
Abstract
Integration of medication-assisted treatment (MAT) for opioid use disorder in primary care settings is an emerging health care delivery model that supports increased access to specialized care but requires primary care provider engagement. Examining the characteristics of providers who provide this service is key to informing targeted recruitment. Using administrative and supplemental data collected during license renewal, this study aimed to identify the characteristics of primary care physicians and nurse practitioners (NPs) associated with greater odds of providing MAT in their practice. A retrospective observational study was conducted using a descriptive correlational design. The analysis included 5259 physicians and 3486 NPs who renewed their licenses electronically in 2021 and specialized in primary care or psychiatry. Chi-square and logistic regression analyses were conducted to identify the demographic and clinical characteristics of physicians and NPs associated with MAT participation in their practice. Physicians had a higher odds ratio (OR) of providing MAT if they were younger than 35 years (OR = 1.334; P = .0443), practiced in a federally qualified health center (OR = 3.101, P < .0001), and offered a sliding fee scale in their practice (OR = 2.046; P < .0001). Likewise, NPs had higher odds of providing MAT if they practiced in a public or community health center (OR = 3.866; P < .0001). The results of this study highlight the personal and professional characteristics of physicians and NPs associated with higher odds of providing MAT. These findings may have implications for the recruitment and sustainability of MAT integration in primary care.
Keywords
Current data on health care workforce participation in medication-assisted treatment is limited and not sufficient to support proactive planning within states.
It is the first state-level study to use licensing and supplemental workforce data to identify characteristics of primary care physicians and nurse practitioners associated with the likelihood of medication-assisted treatment participation.
Findings from this study can inform workforce strategies aimed at expanding medication-assisted treatment accessibility to underserved communities in Indiana and may have implications for analyses in other states.
Introduction
The shortage of behavioral health services in the United States is well documented, and contributing factors to this trend are numerous and varied.1,2 Limitations in psychiatric services are attributable to factors such as a small proportion of psychiatrists practicing full-time, a high rate of psychiatrists preparing to retire, and a stagnant number of psychiatric residencies. 1 A national survey conducted by the National Center for Rural Health Professions found that many rural hospitals report a lack of mental health services as limiting their ability to provide referrals in rural communities. 3 Relatedly, shortages among master’s-trained behavioral health professionals may be attributed to burnout, desire to practice in metropolitan areas, and aversions to treating severe mental disorders. 4 These factors highlight the need for effective solutions to address potential gaps in access to behavioral health treatment, especially for patients seeking treatment for opioid use disorder (OUD).
Trends in the prevalence of OUD and opioid-related deaths have seen an exponential increase in Indiana since before the beginning of the 21st century.5,6 These trends, coupled with a shortage of behavioral health professionals that is projected to continue through 2030, 7 have been the impetus for developing new health care delivery models that can expand the capacity of behavioral health services. Many states have aimed to address limited access to behavioral health services by expanding insurance coverage for behavioral health care, offering reimbursement and loan repayment incentives, increasing provider salaries, and expanding training programs.8,9 Since 2012, Indiana has focused on expanding behavioral health care accessibility by integrating OUD treatment services into the primary care setting. 10
The integration of medication-assisted treatment (MAT) for OUD in the primary care clinical setting is growing as a health care delivery model for increasing access to care.11,12 In combination with counseling and social services, MAT has proven to be effective in supporting sustained recovery from opioid addiction. 12 Recently, legislation was passed that allowed providers to begin prescribing opioid agonist medications in their practice without the need for a waiver, pending completion of the appropriate training. 13 These medications include buprenorphine, naltrexone, and methadone and are proven to aid in reducing the gratifying effects of opioids, reducing symptoms of withdrawal, and improving patient health outcomes after recovery.12,14-16 Despite these promising results, the successful integration of care can be hindered by providers’ attitudes and stigma associated with MAT for OUD, limited administrative support, and a lack of appropriate training.17-19 Even among psychiatrists there is hesitancy to prescribe MAT-related medications given the possibility of patient medication misuse and intensive government oversight. 20 Logistical concerns are likely to be even greater among primary care physicians (PCPs) as they consider how to integrate MAT into their practice and determine whether they have access to behavioral health care resources, such as professional counselors. 21
In response to the limited capacity of PCPs and psychiatrists prescribing MAT-related medications in their practice, 2016 legislation was passed—The Recovery Enhancement for Addiction Treatment Act—that allowed nurse practitioners (NPs) and physician assistants (PAs) to receive training and apply for waivers to prescribe buprenorphine. 22 Both NPs and PAs have significantly contributed to increasing access to MAT. 23 However, since NPs face fewer state-level scope-of-practice restrictions when prescribing buprenorphine, they stand to influence more long-term benefits for access to care for patients from this shift.22-24 Further examination of organizational and personal barriers to prescribing MAT is needed to inform recruitment of qualified prescribers and retain the current NP workforce. However, such examinations require accurate and timely health professions data to confidently determine workforce composition, practice needs, and opportunities for expansion.
Previous studies that have examined MAT-prescribing behavior among primary care providers used public data sources, such as those maintained by the Substance Abuse and Mental Health Services Administration, or study surveys.20,22-24 However, these sources are limited in their ability to describe the practice-based characteristics of providers involved in MAT, and in some cases, only qualitative data were collected. 21 A 2019 study by Jones and McCance-Katz examined the practice-based characteristics of providers prescribing MAT-related medications, however, interpretation of the study results was limited by the methods used and a low response rate to the study survey. 23 Such data limitations are prevalent in MAT-related research and restrict the ability to inform ongoing workforce development initiatives. Obtaining more accurate data through standardized and validated data collection strategies is crucial, but it is also important to understand the information that is needed to guide these workforce-related initiatives in the right direction.
Previous studies have demonstrated several personal and professional characteristics of providers that are associated with their practice choices, and more specifically their engagement in certain types of services. Age, setting, and personal beliefs among physicians have been associated with differences in patient care decisions and practice patterns. 25 This affect is likely a product of differences in experience levels, scientific advances that influence education programs, and cultural changes. 26 Trends in gender representation within certain medical specialties and patient care services have also been observed. 27 Beyond demographic characteristics, other studies have found a relationship between a provider’s specialty, the settings they practice in and corresponding geographic locations with their likelihood of engagement in certain safety net programs.28,29
Previous research findings serve as the basis for studying the relationship between provider characteristics and the prescribing of MAT-related medications. This study aims to identify the demographic and practice-based characteristics of PCPs, psychiatrists, and NPs associated with providing MAT in their practice.
Methods
Study Design and Data Collection
This observational study used a descriptive correlation design and secondary data analysis. Data used in this study analysis include licensure and supplemental data collected during the license renewal period for physicians and NPs. This study was approved as an exempt research study by the Indiana University Institution Review Board (Protocol # 1909917756).
Study data were obtained from the Indiana health professions database, which includes supplemental information collected from Indiana physicians and registered nurses (including advanced practice registered nurses) during the biennial license renewal process. In the state of Indiana, advanced practice registered nurses (APRNs) are required to have an active registered nurse license to engage in advanced practice. Supplemental information includes demographic characteristics, education and training, specialty, practice characteristics, services provided (including MAT services through prescription of buprenorphine, naltrexone, and methadone), and populations served.30,31 These data are collected under statutory authority by the state of Indiana and stored in the Indiana health professions database for the purpose of supporting state-level research and evaluation to inform related policy and planning.32,33 Licensees are notified that supplemental information will be used for research at the time of their renewal.
Deidentified supplemental information for Indiana physicians and registered nurses who renewed their Indiana licenses in the fall of 2021 was obtained from the Indiana health professions database in November 2021. While utilization of self-reported data has a potential for response bias, these study data were collected under statutory authority and licensees attest that the information is true and accurate.
Physicians and nurses who indicated they provide MAT services through prescription of buprenorphine, naltrexone, or methadone were identified as MAT prescribers.
Study Sample
In 2021, 7047 actively practicing physicians were identified as having an active license status, reported that they actively practiced in medicine, and had a specialty in family medicine/general practice, internal medicine (general), obstetrics and gynecology, or psychiatry (Figure 1). While primary care specialties typically include general pediatrics (n = 793), these physicians were excluded because none of them reported providing MAT services. Another 805 physicians who did not have a practice located in Indiana were excluded. Finally, 187 physicians were excluded because their data were missing values for age. Age was calculated using physicians’ date of birth and the date in which they completed their license renewal. Missing date of birth is likely attributable to data entry error at the time of initial licensure application as this is a field that is only provided through the initial licensure application process.
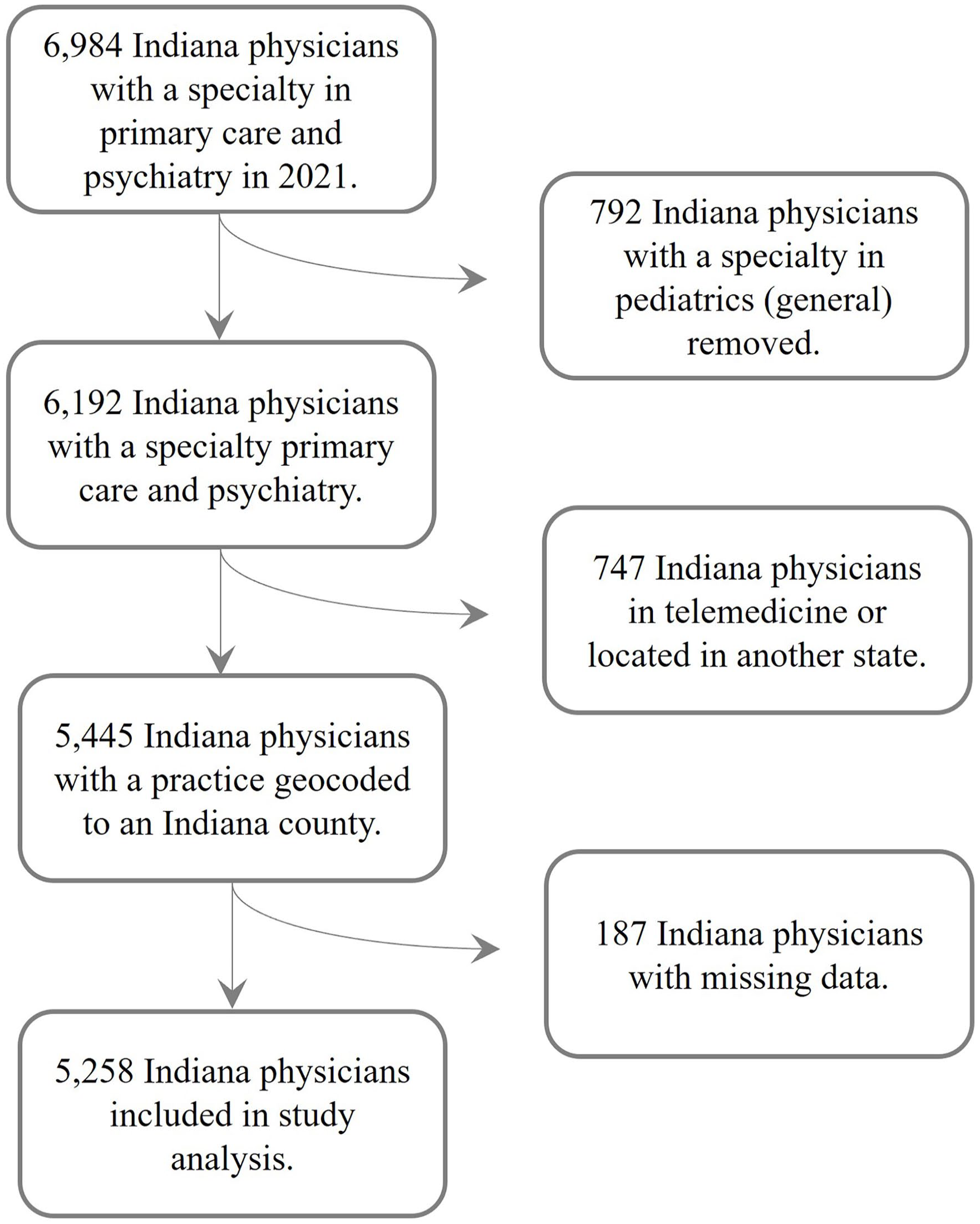
Selection criteria for physicians in study analysis.
APRNs were included in this study analysis if they identified as NPs and reported a specialty in primary care or psychiatry (Figure 2). In 2021, 4057 APRNs were identified as actively practicing and having a specialty in primary care or psychiatry. Of these, 3931 were identified as NPs based on their responses to the supplemental survey. Those who reported their practice setting as insurance claims/benefits or policy/planning/licensing agency or did not report a practice setting (n = 97) were excluded from this study as these setting types do not provide direct care to patients, including MAT treatment. Another 359 NPs who did not practice in Indiana were excluded. There were 4 NPs excluded due to missing values for date of birth.

Selection criteria for nurse practitioners in study analysis.
Study Variables
Physicians’ demographic variables included gender (male/female), race (White/Asian/Black or African American/other), and age group (less than 35/35-44/45-54/55-64/65 and older). Similar demographic variables were included for NPs, though race was classified differently (White/non-White); minority racial groups were collapsed due to the small size of these groups. Physicians’ practice characteristics included practice setting (outpatient clinic/federally qualified health center [FQHC]/other setting), specialty (primary care/psychiatry), acceptance of Medicaid (yes/no), and offer a sliding fee scale (yes/no). For NPs, practice characteristics included specialty (primary care specialties/psychiatry [adult and child]) and practice setting (hospital/outpatient clinical/public or community health agency/other settings).
Public or community health settings, including FQHCs, were analyzed separately for physicians and NPs. These health care safety-net settings are required to provide access to care for underserved and marginalized populations and thus would likely be associated with providers offering specialized services such as MAT. Physicians and NPs may report multiple practice locations (up to 2 for NPs and up to 3 for physicians) when they renew their license. They were included if at least 1 practice was located in Indiana. Most Indiana physicians and APRNs reported only having 1 practice in 2021. Overall, 82% of physicians, 75% of psychiatrists and 74% of APRNs reported only having 1 practice location in 2021.30,31 The first practice identified to be in Indiana was used for this analysis. The county location of their Indiana practice was assigned a rurality status based on the designation provided by the U.S. Department of Agriculture. See Tables A1-A3 in the appendix for information on the reclassification of categorical variables.
Statistical Analysis
All analyses were conducted using SAS 9.4, with a significance threshold of α = .05. Descriptive statistics were conducted on all study variables based on providers’ reported status as MAT prescribers using the PROC FREQ procedures. Chi-square analyses were conducted in these procedures using the chisq statement to determine differences in the distribution of demographic and practice characteristics based on MAT prescription status.
Logistic regression analysis was conducted using the PROC LOGISTIC procedure. This analysis was used to identify the demographic and practice characteristics associated with the likelihood of prescribing MAT-related medications. The Hosmer-Lemeshow test was used for analyzing the goodness of fit for each logistic regression model.
Results
Primary Care Physicians and Psychiatrists
A total of 5258 Indiana-licensed physicians were included in the study, 10.1% of whom reported providing MAT. Most physicians had a primary care specialty, and more than half of the physicians in this study were male and White. Additionally, the majority of physicians reported practicing in an outpatient setting and accepting Medicaid. Over half practiced in a metropolitan center. Results from the chi-square analysis show that there were significant differences in all study variables based on MAT prescriber status (Table 1).
Descriptive Analysis for Physicians Based on Status as an MAT Provider.

Results from the Hosmer and Lemeshow goodness-of-fit test showed that the observed distributions were consistent with the theoretical distribution for the physician logistic regression analysis (χ2 = 5.728, DF = 8, P = .677). The full diagnostic test results can be found in the appendix (Table A.4). Overall, physicians had higher odds of providing MAT if they were under the age of 35 as compared to those 35 to 49, practicing in a FQHC versus in an outpatient setting, and offering a sliding fee scale at their practice (Table 2). On the other hand, physicians had lower odds of providing MAT if they were ages 50 to 64, female, identified as Asian versus White, and had a specialty in primary care versus psychiatry. Physicians practicing in a rural/metro adjacent area also had lower odds of providing MAT as compared to those in a metropolitan center.
Logistic Regression Analysis Results for the Likelihood of Physicians Prescribing MAT-related Medications.

Nurse Practitioners
A total of 3486 NPs were included in the study analysis, 352 (10.1%) of whom reported providing MAT (Table 3). Demographically, most NPs were female and White, and nearly half of NPs were between the ages of 35 and 49 years. Most NPs had a specialty in primary care and reported practicing in an outpatient clinic. Just under half practiced in a metropolitan center. Results from the chi-squared analysis indicated statistically significant differences based on NPs’ reported MAT prescriber status for age, gender, practice specialty, and practice setting.
Descriptive Analysis for Nurse Practitioners Based on Status at an MAT Provider.

Results from the Hosmer and Lemeshow goodness-of-fit test showed that the observed distributions were consistent with the theoretical distribution for the NP logistic regression analysis (χ2 = 3.8012, DF = 9, P = .924). See Table A.5 in the Appendix for the full diagnostic test results. NPs had over 3 times the odds of providing MAT if they were practicing at a public/community health agency (Table 4). However, they had lower odds of providing MAT if they were female, had a specialty in primary care, and practiced in a suburban area. No other comparisons were found to be statistically significant.
Logistic Regression Analysis Results for the Likelihood of Nurse Practitioners to Provide MAT.

Discussion
This study used state-level administrative data to identify the demographic and professional characteristics of Indiana-licensed physicians and NPs associated with the likelihood of prescribing MAT-related medications. Approximately 10% of physicians and NPs reported prescribing MAT-related medications as a part of their practice. Certain characteristics were found to be associated with the likelihood of being in this group. Among both professions, males, those with a specialty in psychiatry, and those practicing in safety-net settings, such as public and community health settings and FQHCs, were more likely to report prescribing MAT-related medications. Physicians under the age of 35 years, those who identified as White, and those who reported offering a sliding fee scale in their practice were also more likely to report prescribing these medications. Many of these findings are consistent with previous research that utilized state-level workforce data to explore the relationship between provider characteristics and their practice, highlighting the value of state-level data to provide insights and inform related workforce assessments, planning, and policymaking.28,29
Provider Data
Examining the MAT workforce requires access to timely data that can be used to quantify workforce capacity. Although there are limitations to this study’s strategy, as will be examined later in this discussion, the state-level data used for these analyses were collected and managed in a standard manner to ensure the greatest possible accuracy. 32 Challenges with accessing accurate data on the total hours MAT providers contributed to this service limited the ability to measure successful integration of MAT in primary care. Previous studies have used patient limits to estimate the number of patients who are being prescribed MAT-related medications,34-36 a strategy that has potential for overestimating the number of patients receiving MAT in their practice. The type of data used in this study may provide a solution for enhancing data collection on MAT providers and supporting longitudinal examination.
Practice Setting
Understanding where MAT providers are likely to practice is important not only for assessing provider capacity but also for identifying implementation of the primary care integration model for expanding MAT services. Study results indicate that physicians and NPs practicing in safety-net settings, public or community health or FQHCs, were most likely to report prescribing MAT-related medications. Prior studies indicate that physicians practicing in such settings are more likely to have access to comprehensive behavioral health resources that complement MAT treatment. 37 There are several models for MAT and primary care integration, all of which require administrative support for tiered care, coordinated services, and access to professional behavioral health services.38,39 However, recent research has not sufficiently assessed the effectiveness of each model and potential resource barriers that could be experienced in different practice settings. 39 Understanding the practice-specific successes and barriers for integrating MAT, and utilizing findings from this and similar studies, could help to identify a more cost-effective approach.
Gender and Practice Patterns
The statistically significant difference in gender among physicians and NPs providing MAT services most likely reflects a longstanding trend in practice patterns among male and female clinicians. While male and female PCPs provide comparable quality health care, female physicians are more likely to provide preventive services as opposed to specialized care.40,41 Additionally, female PCPs are more likely than their male counterparts to provide fewer services and work fewer hours. 42 Similarly, female psychiatrists are more likely to practice in a clinic that does not provide pharmacotherapy and work fewer hours than their male counterparts. 43 Because NPs are predominantly female, few studies have found statistically significant associations between gender and the integration of specialized services; however, a 2016 study by Hellier and Cline reported that male NPs were more inclined to integrate evidence-based care in their practice. 44 This evidence may have implications for the recruitment of both male and female clinicians to provide MAT services.
Limitations
This study has notable limitations. First, the data used in these analyses were self-reported survey data, introducing the possibility of a response bias. This limitation may be minimized by state regulation requiring physicians and nurses to provide supplemental data through a survey administered during their respective license renewals and to attest that all information provided is true and accurate. Second, this study examined cross-sectional data. Therefore, no longitudinal conclusions or implications are possible. However, the results of the descriptive and statistical analyses provide relevant and helpful information for expanding and sustaining MAT services in Indiana. Third, physicians and NPs report the services they provide as part of their overall practice and not for specific practice locations. Those who reported prescribing MAT-related medications as part of their professional practice were classified as MAT providers. There is potential that clinicians reporting multiple practice locations do not prescribe MAT-related medications at all locations. However, given that few providers report more than 1 practice, the authors are confident that these services are being provided in Indiana. Finally, no calculations were conducted to confirm if the size of the study samples was sufficient for statistical power in the analyses. However, the authors are confident in the study samples given the high representation of physicians and NPs included in the analysis.
Conclusions
There is promising evidence that PCPs and NPs can support the integration of MAT into primary care, thus increasing the capacity for this service. However, the sustainability of this integrated model relies on sufficient regulatory and administrative support, both of which may limit expansion initiatives. This study identified the characteristics of providers in Indiana who are most likely to participate in MAT. Future research could utilize the results of this study and common data elements used to examine the effectiveness of various MAT integration models on patient treatment across different practice settings.
Supplemental Material
sj-xlsx-1-inq-10.1177_00469580241237144 – Supplemental material for Exploring the Demographic and Professional Characteristics of Physicians and Nurse Practitioners Associated With Providing Medication-Assisted Treatment: A Retrospective Observational Study
Supplemental material, sj-xlsx-1-inq-10.1177_00469580241237144 for Exploring the Demographic and Professional Characteristics of Physicians and Nurse Practitioners Associated With Providing Medication-Assisted Treatment: A Retrospective Observational Study by Hannah L. Maxey, Sierra X. Vaughn, Analise Dickinson and Robin Newhouse in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-xlsx-2-inq-10.1177_00469580241237144 – Supplemental material for Exploring the Demographic and Professional Characteristics of Physicians and Nurse Practitioners Associated With Providing Medication-Assisted Treatment: A Retrospective Observational Study
Supplemental material, sj-xlsx-2-inq-10.1177_00469580241237144 for Exploring the Demographic and Professional Characteristics of Physicians and Nurse Practitioners Associated With Providing Medication-Assisted Treatment: A Retrospective Observational Study by Hannah L. Maxey, Sierra X. Vaughn, Analise Dickinson and Robin Newhouse in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-xlsx-3-inq-10.1177_00469580241237144 – Supplemental material for Exploring the Demographic and Professional Characteristics of Physicians and Nurse Practitioners Associated With Providing Medication-Assisted Treatment: A Retrospective Observational Study
Supplemental material, sj-xlsx-3-inq-10.1177_00469580241237144 for Exploring the Demographic and Professional Characteristics of Physicians and Nurse Practitioners Associated With Providing Medication-Assisted Treatment: A Retrospective Observational Study by Hannah L. Maxey, Sierra X. Vaughn, Analise Dickinson and Robin Newhouse in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-xlsx-4-inq-10.1177_00469580241237144 – Supplemental material for Exploring the Demographic and Professional Characteristics of Physicians and Nurse Practitioners Associated With Providing Medication-Assisted Treatment: A Retrospective Observational Study
Supplemental material, sj-xlsx-4-inq-10.1177_00469580241237144 for Exploring the Demographic and Professional Characteristics of Physicians and Nurse Practitioners Associated With Providing Medication-Assisted Treatment: A Retrospective Observational Study by Hannah L. Maxey, Sierra X. Vaughn, Analise Dickinson and Robin Newhouse in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors have no acknowledgments for this manuscript.
Author Contributions
Hannah L. Maxey contributed to the study design, study analysis, literature review, and manuscript development.
Sierra X. Vaughn contributed to the study design, study analysis, literature review, and manuscript development.
Analise Dickinson contributed to the literature review and manuscript development.
Robin Newhouse contributed to the study analysis, literature review, and manuscript development.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received funding support for the research, authorship, and/or publication of this article through the Indiana University Grand Challenge: Responding to the Addictions Crisis.
Ethical Approval
This study was approved under the Indiana University Institution Review Board (Protocol # 1909917756).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.