
Abstract
Compared to younger adults, older adults who smoke cigarettes are half as likely to make a quit attempt, but more likely to maintain abstinence using evidence-based smoking treatments (EBSTs), illustrating the need for motivational messages to promote cessation through EBSTs. It is unclear whether messaging regarding the association between smoking and dementia might motivate older adults to quit. We conducted 90-min semi-structured qualitative interviews and surveys via telephone with 24 U.S. older adults who smoke (ages 50-75) with no cognitive impairment history. Rapid content analysis revealed the most reported health-related concern of aging was dementia/cognitive loss/loss of functioning. However, most participants were unaware of the association between cognitive decline and smoking. Participants had seen previous smoking cessation advertisements, but most did not feel motivated to quit by them. The majority found a message about smoking raising dementia risk and quitting decreasing that risk to be motivational for cessation. Exact message content preference varied, but 2 broad categories arose: hope- and fear-based messages. Most participants stated willingness to use some cessation pharmacotherapy and half were willing to use cessation counseling. Participants preferred messages to come from older adults who were successful quitters. To our knowledge, this was the first study to explore potential motivational messages targeting older adult smokers, including the potential acceptability of a dementia-related message in this context. This work supports patient desire for targeted motivational messages for older adult smokers. Messages highlighting the link between smoking and dementia are perceived to be motivational for this group; future work should compare a hope- to fear-based messages.
We need to motivate quitting in older adults who smoke because older adults are half as likely to try to quit smoking as younger adults but are more successful at quitting when they use evidence-based treatment.
We found that dementia is an important health consequence for older adults who smoke, but the impact of smoking on dementia is unknown to this population and could motivate cessation.
The link between dementia and smoking should be disseminated as a motivating message for cessation, and a hope- and fear-based cessation message should be tested for efficacy in motivating cessation attempts among older adults who smoke.
Introduction
Smoking remains the leading preventable cause of death and disability in the United States (U.S.), resulting in 480 000 preventable deaths per year.1,2 Although tobacco prevention and treatment efforts have successfully reduced adult smoking rates in the U.S. over the past 2 decades, older adults remain stagnant in their cessation rates. Since the year 2000, older adults who smoke in the U.S. remained less likely to make a quit attempt and half as likely to quit compared to younger adults who smoke. 3 Consequently, there has been only a 2.1% reduction in smoking prevalence among people who smoke ≥65 years, versus a 27.7% reduction in smoking prevalence among adults overall. 4 This is particularly problematic as older adults who smoke bear a disproportionate burden of the health consequences of smoking. 1 Given the expected doubling of the older adult population in the next 30 years, increasing smoking cessation among this population is a vital public health priority. 5
Lower cessation efforts among older adults who smoke may be due to misconceptions/motivational deficits among older adults who smoke, longer experiences with smoking, and elevated nicotine dependence. Doubts about the benefits of quitting for older adults and the efficacy of evidence-based smoking treatments (EBSTs) may also reduce older adults’ who smoke attempts to quit. 6 These doubts may stem from decades of smoking and multiple potential failed quit attempts throughout this time. Importantly, EBSTs are more effective for older adults who smoke than for younger counterparts. 6 This is particularly relevant as U.S. adults ages 50 and older who smoke have higher nicotine dependence levels than younger counterparts, highlighting the importance of using cessation medication during quit attempts. 7 It is imperative that we develop strategies to motivate older adults who smoke to make quit attempts and to ensure that when they do, they use EBSTs.
The first national, federally funded, antismoking initiative (TIPS From Former Smokers) demonstrated that presenting specific negative health effects and their impact on quality of life could successfully increase smoking cessation efforts (ie, 9.15 million quit attempts and >522 000 sustained quits in 3 years). 8 However, this campaign produced fewer quit attempts among older adults than younger adults, potentially due to the original target audience of the campaign. 9 This campaign was targeted toward currently smoking adults in the U.S., ages 18 to 54 years old, and therefore may not have represented the most relevant health consequences of older adults. 10 Limited campaign effects for older adults who smoke may have been due to older adults’ who smoke lack of knowledge about the efficacy of EBSTs, lowered self-efficacy due to previous unsuccessful quit attempts, and beliefs that it is too late to reap the health benefits of cessation.11-13
According to the Health Belief Model (HBM), impactful motivational messages for older adults who smoke should focus on health threats they perceive as important and personally relevant and messages should be offered with a feasible, effective course of action to address the health threat. 14 Older adults’ greatest aging-related fear is cognitive decline associated with developing dementia15,16; this illness is both important and personally relevant. Cigarette smoking is prospectively associated with a 70% increased risk of Alzheimer’s disease dementia onset and is 1 of the 8 known modifiable risk factors for dementia.17,18 Smoking cessation, even in an older adult population, has been shown in longitudinal cohort studies to reduce the risk of Alzheimer’s disease and related dementias (ADRD) and slow cognitive decline.18-20 The link between smoking and ADRD risk coupled with availability of EBSTs may offer an effective strategy to respond to this threat. Unfortunately, the link between smoking and ADRD risk has not been clearly articulated to general or medical communities and is not used as a motivator for smoking cessation in theU.S.2,8
To address this need to identify effective, motivational messages specifically for older adults who smoke, we used qualitative methods to identify patient-centered health-related messages with especially high potential to: (1) motivate smoking cessation attempts by older adults; and (2) increase EBST use. We hypothesized that the link between dementia and smoking might serve as novel motivational content for this group of older adults who smoke.
Methods
Participants and Procedure
Participants were recruited for a telephone-based study using Facebook advertisements (Advertisements invited participants between the ages of 50 and 80 who currently smoke cigarettes to call or complete an online screener (via Qualtrics XM; Qualtrics). The minimal age of 50 was used as this is the designation of “older adults” in the most recent tobacco cessation guidelines. 21 Initial inclusion criteria included: ages 50 to 80 years old and self-reporting smoking ≥5 cigarettes per day (CPD), and no self-reported history of either dementia or Mild Cognitive Impairment (MCI), confirmed via cognitive screener (MOCA-BLIND score ≥19) after obtaining consent. 22 The screener also identified gender, race, and asked participants to write their “biggest health-related fear of aging.” After screening for initial eligibility, potential participants scheduled their 90-min telephone interview.
During the phone interview, potential participants provided informed verbal consent for study procedures and completed the MOCA-BLIND cognitive screener to confirm eligibility. Individuals who failed the cognitive screener were discontinued from the study and were mailed a $10 check to compensate for their time. Eligible participants went on to complete a 60-min semi-structured qualitative interview, followed by a 15 min survey completed over the phone. Qualitative interviews were recorded and transcribed for analysis. Participants were compensated $50 for their time and efforts. All study procedures were reviewed and approved by the local Institutional Review Board.
Qualitative Data Collection and Analysis
The interview guide was intended to identify content that could motivate a smoking cessation attempt and the use of EBST among older adults who smoke (Appendix 1). The guide queried participants about their previous experiences with smoking cessation public health campaigns, HBM 14 domains of barriers to quitting and benefits of quitting, susceptibility (ie, how likely they are to get a disease and how much is it related to their smoking), and severity (how important is the disease to them) of health-related fears of aging identified in their screening survey. Participants were then provided brief psychoeducation on the association between cigarette smoking and ADRD risk and queried about their perceived susceptibility and severity of cognitive decline and ADRD, understanding of the benefits of quitting, motivational impact of the psychoeducational information, self-efficacy in quitting, and access to EBSTs. Interviews were conducted by a bachelor’s level health counselor with training in conducting qualitative interviews, and a PhD level clinical psychologist (ALJ), with expertise in designing, conducting, and analyzing qualitative interviews. Both interviewers were involved in analysis of the collected qualitative data.
Transcriptions were first analyzed using a rapid analytic approach. Rapid qualitative analysis is a systematic and rigorous process, used to condense and review data in an efficient manner to ensure progression of research in a timely manner.23-25 It has been previously used in healthcare and tobacco dependence-related research and has been shown to generate codes similar to more in-depth analytic processes.26,27 Summaries of participant responses were pulled from transcripts and organized by domains (aligned with questions from the interview guide) in an MS Excel matrix. 28 ALJ reviewed the initial 5 summaries and generated an initial set of thematic codes for each domain. Then coders independently reviewed summaries and assigned codes to participants. Coders met on a weekly basis for consensus meetings to resolve any coding discrepancies, and, when appropriate, generate new themes, resulting in a recoding of the entire dataset. If summaries provided in the matrix resulted in discrepant codes and a consensus could not be reached, the coders reviewed the original transcript of that participant’s data during the consensus meeting to come to mutually approved agreement. For added rigor and to ensure no subtleties in context were missed ALJ later independently reviewed the full transcripts using Atlas.ti (Version 9.1.7.0 Windows) 29 and applied a directed content analytic approach. 30 Directed analysis incorporates the researcher’s knowledge of existing theory to extend the understanding of a topic of interest using a primarily deductive approach. 30 Due to the small sample sizes in qualitative analyses (cf. quantitative analyses), results are not used for statistical comparison. However, unlike most qualitative analyses, content analyses allow for frequency of codes to be presented in order to provide additional interpretation of the data.30,31 The same domains used in the rapid analysis guided this supplemental analysis, and development of codes was similarly based on existing theory which was inherently written in the semi-structed interview guide.
Survey Measures and Quantitative Analysis
Survey questions assessed socio-demographic information, psychiatric history (current and past diagnoses coded as “absent” or “present”), smoking use history, and nicotine dependence. The time to first cigarette 32 was used to determine dependence level (“High” = smokes in the first 30 min of the day vs “Low” = smokes after 30 min) consistent with prior research. 33 Descriptive analyses were calculated using IBM SPSS Statistics (Version 26).
Results
Quantitative Results
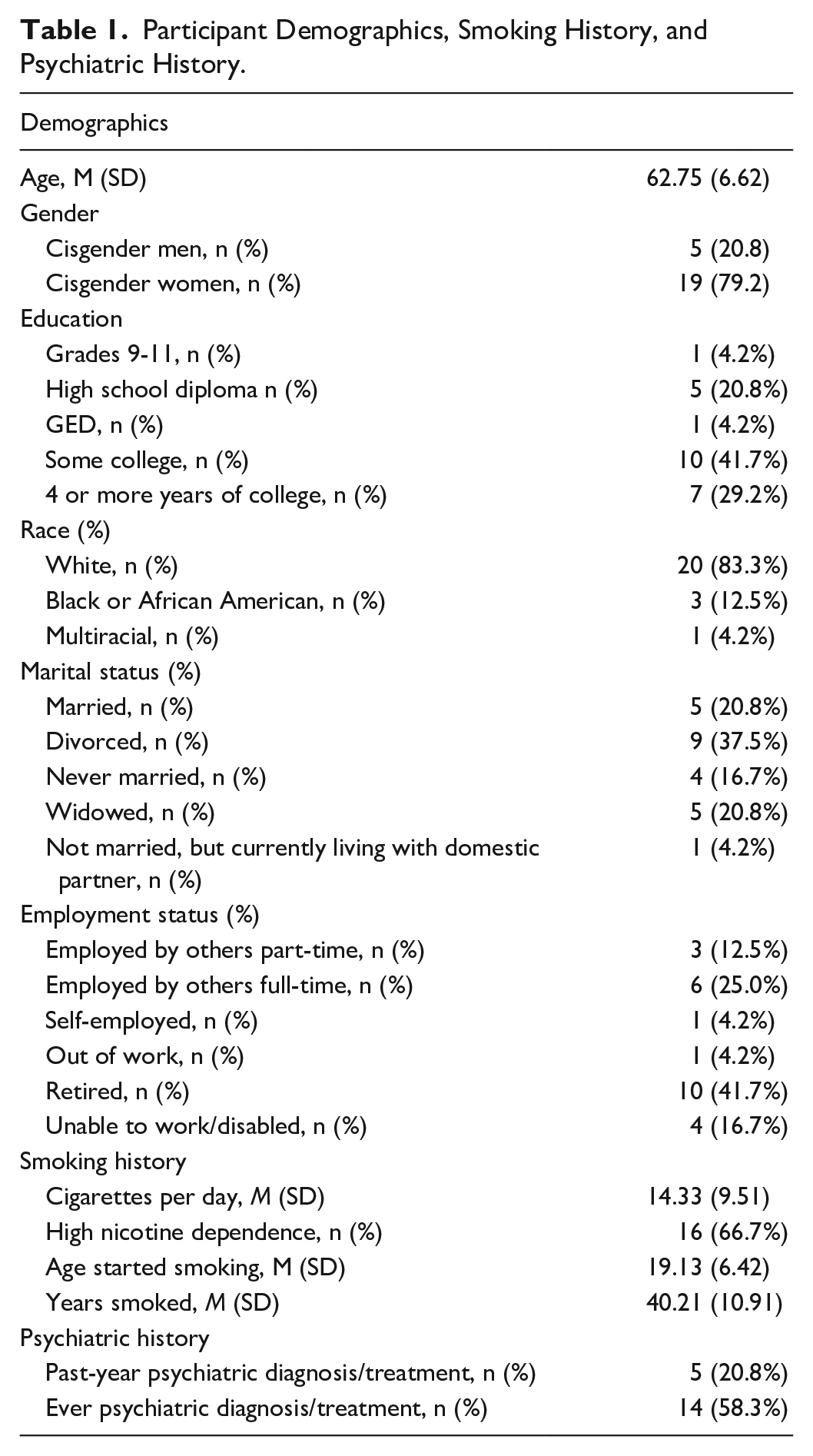
Twenty-four adults between the ages of 50 and 75 completed the study. An additional 10 participants passed the initial eligibility screen and provided consent, but did not pass the cognitive screener. See Table 1 for full demographic, psychiatric, and smoking information.
Participant Demographics, Smoking History, and Psychiatric History.
Qualitative Results
Previous exposure to smoking cessation advertisements
All participants reported previous exposure to advertisements, with various modalities and messages. Common advertisement content themes included: risks of smoking, evidence-based treatment options, and benefits of quitting. The most common advertisement modality reported was television, followed by pamphlets in a doctor’s office, print materials (ie, newspapers, magazines), and the internet. Although all participants had previously seen advertisements, most did not feel motivated by them. Other common themes related to reactions to advertisements, in order of frequency, were: thinking about quitting without making an attempt, feeling that ads were off-putting, feeling negative about themselves, questioning the authenticity of advertisements, and reporting that advertisements were not memorable, were unrelatable or unlikely to be relevant for them (ie, the highlighted consequence would not happen to them), and that they led to a short, unsuccessful quit attempt (Table 2). Some participants actively looked away from advertisements (P15: “. . .I mean, it’s kind of overwhelming and look away and [I] pray. . .that that doesn’t happen to me”) while others demonstrated optimism bias (P1: “I think in the back of my mind. I think, well, well that isn’t going to happen to me.”).
Influence of Previous Cessation Advertisements.

Benefits and drawbacks of smoking
Participants reported a variety of benefits from smoking. In order of reported frequency, smoking benefits were: relaxation, feels rewarding or pleasurable, occupies me, satisfies cravings, tastes good, appetite control, and no benefits.
Smoking drawbacks included (in order of frequency): it is dirty and smells bad, cost, stigma/judgment from others, exacerbates health conditions/symptoms, future health risks, inconvenient (eg, must go outside to smoke), not in control (ie, the cigarettes control me), isolating, a “nasty habit,” and bad example for others.
Greatest health concern (severity)
Participants reported many aging-related health concerns when asked their greatest aging-related health concern, with dementia/cognitive loss/loss of function being the most common (P16: “I guess there is nothing physically wrong with me. I don’t take medication for anything. I don’t have diabetes. I don’t have thyroid . . . And if I did, that’s something I could control. . . . dementia you cannot control.”). The other most common health risks, in order of frequency, were: cancer, heart attack, lung diseases (ie, COPD and emphysema), pain/arthritis, falling, death, mobility issues, and difficulty accessing medical care (Figure 1).
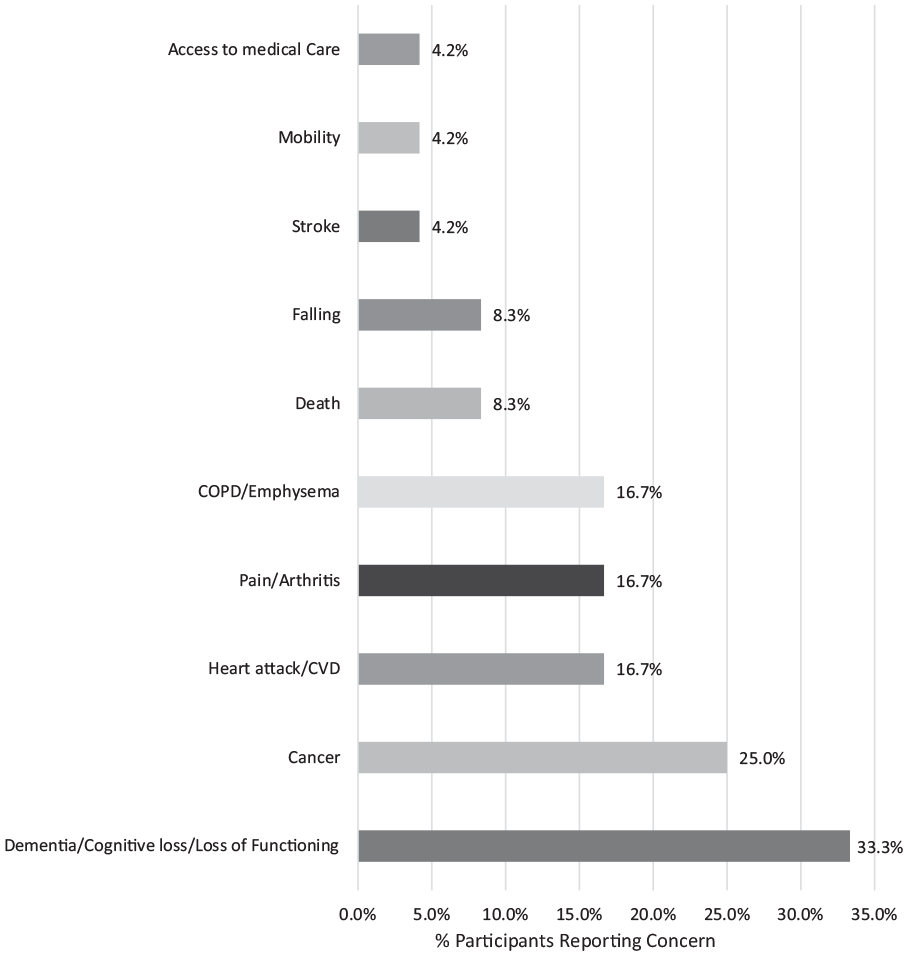
Greatest health-related fears of aging.
Susceptibility to feared diseases and benefit of quitting
When participants were asked about how likely they are to develop their most feared health concern, over half believed they will very likely get it, and 3 of the 16 individuals reporting strong susceptibility to their stated fear stated they are already experiencing symptoms of this health issue. Importantly, although some participants were experiencing symptoms of their greatest health-related fear, or had family members with known health consequences of smoking, they reported this did not impact their motivation to quit. There was a common theme of fatalism due to their age, and potential impacts of smoking on health (P23: “Their mindset already is that, you know what, f— it. I’ve lived this long. I’m going to do – I want to go out doing what I want to do.”). Almost all of participants believed quitting smoking would lower their future risk of getting their most feared disease, while only a few individuals believed smoking was unrelated to their greatest aging-related health concern. Of note, half of the individuals who most feared dementia or loss of cognitive functioning were unsure or doubtful that smoking was related to their health risk. In comparison, all participants who most feared cancer believed that they were likely to get cancer related to their smoking (P8: “Well, I’ve been smoking for over 50 years. And odds are, it seems, that that [cancer] will be what kills me.”) and that quitting would lower their risk of getting cancer (P12: “. . .if I were to quit, my chances are going to be better to not get cancer than they are at this point.”).
Barriers to quitting smoking
Common themes surrounding barriers to quitting smoking included: habit/behavioral addiction, lack of desire/motivation to quit, stress, fear of failure/anxiety, physical addiction, smoking is pleasurable, boredom, difficulty accessing treatment, treatment costs too much, lack of confidence in quitting, and being around other people who smoke. Other themes mentioned included not having other ways to control weight, overconfidence in ability to remain quit, and use of other addictive substances.
Dementia and smoking link
Half of the participants were naïve to the link between smoking and dementia, and only 5 were aware of any specifics of this relation. Most participants felt strongly that information about the link between smoking and ADRD should be shared with the public; some were confused and upset that they did not yet know this information (P23: “I never heard up until you let me know this. I never– all those facts, I’ve never heard of before, never, nowhere. I think that should be brought out to the public.”).
Preference for exact message content varied, although 2 general themes for preferences emerged: fear-fear based messages (P8: “. . . one commercial that’s really effective when they show you someone who is pretty near death. And that’s very scary. . .”) and hope-based messages (P36: “Something that probably emphasizes the benefits rather than the risks.”). Almost all participants believed a message linking smoking to dementia risk was motivational, with some noting that their family connection with dementia increased the motivational impact of this message (P19: “. . .Sometimes I worry about Alzheimer’s and that . . . my mother was getting forgetful before she ever died. And it kind of makes me think twice because I have no children and nobody to take care of me. So I’m like, yeah, I should quit because I’m kind of– I mean, I’m on my own.”). Over half of participants believed an ADRD-risk message was more motivating than previous advertisements. There was no clear preference for advertisement wording of “Alzheimer’s disease” or “dementia.”
Themes of preferred message imagery included: personal/emotionally salient and relatable images, image of dementia occurring, not recognizing kids, image of family members/kids, infographic of increased risk, healthy versus diseased brain, list of risk factors, and visual of benefits of quitting.
Treatment experience, preferences, and access
Participants were asked about willingness and effectiveness of each smoking cessation medications and counseling separately. Most participants were willing to use at least 1 form of medication; over half of individuals reported willingness to use selected (vs all) medications even after previous experiences with unwanted negative side effects. Similarly, most participants believed medications would be helpful in quitting, and almost all of those who didn’t believe medication could help them quit thought medications could benefit others.
Smoking cessation counseling was largely a novel idea for participants (P2: “They have nutrition counselors and stuff like that over there. They’ll always refer you for something like that. But yeah, I never thought to see if they had smoking cessation therapists or something.”). One participant believed counseling should be reserved for traumatic events (P16: “. . .Counseling isn’t going to get you over a bad habit. . .If somebody was abused as a child they go to counseling. Somebody was beat up, somebody was raped, things like that.”). Although many had not previously considered counseling, over half reported willingness to try it in a future quit attempt, and the majority believed it would be helpful for them (2 participants thought counseling wasn’t right for them but believed it would help others in their position). Participants noted the importance of not being judged by a cessation counselor, ensuring counseling would be easily accessible, and that counseling could be particularly helpful for changing the behavioral aspects of smoking.
There was no clear preference for individual versus group counseling format, or modality (in person, telephone, video). The most preferred counselors were people who used to smoke, particularly those who are non-judgmental and have similar experiences. Participants also reported a desire for a support/peer group, like Alcoholics Anonymous. Only 2 of the 24 participants preferred a doctor to provide cessation counseling.
Access to EBST was asked about in a combined manner (ie, medications and/or counseling). Regarding EBSTs access, participants noted that when ready to discuss cessation treatment options, their doctor was the primary person they would go to and that they want their doctor to follow up on their cessation progress. Other less commonly preferred access points included local drugstore, Quitline, and local senior center. When discussing access, many participants listed poor insurance coverage and limited healthcare access as barriers to receiving EBST. When discussing who participants would want to hear messaging about EBST from, there was a clear preference for messengers of similar age who formerly smoked. (P11: “. . .someone who’s been in your shoes, so to speak. Where you’ve been, who has gone through it, and who has proven that it’s not too late. You’re not too old. You can still reap the benefits basically.”).
Discussion
This qualitative study of 24 older adults who smoke was designed to inform the development of a participant-centered motivational advertisement for older adults who smoke. Despite all participants reporting previous exposure to cessation advertisements, they were not motivated by these advertisements and at times felt worse about themselves and unwilling to quit. To our knowledge, this was the first study to explore potential motivational messages targeting older adults who smoke, including the potential acceptability of a dementia-related message.
Like the general older adult population, dementia, cognitive decline, and loss of functioning were the most commonly reported “greatest aging-related health concern” identified by participants.15,16 However, participants were largely unaware of the link between smoking and dementia. Overall, the dementia-smoking link was highly motivational for smoking cessation and participants noted the importance of disseminating this message to the public. The increased risk of dementia related to smoking as well as the reduction of that risk when quitting at an older age were particularly important. Further, for those that did not report dementia as their greatest aging-related health concern, they believed that the dementia-smoking link was more motivational for quitting smoking than their initially reported feared-health condition. This change in motivation also occurred among many of the participants who endorsed themes of fatalism when discussing susceptibility to their feared health conditions and limited benefits of quitting.
This research also provided important information on how such dementia-smoking risk messages should be delivered. Participants endorsed the use of both hope- (ie, “what would I gain from quitting”) and fear-based (ie, “what would I lose if I kept smoking”) advertisements. They also reported a desire for representation of older adults who formerly smoked in advertisements, with a particular emphasis on emotionally salient messages.
These 2 general themes of fear and hope are consistent with prospect theory (eg, gain-loss theory), 34 which has been previously researched in tobacco cessation messaging among younger and middle-aged adults. A 2007 study of young and middle-aged adults who smoke found that gain-based (vs loss-based) messages are more effective in promoting early cessation success for those engaged in medication-aided treatment. 35 A more recent study found that positively framed (hope-based) messages are more motivational than negative-based messages in prompting smoking cessation attempts, but did not focus on older adults. 36 A study of both smoking and non-smoking college undergraduates found that positive (hope-based) smoking cessation messages were more motivational than negative (fear-based) messages. 37 Conversely, there is strong empirical support for emotionally-laden and graphic antismoking advertisements increasing population-level cessation attempts; however, the odds of making a quit attempt were lower among people adults ages 65 and older who smoke compared to 18 to 24 year olds. 38 Hope- versus fear-based messages to motivate smoking cessation specifically among adults aged 50 and older has yet to be examined. Further, a message highlighting the increased risk of dementia from smoking and beneficial impact of quitting on dementia risk, has yet to be tested in this population.
An important part of a messaging strategy for older adults includes increasing engagement in EBSTs. There was some apprehension regarding cessation medications due to previous negative side effects; however, most participants believed some form of cessation medication would be helpful to quit and were willing to try at least 1 medication during a future quit attempt. Although many participants were unaware of the availability of cessation counseling, over half reported a willingness to use counseling. Participants reported wanting to feel supported, heard, and not judged by cessation counselors. When discussing potential ways to do this, many participants referenced Alcoholics Anonymous, with an emphasis on similarly aged peers, which they liked for its availability and camaraderie.
The most preferred messenger for promoting EBSTs was someone who formerly smoked of similar age who had succeeded in their attempt. This aligns with multiple theories of persuasion in health communication (Elaboration Likelihood Model, Transportation Theory) highlighting the benefit of using narratives with protagonists who the target audience can identify and empathize with to promote changes in behavioral intentions and beliefs.39-42 This may also explain why previous campaigns were not as effective among older people who smoke.
Study limitations and strengths must be considered. The convenience sample used in this study was predominantly white and from a midwestern state and thus not nationally representative. Although all participants were recruited using Facebook advertisements, other community recruitment efforts were made including flyers in local residential adult living centers, and community-based recruitment efforts by the Wisconsin Community Academic Aging Research Network. Future work should evaluate the importance of culturally specific messages to assess acceptability and differential effectiveness for various communities. Participants were primarily recruited online (although other recruitment methods were used), potentially providing a biased sample. Recruitment of older adults who do not use social media may offer different results. Although completing the visit via telephone may have limited the sample to those comfortable with this form of interaction, it also allowed for greater reach to different geographic areas and provided a safe form of communication during the pandemic among individuals at high risk for COVID-19.
Results of this preliminary study support the development and testing of novel motivational messages for older adults who smoke to promote smoking cessation and use of EBST. Findings suggest the promise of using hope- and fear-based messages centered on the dementia-smoking link using narrative communication from older people who formerly smoked. Given the preliminary nature of this study and homogeneity of sample queried, future research efforts should: (a) work to develop messages using the link between smoking and dementia, (b) use randomized control trials to test this message content (vs control messages) for initial acceptability and efficacy in older adults, and (c) examine whether this message content would be motivational in a more racially diverse population.
Supplemental Material
sj-docx-1-inq-10.1177_00469580241236416 – Supplemental material for Qualitative Message Development to Motivate Quitting Smoking in Older Adults: Dementia May Motivate Quitting
Supplemental material, sj-docx-1-inq-10.1177_00469580241236416 for Qualitative Message Development to Motivate Quitting Smoking in Older Adults: Dementia May Motivate Quitting by Adrienne L. Johnson, Sara Doyle, Carey E. Gleason, Jessica Cook, Jane Mahoney and Megan E. Piper in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors would like to acknowledge Tess Kuba for support in conducting study interviews and helping analyze study data. We would additionally like to thank all the study participants without whom this research could not have been completed.
Authors Contributions
Data Availability
The data generated and/or analyzed in this article are not publicly available to protect participant confidentiality given the qualitative nature of the study. They can be made available upon reasonable request from the author and through local institutional review board approval.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a career development award from the National Institute on Aging at the National Institutes of Health to ALJ (grant number K23AG067929).
Ethics Statement
This study was approved by the University of Wisconsin School of Medicine and Public Health Institutional Review Board (IRB #: 2020-1429).
Consent Statement
Verbal consent was obtained from participants prior to engagement in any study activities.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.