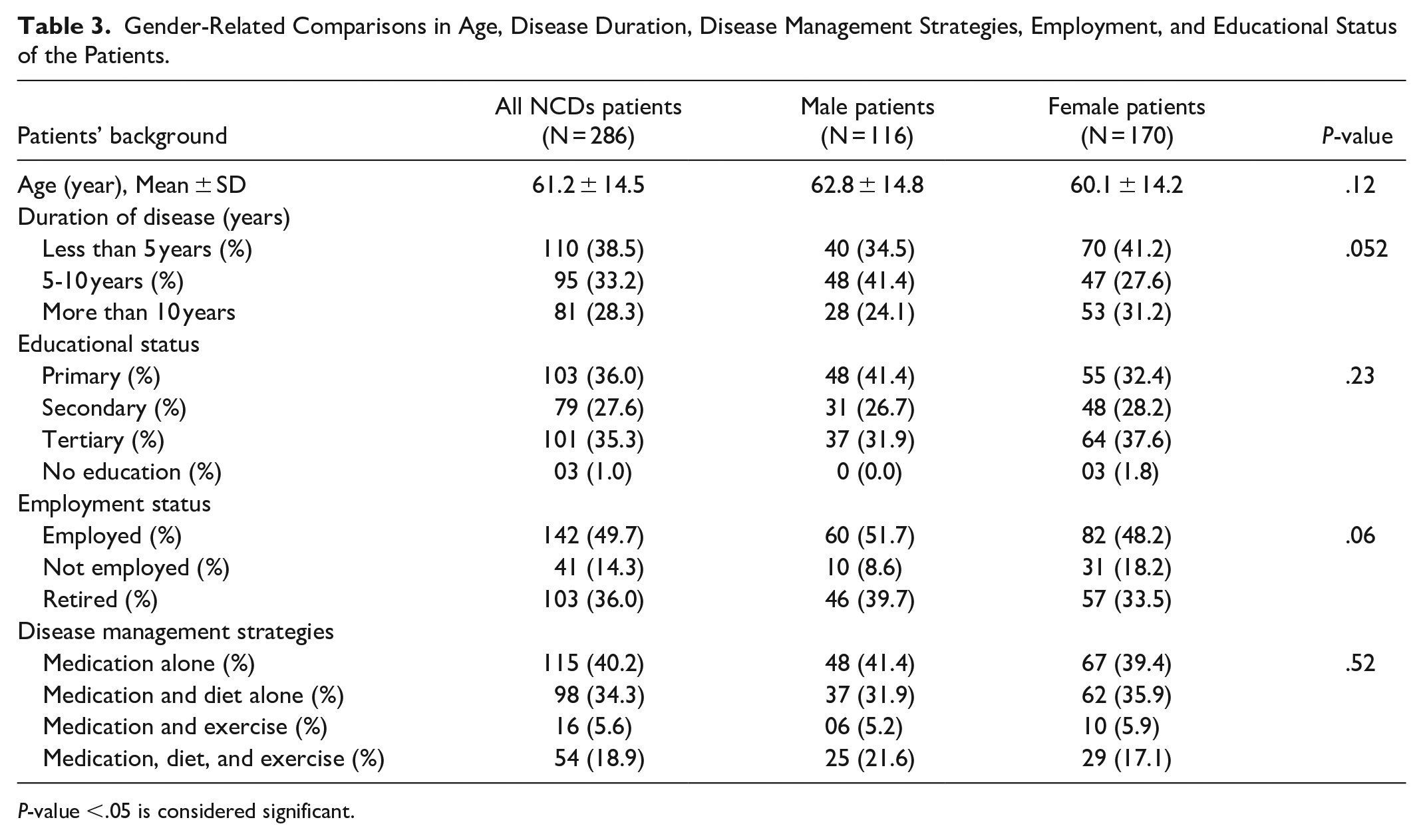
P-value <.05 is considered significant.
Baseline Self-Efficacy Scores [1-10] for All, and Between Male and Female Patients.

P-value <.05 is considered significant.
Discussion
The analysis of the data from this study, which assessed the baseline self-efficacy scores of 286 NCD patients at 4 tertiary hospitals in Southeastern Nigeria, showed that more females than male NCD patients were seen in the 4 tertiary hospital clinics during the 3-months study period. About 40% of all the patients interviewed manage their NCDs with medications alone. The patients had a relatively low mean self-efficacy scores under regular exercise scales (52%-55%) and management of disease symptoms scales (53%-55%), and
Gender-biased Routine Clinic Visits: Female Versus Male NCD Patients
The finding of higher number of female NCD patients in this cross-sectional study might reflect the general healthcare uptake in this population. It is possible that women have higher prevalence of NCDs in this region of Nigeria or that women living with NCDs are more compliant with clinic appointments than their male counterparts. A Center for Disease Control series report in the United States showed that non-pregnant women were 33% more likely than men to visit a doctor. 12 The report also indicated that most elderly women living with hypertension or diabetes were more likely to keep a specialist doctor appointment than their male counterparts. 12 Furthermore, a study of apparently healthy southwestern elderly Nigerians (aged > 55 year) showed that women residing in the urban areas were at a greater risk for cardiovascular diseases than men particularly because of overweight/obesity and sedentary. 13 Thus, this high number of female NCD patients in this study appears consistent with the vulnerability of women to NCDs. 14 Non-communicable diseases have been identified, globally, as the leading cause of two-thirds of death among women annually. 14 It should, however, be noted that the risk factors for NCDs are similar for men and women, but at times women health-related issues are misinterpreted or neglected. 15 Therefore, going forward, it may be important to recognize the peculiarities of the female gender when designing disease self-management program given the NCD-related high mortality in women in low- and middle-income countries. 14 It is however encouraging to observe that the female patients appeared to have higher confidence to do other things than just taking medications to reduce how much the illness affected their everyday lives (61% vs 66%, P = .06). Perhaps, female patients might be more disposed to disease self-management program than their male counterparts.
Poor NCD Management Strategy: 40% Manage With Only Medications
The finding that about 40% of the NCD patients interviewed indicated that they manage their diseases with only medications is a major source of concerns for this study population. The 4 tertiary hospitals chosen for this study have specialized clinics during which the patients were given basic health education specific to their ailments. It is rather surprising that about 40% of the 286 respondents were not utilizing a combination of medication, exercise and diet in the management of their illnesses. This is less surprising given that the patients’ mean self-efficacy scores were comparatively lower, albeit insignificant, under the themes of regular exercise scale and management of disease symptoms (P > .05, Table 4). It is widely accepted that the best approach to stemming the tide of increased morbidity and mortality from NCDs is through disease self-management program.7,9,10 We witnessed evidence of minimal health education sessions during clinics at the tertiary hospitals, but Nigeria, like most other developing countries, have not developed nor integrated disease self-management program into the healthcare systems as seen in other countries.7,9,10 We are strongly of the opinion that the development of disease self-management programs for this population might assist in improving the number of NCD patients that would utilize non-pharmacological strategies in the management of their NCDs. Indeed, that is the focus of our ongoing joint research project in Nigeria.
Low Baseline Self-Efficacy Scores: Regular Exercise and Disease Symptoms Management
The observed relative low mean self-efficacy scores under regular exercise scale and management of disease symptoms scale are rather surprising given the health education sessions we witnessed at the clinics during the study. It is most likely that the health education sessions did not include the principles of disease self-management. The basic principle of disease self-management is that the patient is the primary manager of his/her chronic disease while the healthcare provider is the coach or guardian; both working in partnership to develop the best strategies for managing the chronic disease.7,9,10,16 It is possible that the healthcare educators at the clinics were not engaging the patients on disease self-management principles and thus created a gap in the appropriate health education with clinical goals during teaching session. Indeed, some other workers have queried the contents and principles of health education impacted on the NCD patients during clinics visits. 17 It should be noted, however, that increased regular exercise is one of the beneficial lifestyle behaviors that is difficult for patients to comply with especially in Nigeria urban cities without walkways for physical exercise like walking or jogging. 18 That notwithstanding, we suggest that since increased physical activity assists in managing chronic diseases, the provision of infrastructural facilities such as walkways, exercise centers and open green savannas are likely to facilitate proper management of NCD patients in this population. 19
High Mean Self-efficacy Scores: Influence of Community and Friendly Doctors
The finding that the patients had high mean self-efficacy scores in getting assistance from family, community and friends is a true reflection of African extended family system and community way of life in villages and cities. 20 In Africa, and indeed in Nigeria, friends and relations consider anyone’s burden as a community burden, and individuals readily assist each other in times of difficulties. This is enshrined in African hospitality concept specially practised in Igbo ethnic group. 20 Of greater significance from this study is the observation that the patients had high mean self-efficacy scores under the theme to communicate openly with the physicians and readiness to ask the physicians open questions related to their illness. The patients’ indication of high confidence in doctor-patient interaction or relationships seen in this study is very interesting and would be beneficial in designing Nigeria disease self-management program. NCD patients are the primary managers in disease self-management program. 16 Given that patients are usually given insufficient time during routine clinic visits, patients with high confidence and motivation to speak openly with the healthcare team about their illness are much more likely to achieve the desired clinical goals. 21
Study Limitations and Conclusions
There are a few limitations to this study. The study was designed as consecutive cross sectional exploratory pilot study to determine the baseline self-efficacy levels of NCD patients that would be involved in the next metabolic study. Thus, sample size and power analysis was not performed for this pilot stage. Additionally, we did not validate the questionnaire tool used in the study given that the selected questions have been validated and used by other authors.9,10 These 2 limitations notwithstanding, this study showed that hypertension (43%), diabetes (31%), and chronic kidney disease (5.2%) are the common NCDs in these clinics and more females than males appeared affected. Although the majority of the patients are literate and reside in cities, 40% manage their NCDs with only medications and 52% to 55% expressed low confidence to manage their NCD with exercise. These observations taken together; we conclude that these tertiary level NCD patients studied are less than optimal in disease self-management care. We recommend that this study population will benefit from introduction and implementation of disease self-management program in the healthcare system.
Supplemental Material
sj-doc-1-inq-10.1177_00469580241248102 – Supplemental material for The Baseline Self-Efficacy Scores to Manage Chronic Diseases Amongst Nigerian Patients with Non-Communicable Diseases are Sub-Optimal
Supplemental material, sj-doc-1-inq-10.1177_00469580241248102 for The Baseline Self-Efficacy Scores to Manage Chronic Diseases Amongst Nigerian Patients with Non-Communicable Diseases are Sub-Optimal by Chidum E. Ezenwaka, Clementina U. Nwankwo, Rosemary A. Analike, Michiko Moriyama, Anulika J. Afonne, Perpetua C. Ottiwu, Blessing T. Onyeje, Justina N. Okoli, Ifeoma A. Amaechi and Gladys I. Ahaneku in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-2-inq-10.1177_00469580241248102 – Supplemental material for The Baseline Self-Efficacy Scores to Manage Chronic Diseases Amongst Nigerian Patients with Non-Communicable Diseases are Sub-Optimal
Supplemental material, sj-pdf-2-inq-10.1177_00469580241248102 for The Baseline Self-Efficacy Scores to Manage Chronic Diseases Amongst Nigerian Patients with Non-Communicable Diseases are Sub-Optimal by Chidum E. Ezenwaka, Clementina U. Nwankwo, Rosemary A. Analike, Michiko Moriyama, Anulika J. Afonne, Perpetua C. Ottiwu, Blessing T. Onyeje, Justina N. Okoli, Ifeoma A. Amaechi and Gladys I. Ahaneku in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We are grateful for the assistance and cooperation of the Nursing Staff of Nnamdi Azikiwe University Teaching Hospital, Nnewi, Chukwuemeka Odimegwu Ojukwu University Teaching Hospital, Awka, St Joseph Hospital Adazi-Nnukwu, and St Charles Borromeo Specialist Hospital, Onitsha. We thank the administration of the 4 institutions for the permission to use their hospital facilities and patients for the study.
Author Contributions
Chidum E. Ezenwaka: conceptualized the research idea, drafted the proposal, analysis of data, data interpretation, drafted the manuscript, submission of manuscript, and revision of the manuscript.
Clementina U. Nwankwo: refined the research idea, edited the proposal, field data collection, data interpretation, editing the manuscript and revision of the manuscript.
Rosemary A. Analike: refined the research idea, edited the proposal, field data collection, data interpretation, editing the manuscript and revision of the manuscript.
Michiko Moriyama: refined the research idea, edited the proposal, data interpretation, editing the manuscript and revision of the manuscript.
Anulika J. Afonne: refined the research idea, edited the proposal, field data collection, data interpretation, editing the manuscript and revision of the manuscript.
Perpetua C. Ottiwu: refined the research idea, edited the proposal, field data collection, data interpretation, editing the manuscript and revision of the manuscript.
Blessing T. Onyeje: refined the research idea, edited the proposal, field data collection, data interpretation, editing the manuscript and revision of the manuscript.
Justina N. Okoli: refined the research idea, edited the proposal, field data collection, data interpretation and editing the manuscript.
Ifeoma A. Amaechi: refined the research idea, edited the proposal, field data collection, data interpretation, editing the manuscript.
Gladys I. Ahaneku: refined the research idea, edited the proposal, data interpretation, editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was partially supported with the Study and Travel Grant to Professor Chidum Ezenwaka from the University of the West Indies, St Augustine Campus, Trinidad and Tobago.
Ethical Statement
The study proposal was reviewed by the Research Ethics Committee of Nnamdi Azikiwe University Teaching Hospital, Nnewi, Anambra State, Nigeria (Ref. NAUTH/CS/66/VOL16/VER.3/168/2023/053).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.