
Abstract
As e-cigarette use has steadily increased over the recent years, the public health interest in the potential implications of e-cigarette use on cigarette smoking has grown in parallel. With strict adherence to PRISMA guidelines, this systematic review examined the potential associations between e-cigarette use and relapse to cigarette smoking among former cigarette smokers. The protocol was registered on November 06, 2018 (PROSPERO 2018 CRD42018115674). Literature searches were executed from January 01, 2007 to August 20, 2022 and search results were screened according to the PICOS review method. One RCT and 10 adjusted studies examined relapse to cigarette smoking (evidence grade “moderate”) among regular e-cigarette users, reporting mixed and inconsistent findings according to varying definitions of e-cigarette use and relapse. Findings were similarly inconsistent among the 8 adjusted studies examining relapse to cigarette smoking among non-regular e-cigarette users. The inconsistency in findings among studies evaluating regular measures of e-cigarette use, combined with the numerous methodological flaws in the overall body of literature, limit the generalizability of results associated with a causal association between e-cigarette use and relapse to cigarette smoking. Based on findings from this review, more robust studies are required to determine whether a causal association exists between e-cigarette use and relapse to cigarette smoking. Future studies should apply consistent measures of regular e-cigarette use to examine causality with future use patterns, and sufficiently account for known or suspected confounding variables to support inform determinations related to e-cigarette use and cigarette smoking behaviors.
Empirical evidence suggests that e-cigarettes present fewer health risks than combustible cigarettes due to the fact that vapor from inhaled e-cigarettes contains far less of the approximately 7000 chemicals present in cigarette smoke.
Numerous recent systematic reviews have examined the relationship between e-cigarette use among cigarette smokers and changes in continued cigarette smoking; however, few have considered smoking relapse, and none have explored relapse as an explicit outcome measure.
Based on the findings of this review, the available studies do not sufficiently measure e-cigarette use in a manner consistent with regular, established use, do not consistently define relapse in terms of a return to regular cigarette smoking, and do not sufficiently account for known or suspected confounding variables to support robust determinations related to e-cigarette use and cigarette smoking behaviors.
Introduction
Electronic cigarette (e-cigarette) use has rapidly increased over the past decade while cigarette smoking prevalence has declined in parallel.1-4 Empirical evidence suggests that e-cigarettes present fewer health risks than combustible cigarettes; specifically, it has been reported that vapor from inhaled e-cigarettes contains far less of the approximately 7000 chemicals present in cigarette smoke.5,6
The public health issue of the potential association between e-cigarette use and cigarette smoking continues to grow in importance and controversy.7-9 An objective examination of the relationship between e-cigarette use and the use of combustible cigarettes is necessary to understanding the public health implications of the growing e-cigarette product category. 6
Some of the widely published topics on e-cigarette use include the potential of youth transitioning from e-cigarettes to cigarette smoking and the risk of existing cigarette smokers quitting cigarette smoking and adopting e-cigarette use. 6 There is also public health concern of dual use risk if e-cigarettes are not used as a short-term, interim product to migrate away from cigarette smoking {Pierce, 2021 #73}. These potential risks require an assessment of causality to understand the public health effect of e-cigarettes. Furthermore, measurement of risk associated with e-cigarette use and whether those risks offset the benefits to public health. These are critical considerations for the development of future regulatory strategies. 6
The current qualitative systematic review synthesized evidence on the potential associations between e-cigarette use and relapse to cigarette smoking among current and former cigarette smokers. A general understanding of the available published literature on e-cigarette use and cigarette smoking informed the a priori identification of outcome measures. Numerous recent systematic reviews have examined the relationship between e-cigarette use among cigarette smokers and changes in continued cigarette smoking; however, few have considered smoking relapse,10,11 and none have explored relapse as an explicit outcome measure. Consequently, the current systematic review provides a unique focus on cigarette smoking relapse, a key measure along the smoking cessation trajectory, and provides a unique and timely update to previously published reviews in a rapidly growing evidence base on e-cigarette use.
Methods
Overview
The methods and results reported correspond to a larger systematic review addressing the key research question, “Are there any potential associations between e-cigarette use among cigarette smokers and changes in continued cigarette smoking?” The current review focuses only on the identification and characterization of any potential associations between e-cigarette use and relapse to cigarette smoking among former combustible cigarette smokers.
The registered review protocol can be located in the PROSPERO database (The International Prospective Register of Systematic Reviews; registered on November 06, 2018; PROSPERO 2018 CRD42018115674; https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=115674).
This review was executed with strict adherence to the standards of systematic review methodology (“high” overall rating by A MeaSurement Tool to Assess systematic Reviews [AMSTAR] 2) 12 and reporting (Preferred Reporting Items for Systematic Reviews and Meta-Analyses [PRISMA]). 13
Terminology
Supplemental Section 1 provides a comprehensive table of terminology applied in this review.
Literature Search Methods
A comprehensive search of MEDLINE, EMBASE, and PsycINFO was executed by an information specialist. The applied search terms used medical subject headings (MeSH) and terms related to e-cigarette use, cigarette smoking, and cigarette smoking cessation. The initial database search was completed on October 15, 2018 and included articles published from January 1, 2007 to October 15, 2018. A second search was executed on October 17, 2019 including articles published from January 1, 2018 to October 17, 2019. An additional literature search update was conducted on January 5, 2021 including publications from January 1, 2019 to January 5, 2021. The most recent literature review update was completed on August 20, 2022 to include references published between January 6, 2021 and August, 20, 2022. As reported, overlapping search timeframes beginning with the first of the corresponding year were executed to ensure a complete and comprehensive search. Search dates began in 2007 as the first year that e-cigarettes were introduced to the mass market in the U.S.5,6 Supplemental Section 2 presents the complete search strategy.
Eligibility Criteria
The review screening process was defined by the PICOS (Population or participants and conditions of interest, Interventions or exposures, Comparisons or control groups, Outcomes of interest, and Study designs) review methodology (see Supplemental Section 3). No age restriction was applied to the population of interest, and the interventions and controls were e-cigarette users and non-users, respectively. The primary outcome measures identified a priori included: abstinence/quitting from smoking cigarettes, duration of abstinence from cigarette smoking, quit attempts made to abstain from cigarette smoking, age at quit attempt/quitting from cigarette smoking, change in cigarette smoking quantity/frequency, and relapse to smoking cigarettes. Initial scoping searches indicated limited available evidence from randomized controlled trials (RCTs); therefore, the review was not limited by study design, although results from RCTs, where available, were considered the highest level of evidence. The search strategy considered published peer-reviewed literature; theses and dissertations; government and industry documents; clinical trial registries (clinicaltrials.gov); a gray literature search of Google Scholar; and the checking of reference lists of included studies. Additionally, consultation from content experts in the field was sought when appropriate. Due to review team language fluency constraints, only English-language studies were included.
Although the evaluation of regular e-cigarette would provide the strongest evidence, this review was designed to capture the broader evidence base. Given the potential loss of data by limiting inclusion criteria to regular e-cigarette use, this restriction was no applied.
Evidence Synthesis
This review used DistillerSR (Evidence Partners, Ottawa, Canada) to manage data extraction. Articles were screened by two reviewers, independently, based on the predefined criteria, and started with the title/abstract level. Then, full-text articles were obtained for studies that were not excluded at the title/abstract level. Review discrepancies were resolved between reviewers, with any unresolved disagreements adjudicated by a third expert reviewer. All reasons for exclusion were documented. Full details are presented in Supplemental Sections 3 and 9.
Data extraction forms were created in DistillerSR. Data extraction was independently performed by one reviewer, and checked by a second reviewer and discrepancies were resolved, first, through discussion between the 2 reviewers. Resolution only included a third team member, with consideration of the specific publication and the specific details of conflict, if consensus was not met between the 2 reviewers.
Statistical differences between e-cigarette and non-e-cigarette users are presented for each of the included studies according to 95% confidence intervals (CIs) or statistical significance (ie, p-value). Results are specified as “significant” and/or “significantly” to indicate statistical significance (ie, p < 0.05 and/or CI excludes 1.0).
Sensitivity Analyses
Sensitivity analyses were planned, data permitting, to include stratification of results (or removal of data inputs) from: studies that did not adjust for meso- and macro-level variables in addition to age, race/ethnicity, and gender; studies that did not define e-cigarette use or regular cigarette smoking, and with a questionable definition of e-cigarette use and/or regular cigarette smoking. Additionally, stratification by age group, data permitting, and a sensitivity analysis of age, were planned.
Assessment of Confounding
The Socio-Ecological Model created by McLeroy et al. 14 served as the theoretical framework of this review. According to this framework, individuals and their interrelationships in their social (micro-), physical (meso-), and policy (macro-) environments were considered. Further detail is provided in Supplemental Section 4.
The following steps were taken in accordance with Cochrane guidelines for systematic reviews to evaluate confounding factors 15 :
A priori potential confounding factors were defined based on the evidence and expert opinion of research team members and external advisors
Additional variables reported by authors from the evidence base were considered for additional post hoc synthesis.
Outcomes and Related Psychometrics
Recognizing that all the outcome measures are not equally valid and reliable, this review examined Contextual Questions (CQs). These CQs were defined to examine the psychometric reliability and validity of outcome measures applied to the examination of the associations between e-cigarette use among cigarette smokers and changes in continued cigarette smoking. 16 Further detail on the CQ assessment can be found in Supplemental Section 5.
Study Quality Assessment
Two review team members independently appraised study quality using the Downs and Black checklist. 17 Each included study was graded “excellent,” “good,” “fair,” or “poor.” Further information is provided in Supplemental Section 6. Publication bias, which may be assessed by funnel plots, requires 10 or more RCTs included in a meta-analysis. However, with the limited evidence from RCTs examining relapse to cigarette smoking, an assessment of publication bias was not feasible.
Strength of Evidence Evaluation
Strength of evidence (SOE) evaluations were assessed separately for: (1) RCTs; (2) studies that controlled for age, gender, and race/ethnicity; and (3) studies that did not control for key confounders. The overall SOE graded was determined to be “high,” “moderate,” “low,” or “insufficient” according to the Agency for Healthcare Research and Quality (AHRQ) Evidence Based18-20 Practice (EPC) grading system (Supplemental Section 7).
Results
Overview
The larger review, from which relapse to cigarette smoking is reported from, identified a total of 8443 articles that were retrieved from the specified databases, with 4 additional articles that were identified through other sources (total: N = 8447). Of the 8447 potentially relevant articles, 6509 were excluded at the title/abstract level, resulting in 1940 articles eligible for review at full-text level (Supplemental Section 8). Subsequently, 1726 articles were excluded if they did not meet inclusion criteria (Supplemental Section 9), resulting in 214 studies eligible for inclusion in the larger systematic review (Supplemental Section 10). The weighted overall kappa for inter-rater reliability at Level 2 screening was 0.86. All selection steps are presented in Figure 1 (PRISMA flowchart).
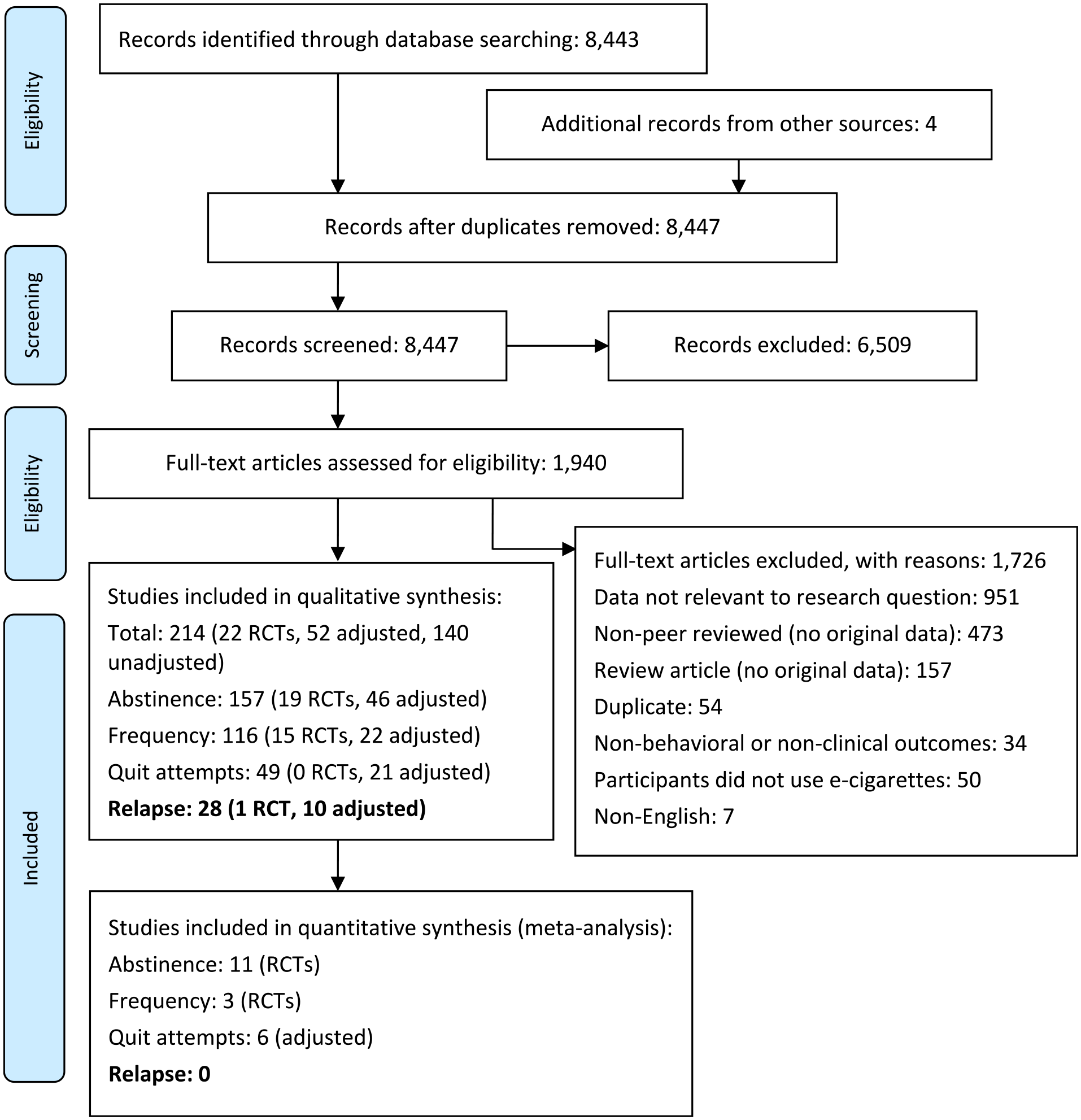
PRISMA flowchart when examining the potential associations between e-cigarette use among cigarette smokers and changes in continued cigarette smoking.
Of the 214 studies that were eligible for inclusion in the larger systematic review, 28 studies reported outcomes related to relapse to smoking cigarettes. Among these 28 eligible studies, one study was an RCT, 21 and 10 were observational studies18-20,22-28 that adjusted for gender, age, and race/ethnicity between groups (ie, adjusted for key demographic characteristics). These 10 studies were included in the qualitative synthesis of evidence. Studies that did not report demographically adjusted data are not included in the qualitative review but summary tables are provided in Supplemental Sections 11-14.
For each included study, information regarding the study characteristics (Supplemental Section 11), demographic and baseline characteristics (Supplemental Section 12), and study outcomes (Supplemental Section 13) were extracted. Although a quantitative synthesis was sought, the included studies were not adequate or compatible with the conducting of a meta-analysis. Complete details on the assessment of studies for inclusion in a meta-analysis—to include reasons for incompatibility among studies—are provided in Supplemental Section 14.
Of the 11 studies eligible for the qualitative synthesis of evidence, 2 studies were published in 201827,28, three in 201918,24,26, three in 2020,19,20,22 and three in 2022.21,23,25 Only one RCT was identified. 21 The remaining 10 studies were longitudinal in design.18-20,22-28 Ten studies were conducted in the US.18-20,22-28 Eight studies identified their study populations as “adults” (≥18 years old)18-20,22-24,26,27, one study included participants 18 to 29 years old, 25 while another study included participants 12 years and older. 28 One study did not define their study populations by age, but instead sampled participants who were attending stop smoking services. 21
Although RCTs were considered the highest level of evidence, only one RCT was identified and subsequently adjusted studies were included in the qualitative review. In addition to the demographic characteristics specified, most studies included further adjustments with varying combinations of other micro, meso, and macro covariates (eg, the presence of a tobacco user at home, highest parental education, and exposure to tobacco advertisements).
The reliability and validity of the relevant outcome measure—relapse to smoking cigarettes—was evaluated (as a contextual question, with a comprehensive but not systematic review of the literature) to provide fuller context for the interpretation of the synthesis of evidence. This measure was a single-item measure related to changes in cigarette smoking. Empirical data regarding the reliability and/or validity of this outcome measure was lacking, and therefore qualified as “inconclusive.” Further details, including a CQ evidence table of reliability and validity data identified for relapse to smoking cigarettes (Supplemental Section 5).
Two investigators appraised the included studies for quality according to the Downs and Black checklist. 17 Five studies (45%) were rated “good,”18,21,26-28 and six (55%) were rated “fair”19,20,22-25 (Supplemental Section 6). Although publication bias can be assessed using funnel plots, the absence of meta-analyses precluded such an assessment.
Definitions of E-Cigarette Use by Outcome Measure
Among the 11 included studies that examined relapse to cigarette smoking, 3 studies evaluated the association between regular e-cigarette use and relapse to cigarette smoking21,24,27, six studies evaluated non-regular e-cigarette use and relapse to cigarette smoking,19,20,23,25,26,28 and two studies evaluated the association between both regular and non-regular e-cigarette use and relapse to cigarette smoking.18,22
Of the 5 studies that evaluated the association between regular e-cigarette use and relapse to smoking, one study was an RCT in which e-cigarettes were administered to current-established cigarette smokers as part of the intervention. 21 These participants were considered to be regular e-cigarette users in terms of outcomes reported within the defined timeframes of the study. Three22,27,29 of the remaining 4 studies that evaluated regular e-cigarette use applied daily and nondaily use as the definition of regular e-cigarette use, reported as separate categories of users. In the remaining study, 18 regular use was defined as daily or nondaily use as a single category.
Of the 8 studies that evaluated the association between non-regular e-cigarette use and relapse to smoking cigarettes, the following definitions of non-regular use were applied: current or past 30-day use in 4 studies,18,19,25,26 ever use in 3 studies,25,26,28 use as a cessation aid in one study, 23 former use in 2 studies,18,25 past 12-month use in one study, 20 and experimental use or first-time use in one study. 22
Qualitative Synthesis of Available Evidence
Results of the qualitative analysis were stratified by regular versus non-regular e-cigarette use. Although RCTs were considered the highest level of evidence, only one relevant RCT was identified; consequently, the qualitative synthesis included studies that controlled for 3 key demographic variables (age, gender, and race/ethnicity).
Tables providing data from RCTs, adjusted and unadjusted studies of relapse to cigarette smoking are provided in Supplemental Section 13.
Relapse to cigarette smoking (regular e-cigarette use)
This systematic review identified one RCT 21 and 4 adjusted studies18,22,24,27 that investigated the association of regular e-cigarette use and relapse to cigarette smoking among regular e-cigarette users. Summary characteristics of these studies are provided in Table 1.
Summary Characteristics of RCTs and Adjusted Studies for Relapse to Smoking Cigarettes Among Regular E-Cigarette Users.

e-cig = electronic cigarette; smokers/smoking = cigarette smokers/cigarette smoking.
In a pragmatic RCT by Tattan-Birch et al. 21 cigarette smokers who were trying to quit were recruited to participate in a 12-week behavioral smoking cessation support program and were randomized to receive either a nicotine e-cigarette starter kit plus varenicline, or varenicline alone. At the follow up between Weeks 9 and 12 post-quit date, the rate of relapse to smoking cigarettes after continuous abstinence was 43% lower in the e-cigarette plus varenicline group compared to varenicline only group (hazard ratio [HR] = 0.57, 95% CI: 0.34-0.96). Adherence to varenicline treatment was similar between the 2 groups, with 22.9% of those in the e-cigarette plus varenicline group and 22.7% of those in the varenicline only group using varenicline daily for at least 8 weeks after quitting (risk ratio [RR] 1.02, 95% CI 0.47-2.20). In the e-cigarette plus varenicline group, 79.2% of participants used e-cigarettes daily for at least 1 week after their quit date, and 41.7% reported daily use at every session after quitting. Notably, there was also some contamination, with 20.5% of participants randomized to the varenicline only group using e-cigarettes daily for at least 1 week after the quit date, and 6.8% reported daily use at every session they attended. 21
In a longitudinal panel using data from the first 2 waves of the Population Assessment of Tobacco and Health (PATH) study in adult former cigarette smokers (18 years of age or older), Azagba et al. 22 defined regular e-cigarette use as either every day or someday use among established e-cigarette users (those who had ever used “fairly regularly”). Someday e-cigarette use (odds ratio [OR] = 4.78, 95% CI: 2.13-10.72; p < 0.05) was significantly associated with a higher odds of relapse to someday cigarette smoking compared to e-cigarette non-users; however, daily e-cigarette use (OR = 1.73, 95% CI: 0.84-3.57; p = NS) was not significantly associated with relapse to someday cigarette smoking. When assessing relapse to daily cigarette smoking, neither daily e-cigarette use (OR = 2.02, 95% CI: 0.98-4.62; p = NS) nor someday e-cigarette use (OR = 1.43, 95% CI: 0.35-5.89; p = NS) were significantly associated with relapse to daily cigarette smoking. 22
Similarly, using the first 2 waves of PATH, Dai and Leventhal 18 assessed relapse to cigarette smoking among former e-cigarette users, current occasional e-cigarette users, current regular e-cigarette users, and e-cigarette non-users. The authors categorized participants as “relapsers” if, at follow-up, they reported smoking cigarettes every day or some days. Among participants who had quit smoking cigarettes within the prior 12 months, the odds of relapse to cigarette smoking were not different between current regular e-cigarette users and e-cigarette non-users (AOR = 1.00, 95% CI: 0.57-1.75). This was also the case for prior and current occasional e-cigarette users (reported in detail in the results section for non-regular e-cigarette use). In contrast, in participants who had quit smoking cigarettes >12 months ago, current regular use of e-cigarettes was significantly associated with higher odds of relapse to cigarette smoking (AOR = 3.77, 95% CI: 1.48-9.65, p < 0.05). 18 This was consistent with findings in prior e-cigarette users, but not in current occasional e-cigarette users (reported in detail in the results section for non-regular e-cigarette use).
Using data from Waves 1 to 3 of the PATH survey, Kalkhoran et al. 24 reported that the odds of relapse to cigarette smoking did not differ between daily (AOR = 1.41, 95% CI: 0.76-2.61, p = NS) or nondaily (AOR = 1.07, 95% CI: 0.73-1.58, p = NS) e-cigarette users compared with e-cigarette non-users.
Verplaetse et al. 27 used Wave 1 to 2 data of the PATH study to assess relapse to cigarette smoking among daily and non-daily e-cigarette users compared with e-cigarette non-users. Among male participants, both daily (AOR = 2.96, 95% CI: 1.49-5.86, p = 0.002) and non-daily (AOR = 3.05, 95% CI: 1.29-7.17; p = 0.01) e-cigarette users had significantly higher odds of relapse to cigarette smoking compared with e-cigarette non-users. Conversely, among females, neither daily (AOR = 1.15, 95% CI: 0.57-2.29, p = 0.69) nor non-daily (AOR = 1.12, 95% CI: 0.49-2.60; p = 0.78) e-cigarette use was associated with relapse to cigarette smoking.
Relapse to smoking cigarettes (non-regular e-cigarette use)
Eight studies investigated the association of non-regular e-cigarette use and relapse to cigarette smoking.18-20,22,23,25,26,28 Summary characteristics of these studies are provided in Table 2.
Summary Characteristics of Adjusted Studies for Relapse to Smoking Cigarettes among Non-Regular E-Cigarette Users.

e-cig = electronic cigarette; EHR = electronic health record; NRT = nicotine replacement therapy; smokers/smoking = cigarette smokers/cigarette smoking.
In a longitudinal panel study using data from Waves 1 through 8 of the Marketing and Promotions across Colleges in Texas project (Project M-PACT) Loukas et al. 25 investigated the rate of relapse to cigarette smoking—defined as the transition from non-current cigarette smoking to current cigarette smoking—among ever cigarette smokers at baseline. In the adjusted model, probability of transitioning from non-current cigarette smoking to current cigarette smoking (ie, relapse) was higher among past 30-day e-cigarette users (adjusted hazard ratio [AHR] = 1.92, 95% CI: 1.50-2.45) and ever e-cigarette users (AHR = 1.14, 95% CI: 0.92-1.40) compared with never e-cigarette users. 25
In a longitudinal panel study using data from Waves 3 through 5 of the PATH study, Chen et al. 23 assessed the rate of relapse among participants who were cigarette smokers at Wave 3 and former cigarette smokers at Wave 4. At Wave 5, the rate of relapse was higher among those who reported having used e-cigarettes to quit smoking cigarettes compared to those who did not use e-cigarettes to quit (adjusted risk difference [ARD] = 9.4%, 95% CI: −5.0% to 22.8%). 23
In addition to applying measures of regular e-cigarette use described previously, Azagba et al. 22 also applied a non-regular definition of experimental e-cigarette use. Consistent with findings from their analysis of someday e-cigarette use, the odds of relapse to someday cigarette smoking were significantly higher among experimental e-cigarette users compared with e-cigarette non-users (OR = 5.43, 95% CI: 2.25-13.10; p < 0.05). However, experimental e-cigarette use was not significantly associated with relapse to daily cigarette smoking (OR = 1.76, 95% CI: 0.44-7.04; p=NS). 22
Using the first 3 waves of PATH data, Edwards et al. 19 reported that former established cigarette smokers who were current e-cigarette users were significantly more likely to relapse to cigarette smoking compared with e-cigarette non-users (AOR = 1.5, 95% CI: 1.1-2.1; p < 0.05). However, when the analysis was restricted to recent former established cigarette smokers (ie, those who had quit in the past 12 months), there was no significant association between current e-cigarette use and relapse to cigarette smoking (AOR = 1.1, 95% CI: 0.7-1.6, p=NS). 19
Using the first 4 waves of PATH data, Everard et al. 20 evaluated relapse to current daily or someday cigarette smoking among recent (ie, those who had quit in the past year) or long-term (ie, those who had quit more than a year ago) former established cigarette smokers. The authors found consistently significant associations between past-year e-cigarette use and relapse to cigarette smoking among all former established cigarette smokers (AHR = 2.98, 95% CI: 1.93-4.60; p < 0.05), recent former established cigarette smokers (AHR = 1.63, 95% CI: 1.04-2.53; p < 0.05), and long-term former established cigarette smokers (AHR = 3.79, 95% CI: 1.75-8.20; p < 0.05). 20
Using data from the first 2 waves of the PATH study, Dai and Leventhal 18 showed that among participants who had quit smoking cigarettes within the prior 12 months, the odds of relapse to cigarette smoking—defined as smoking cigarettes daily or on some days at follow-up—were not different between either former (AOR = 1.34, 95% CI: 0.78-2.29) or current occasional (AOR = 1.92, 95% CI: 0.84-4.40) e-cigarette users compared with e-cigarette non-users. These results were consistent with findings among regular e-cigarette users (reported in detail in the results section for regular e-cigarette use). In contrast, among participants who had quit smoking cigarettes >12 months ago, prior use of e-cigarettes was significantly associated with higher odds of subsequent relapse to smoking cigarettes compared with no e-cigarette use (AOR = 2.00, 95% CI: 1.25-3.20, p < 0.05), consistent with the findings in current regular e-cigarette users (reported in detail in the results section for regular e-cigarette use). However, current occasional e-cigarette use was not associated with higher odds of subsequent relapse to smoking cigarettes (AOR = 1.56, 95% CI: 0.34-7.14). 18
McMillen et al. 26 also used data from Waves 1 and 2 of the PATH study to evaluate relapse to cigarette smoking among participants who had quit cigarette smoking 5 or more years before the baseline survey. Ever e-cigarette users had significantly higher odds of relapse to cigarette smoking at follow-up—defined as having smoked cigarettes even one or 2 puffs—compared with e-cigarette non-users (AOR = 3.3, 95% CI: 1.6-6.7, p < 0.05). 26
Finally, one retrospective cohort study by Young-Wolff et al. 28 found that e-cigarette users were significantly more likely to relapse to cigarette smoking than non-e-cigarette users. Using data from electronic health records—participants matched for age, sex, race/ethnicity, and smoking status in the same month and year as the first documented ENDS use—the authors reported that e-cigarette users (participants with at least one “e-cigarette user” entry in their records) had significantly greater odds of relapse at 12 months compared with non-e-cigarette users (AOR = 2.35, 95% CI: 1.95-2.85); when further adjusting for median household income, psychiatric/substance use disorder diagnoses, use of tobacco cessation medication, and time since quitting cigarette smoking, the result remained significant (AOR = 1.53, 95% CI: 1.22-1.92). 28
Strength of Evidence
The overall SOE among the adjusted data regarding the association between e-cigarette use and relapse to smoking cigarettes were graded “moderate.” The SOE domain score table and the SOE and CQ ratings summary table for RCTs, adjusted and unadjusted data are presented in Supplemental Section 10.
Discussion
The current literature review identified a number of “good” quality studies (according to the Downs and Black quality metrics 17 ) that evaluated the association between e-cigarette use among cigarette smokers and relapse to smoking cigarettes. Although RCTs were considered as highest level of evidence, only one RCT was identified and therefore, studies that controlled for age, gender, and race/ethnicity (ie, studies reporting adjusted results at a higher level of evidence than the unadjusted results) were also included in the qualitative synthesis of evidence.
The RCT by Tattan-Birch et al. 21 found that the rate of relapse to smoking cigarettes after continuous abstinence was lower among participants randomized to use e-cigarettes and varenicline compared with those randomized to use varenicline alone. However, the authors reported that 20.5% of participants in the varenicline only group also used e-cigarettes for at least 1 week after the quit date, and 6.8% used them daily at every session. 21
Of the 10 adjusted studies that investigated the association of e-cigarette use and relapse to cigarette smoking, 4 applied definitions of regular e-cigarette use. Azagba et al. 22 found that experimental and someday e-cigarette users were significantly more likely to relapse to someday cigarette smoking; however, daily e-cigarette users were not. Moreover, when defining relapse in terms of daily cigarette smoking, neither experimental, someday, nor daily e-cigarette use was significantly associated with relapse. Stratifying their results by regular and non-regular measures of e-cigarette use, Dai and Leventhal 18 found no significant difference in the odds of relapse among current regular, current occasional, and prior (non-current ever) e-cigarette users when compared with non-e-cigarette users, in a sample of former cigarette smokers who had quit in the previous 12 months. By contrast, among former cigarette smokers who had quit smoking >12 months ago, current regular use and prior use of e-cigarettes were both significantly associated with higher odds of relapse to smoking cigarettes compared with no e-cigarette use; current occasional e-cigarette use was not associated with higher odds of subsequent relapse to smoking cigarettes. Verplaetse et al. 27 stratified their study results according to regular and non-regular e-cigarette use, as well as by gender. The study found significantly higher odds of relapse associated with both daily and non-daily e-cigarette use in men, but not in daily or non-daily e-cigarette use in women. 27 In addition, Kalkhoran et al. 24 found no difference in the odds of relapse among daily and never e-cigarette users or between non-daily and never e-cigarette users.
Among the remaining studies evaluating relapse to cigarette smoking—all of which applied non-regular measures of e-cigarette use—e-cigarette use was generally found to be significantly associated with relapse to smoking cigarettes. An analysis of recent former cigarette smokers by Edwards et al. 19 found no significant association between current e-cigarette use and relapse to smoking cigarettes, however, the same study found a significant association among all former cigarette smokers and relapse to smoking cigarettes. Everard et al 20 found relapse to smoking cigarettes to be significantly associated with past-year e-cigarette use among both recent and long-term former cigarette smokers, as well as former cigarette smokers in general. McMillen et al. 26 found that among former smokers who had quit smoking cigarettes 5 or more years ago both ever and past-30-day e-cigarette use were significantly associated with relapsing to cigarette smoking at follow-up compared with no e-cigarette use. Young-Wolff et al. 28 found that e-cigarette users were significantly more likely to relapse to cigarette smoking than non-e-cigarette users at 12 months follow-up. Finally, Chen et al. 23 reported that the rate of relapse at was higher among those who reported having used e-cigarettes to quit cigarette smoking compared to those who did not use e-cigarettes to quit. 23
The current systematic review exhibited 3 major strengths. First, its comprehensive search methodology, which yielded a large number of available studies for review. Second, the current review had a clearly defined PICOS, which assured the identification of the strongest evidence relevant to the research question. Third, guidelines for this review ensured that demographically-adjusted studies were included in the qualitative syntheses. Consequently, this systematic review provides a thorough and methodologically sound synthesis of the literature regarding the research the potential association between e-cigarette use among cigarette smokers and relapse to cigarette smoking.
In spite of these strengths, a number of limitations in the evidence base considerably restrict the interpretation of the findings. First only one RCT reported data on relapse to smoking cigarettes, and few studies reported demographically-adjusted results—only 10 of the 28 identified studies. Such a paucity of results from RCTs or from studies controlling for key demographic variables restricted the evidence pool considerably, thereby limiting the interpretation of findings in the qualitative synthesis. Additionally, eight18-20,22-24,26,27 of the 10 adjusted studies used PATH data from Waves 1 to 4 and therefore had potentially overlapping analytic samples. Moreover, the definition of e-cigarette use was not restricted to regular use; doing so would have provided the strongest evidence on potential associations with relapse to smoking cigarettes. Instead, the review was broadened to include any measure of e-cigarette use, with most studies measuring ever or current (past-30-day) use and applying definitions of cigarette use that were more consistent with temporary experimentation than regular use. Although results were stratified by regular versus non-regular e-cigarette use, only 4 adjusted studies were found which applied definitions of regular e-cigarette use. Given this small number of studies, conclusions are limited, and a need for future studies to apply definitions of e-cigarette use that identify regular established users is warranted. Variations in the definitions of both former cigarette smoking (ie, participants and baseline) and outcome measures further impede the conclusions that can be drawn. Other limitations include inadequate follow-up or measurement periods and the variation in the type of e-cigarettes used, in terms of design, nicotine concentration, flavor, and device generation.
Conclusions
In conclusion, more robust studies are required to determine an association between e-cigarette use and relapse to smoking cigarettes. Based on findings from this review, the available studies do not sufficiently measure e-cigarette use in a manner consistent with regular, established use, do not consistently define relapse in terms of a return to regular cigarette smoking, and do not sufficiently account for known or suspected confounding variables to support robust determinations related to e-cigarette use and cigarette smoking behaviors.
Supplemental Material
sj-docx-1-inq-10.1177_00469580231214457 – Supplemental material for A Systematic Review Investigating Associations Between E-Cigarette Use Among Former Cigarette Smokers and Relapse to Smoking Cigarettes
Supplemental material, sj-docx-1-inq-10.1177_00469580231214457 for A Systematic Review Investigating Associations Between E-Cigarette Use Among Former Cigarette Smokers and Relapse to Smoking Cigarettes by Mimi M. Kim, Isabella Steffensen, Red Thaddeus D. Miguel, Tanja Babic and Julien Carlone in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors would like to acknowledge Thera-Business (Ontario CANADA) for providing their systematic review expertise to all study activities across all levels of the updated review process. The authors would also like to thank Dr. Geoffrey Curtin, a retired employee of RAI Services Company, for his scientific contributions during the conceptualization of this review.
Authors’ Contributions
MMK conceived the study. MMK, IS, RDM, TB, and JC collected and analyzed project data. MMK, IS, and RDM defined the study design, selection of measures, interpretation of data, and co-wrote the manuscript. All authors have read and approved the final article. The corresponding author attests that the listed authors meet authorship criteria and that no others meeting the criteria have been omitted.
Availability of Data and Materials
All data and materials considered in this review are publicly available.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Kim is a former full-time employee of RAI Services Company, a wholly owned subsidiary of Reynolds American Inc.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All study activities were executed by providers external to RAI Services Company (Thera-Business), who were financially compensated for services according to contractual terms with RAI Services Company. RAI Services Company is a wholly owned subsidiary of Reynolds American Inc., whose operating companies manufacture and market tobacco products. The conception, analysis, and writing for this manuscript was a collaboration between Thera-Business and RAI Services Company.
Ethics Statement
Ethical approval for this study was not required.
Consent for Publication
Not required for this publication as no individual or identifiable information is considered.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.