
Abstract
The increase in hip fractures (HF) due to aging of the population and the rise in attractiveness of services provided at home following the COVID-19 pandemic, emphasize the need to compare outcomes of home versus hospital HF rehabilitation. To date, studies comparing the 2 services have focused primarily on clinical outcomes rather than patient-reported outcomes (PROs). This longitudinal observational study evaluated PROs of older adults with HF in the 2 settings. The SF36 questionnaire was used to measure PROs 3 times after surgery. The first PRO was retrospective and reflected pre-fracture health status. Descriptive statistics and mixed-effect logistic regression were used. Of 86 patients participating in the study, 41 had home rehabilitation and 45 had hospital rehabilitation. In both groups, the mental and physical scores plummeted 2 weeks after the HF, compared to pre-fracture status. The difference in improvement from pre-fracture status to recovery in both groups, were not significantly (P < .05) different, except for the pain domain. PROs of home versus hospital rehabilitation were similar, suggesting that rehabilitation at home can be as effective as hospital rehabilitation for suitable patients. This knowledge can improve quality of care in an aging global population.
Keywords
Following the COVID-19 pandemic, the percentage of patients with hip fractures discharged to continue rehabilitation at home has increased. Studies comparing home-based and hospital-based rehabilitation have focused on clinical outcomes rather than patient-reported outcomes (PROs). PROs can broaden our understanding of patients’ experiences and outcomes throughout the recovery process.
Patient-reported outcomes of home versus hospital-based rehabilitation were similar, suggesting that home rehabilitation is as effective as hospital-based rehabilitation.
The findings from this study can help medical staff in deciding rehabilitation plans for patients with hip fractures and support policy planning regarding the preparedness for the growing need for rehabilitation units.
Introduction
Hospitalization rates of patients with hip fractures (HF) have increased substantially in the past decade. 1 HFs in older adults are related with poor outcomes, high costs and a lengthy rehabilitation process.2,3 Rehabilitation following HF has been designed to reduce the effect of the fracture on long-term disability, 4 decrease the risk of mortality 5 and improve patients’ quality of life. 6 Most of the improvement occurs during the first 3 months after the fracture. 7
Rehabilitation can be achieved in a hospital or at home. 8 The decision of where the patient will undergo rehabilitation is dependent on social, medical, and cognitive determinants. HF patients are typically referred for home rehabilitation if they have a caregiver at home, do not require close medical attention, and/or are permitted to ambulate. 9
Multidisciplinary comprehensive rehabilitative care has been reported to have a positive outcome on patients recovering from HF.10,11 This treatment includes healthcare delivery by multiple health professionals such as nurses, physicians, physiotherapists, occupational therapists, social workers, and dietitians. In Israel, post-HF rehabilitation is multidisciplinary and cost-free in both settings. 9
Rehabilitation in both settings has its objective advantages and disadvantages. Hospitalization of older adults with HF has been associated with an increased risk of infections 12 and cognitive and functional deterioration.13,14 In contrast, home care has been designed to reduce iatrogenic complications and hospitalization-related expenses, and to honor patients’ wishes to stay at home. 15 However, rehabilitation at home may result in less medical attention and a greater burden on family caregivers.16 -18
Due to the aging of the population, in the past decade there is a growing need for rehabilitation together with an increase in home rehabilitation. 19 This change became increasingly evident when the COVID-19 pandemic caused older adults to fear leaving their homes for treatment in medical facilities due to the risk of infection. 20 Outcome comparisons of the 2 settings can help healthcare professionals recommend the best-suited rehabilitation location for patients with HF and support policy planning by improving the preparedness for the growing need for rehabilitation units. 15
Previous studies that compared home versus hospital settings primarily focused on clinical and functional outcomes21,22 but not on quality-of-life outcomes that are meaningful to the patient. Empathy and compassion have been proven to influence outcomes, 23 therefore in recent years, the use of patient-reported outcomes (PROs) in healthcare has increased.24,25 PROs are measured using validated questionnaires that assess the symptoms, function, and quality of life from the patient’s perspective. Therefore, the need to measure patient-valued outcomes is warranted. 26 The aging global population and predictable increase in the incidence of HFs emphasize the need to establish outcome sets that would be most meaningful to patients. This study sought to evaluate PROs of patients with HF in home-based and hospital-based rehabilitation.
Methods
Study Design
This longitudinal observational multi-center study of patients with HF was designed based on the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 27
Study-setting
Study participants were recruited from the 2 largest tertiary medical centers in the Middle East, during the period from December 2021 to November 2022.
Participants
Inclusion criteria were patients who (a) were age 60 years and older; (b) had undergone HF stabilization: anatomical femoral neck fractures and per-trochanteric; (c) were able to understand and sign the informed-consent form; (d) understand Hebrew. Exclusion criteria were patients with (a) pathological fractures; (b) severe hearing disabilities.
The study participants were divided into 2 groups. Group one included patients after surgery who were discharged from the Department of Orthopedics to their homes and received a visit from a member of the at-home rehabilitation team within 24 to 48 h. Group two included patients after surgery who were admitted to the Rehabilitation Department directly from the Department of Orthopedics. It is important to note that the patients were allocated to a specific group at the discretion of the medical team but not for the purpose of research. Each patient’s rehabilitation setting was decided based on meetings between the clinical team—including the social worker, nurse, and physicians—and the patient with his/her family. The medical team’s criteria for placement and discharge plan were based on the patient’s comorbidities cognitive status, and social support. For example, patients with no social support and/or severe comorbidities such as kidney disease that required dialysis remained in-hospital for their rehabilitation.
Rehabilitation therapy in both settings were similar and included an integrative treatment approach carried out by a multidisciplinary staff. The rehabilitation regimen in the hospital included daily (7 days/week) visits and care by nurses and geriatricians; physiotherapy and occupational therapy on every weekday (5 days/week); at least 2 meetings with the social worker; at least one dietitian consultation; and upon request, consultations with orthopedic and rehabilitation specialists as well as a psychologist and speech therapist. The home rehabilitation regimen included daily (7 days/week) on-call geriatrician and nursing care supervision; physiotherapy and occupational therapy 2 or 3 times per week; at least 1 meeting with a social worker; and upon request, consultations with dietitians, orthopedic and rehabilitation specialists as well as a psychologist and speech therapist.
Data Collection
At baseline, demographic and clinical data including co-morbidities, functional status prior to fracture, and social support, were collected from patients’ hospital and community medical files.
Outcome Measurements
PROs were measured using the short form (SF)-36 questionnaire. Although the SF36 is a general questionnaire that addresses specific conditions,28,29 it is suitable for measuring PROs in patients with HF 30 and evaluating recovery after lower extremity trauma. 31 The questionnaire consists of 36 questions that address 8 topics: physical functioning, physical role limitation, general health, bodily pain, vitality, social functioning, emotional role limitation, and mental health. Results are interpreted by calculating scores for each topic and summarizing scores of several topics to generate a physical component score (PCS) and mental component score (MCS).32,33
Measurements were performed 3 times: 24 to 48 h after surgery while the patient was still hospitalized (T1), 2 weeks post-surgery (T2) while hospitalized or by phone, and 3 months later by phone (T3) (See Figure 1 for timeline). The first time point involved a retrospective assessment and reflected health quality and functionality prior to the fracture. 34

Timeline for SF36 PRO questioning.
Statistical Measures
Descriptive statistics were used to outline the patient’s demographics and medical history. t-Test and Chi-Square were used to detect differences in the characteristics of the groups. SF36 data were scaled; therefore, possible scores ranged from 0 (poor health) to 100 (excellent health) for the 8 domains. Additionally, PCS and MCS that have been reported as responsive in orthopedic conditions, 35 were calculated. The calculations were performed according to the RAND Corporation website (36-Item Short Form Survey (SF-36) | RAND) and the oblique (correlated) factor solution that is recommended for orthopedic patients. 36
Mixed effect logistic regression was used to compare PROs. The mean scores were adjusted for age, sex, and Charlson et al 37 co-morbidity index (CCI), which is a predictive score of health outcomes in patients with HF.3,38 The PROs were not adjusted for fracture and surgery type, as others have reported no association between health-related quality of life and surgical approach.39 -41 The minimal important difference (MCID) was calculated, assuming that changes of 9 points in one of the subscale scores and 2 points in the PCS and MCS of the SF36 are considered as the MCID.42,43 MCID was compared between the 2 groups and among assessment time points: pre-fracture versus 2 weeks after (T1-T2), 2 weeks versus 3 months after fracture (T2-T3), and pre-fracture versus 3 months post-fracture (T1-T3).
The data were managed with Excel 2016 and analyzed using IBM SPSS Statistics for Windows Version 27 and Stata version 15.0.
Sample Size
The sample size was determined using Winpepi 11.65. We considered a change of 9 points in one of the subscales of the SF36 to be the MCID. 42 To detect a difference of 9 points on the subscale, assuming a standard deviation of 10 points and a power of 80% and P < .05, a sample size of 20 participants in each group was required. Accounting for possible attrition due to the unfortunate increased risk for deterioration and mortality following HF, 44 we set a goal to increase the sample size of each group by at least 50%, that is a minimum of 30 participants in each subgroup.
Ethics Approval and Consent of Participation
The study was approved by the ethics committees of the 2 hospitals (#SMC-7933-20, and #HMO-0691-21). All participants provided written informed consent before enrolling in the study.
Results
Characteristics of Participants
A total of 86 HF patients participated in the study; 45 patients underwent rehabilitation in the hospital and 41 at home (see Figure 2 for the description of study participants’ groups and follow-up at 2 weeks and 3 months). The 2 groups had similar characteristics (P > .05) (see Table 1) with the exception of age and CCI. No significant differences (P > .05) were found in demographic, clinical, and social characteristics between study participants and patients excluded from the study (n = 141) for self-reported reasons, such as health issues, hearing difficulties, and language barriers.
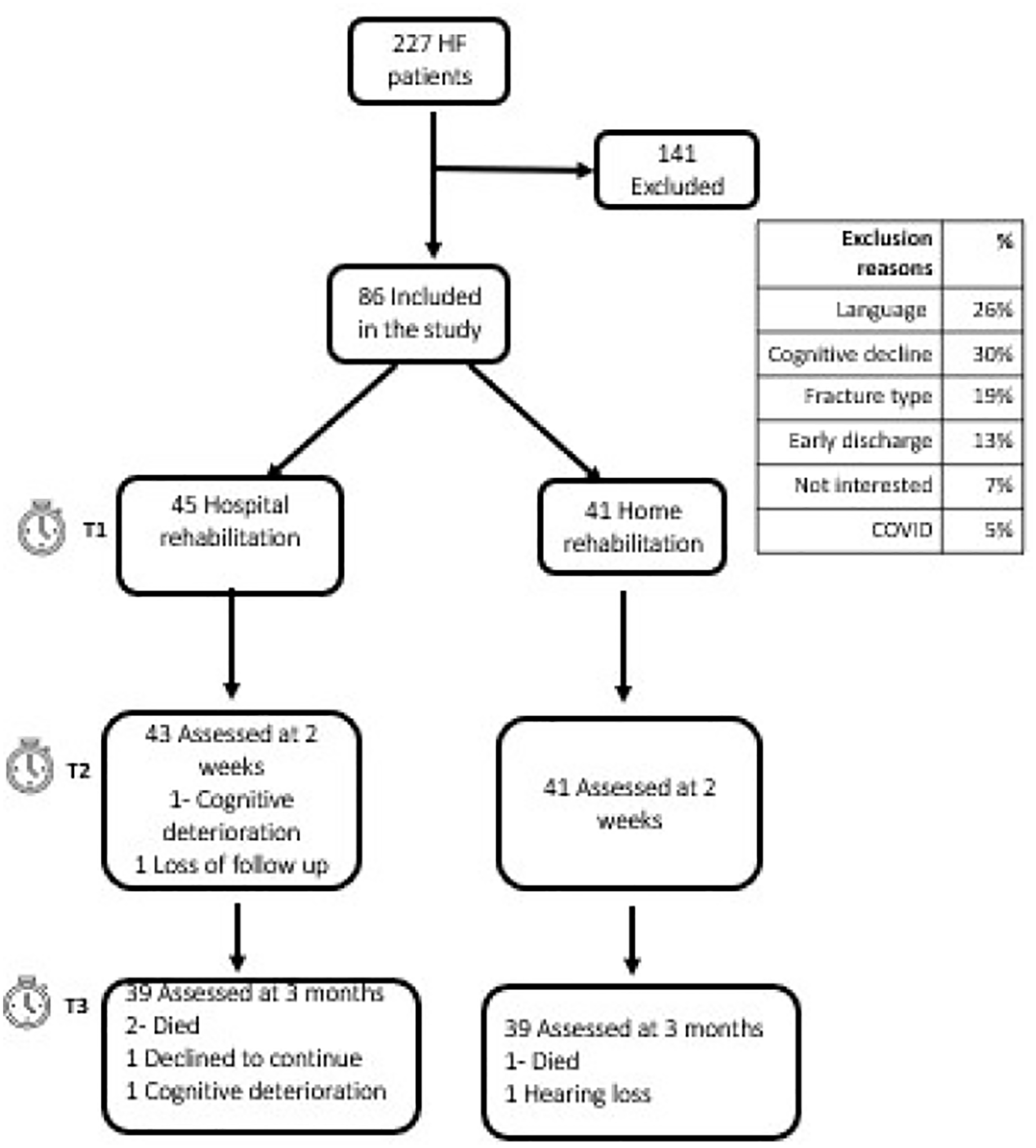
Description of study participants’ groups and follow up 2 weeks and 3 months later.
Comparison of Characteristics Between the Hospital and Home Rehabilitation Groups.

Note. SD = standard deviation.
PROs
Response rates were 100%, 98%, and 91% at T1, T2, and T3, respectively. The 2 groups had similar declines in most SF36 health scores 2 weeks post after fractures. Figure 3 presents the physical and mental summary scores, adjusted for age, sex, and CCI, of the participants in the home and hospital groups. No significant differences in the scores (P < .05) were observed when comparing the PROs scores between both the groups at pre-fracture (T1), 2 weeks post fracture (T2), and 3 months later (T3). In both groups, the mental and physical scores plummeted 2 weeks after HF (T2), in comparison to the pre-fracture status (T1). Table 2 describes this by presenting the differences (delta) in scores at the 3 timepoints. For example, in the home rehabilitation group physical function declined between the pre-fracture measurement (T1) and the post-fracture measurement (T2) by 61.34 points, however it improved by 34.38 points between the T2 measurement and the measurement 3 months post fracture (T3). However, the T3 measurement did not return to its pre-fracture (T1) value, and was lower by 26.92 points. This deterioration was MCID in all health domains and in the 2 summary domains, PCS and MCS. The patients’ health status improved 3 months after HF (T3). This difference was MCID primarily for the physical health domains (PCS, physical function, and pain) and MCS.

Comparison of PROs scores in hospital and home rehabilitation groups, at T1, T2, T3, adjusted to sex, age, and CCI.
Comparison of the Difference in PRO Scores Between Time Points (T1-T2, T2-T3, T1-T3) in the Hospital and Home Groups Adjusted for Sex, Age, and CCI.

Note. PF = physical functioning; RL = physical role limitation; BP = bodily pain; GH = general health; V = vitality; SF = social functioning; EL = emotional role limitation; MH = mental health; PCS = physical component score; MCS = mental component score.
Bold= Values in a row that differ statistically (P < .05) when compared between the home and hospital groups, at the 5% probability level according to the multi-analysis regression.
With the exception of bodily pain, no significant (P < .05) differences were found in improvement from the pre-fracture status to the 3 months post-facture status in either group.
Discussion
The current findings suggested that the rehabilitation setting did not influence PROs. Therefore, the choice of rehabilitation setting can be based on other factors such as the patient’s medical and social condition, the patient’s and family’s/caregiver’s preference and the ability to provide homecare. For the pre-fracture evaluation, the hospital group had a lower SF36 score than did the home group. This was not surprising, since patients with more co-morbidities are typically referred for inpatient rehabilitation rather than home rehabilitation.45,46 For a more balanced comparison of both groups, the outcomes were controlled for age, sex, and CCI. However, although the preliminary SF36 score of the home rehabilitation group was higher than that of the inpatient group, the outcomes were mostly similar.
The findings from this study are compatible with findings from previous studies that compared clinical outcomes such as 30-day readmission rates, mortality rates during or within 90 days of rehabilitation, and functional improvement. No significant difference in these outcomes were observed between home-based and in-hospital rehabilitation.21,47 -50 In fact, patients undergoing home rehabilitation have been reported in previous studies to experience fewer adverse events 51 such as infections. 52 Home rehabilitation has also been found to have a positive effect in the early stages of rehabilitation, on patients’ balance confidence, 18 self-efficacy, 53 functionality, 54 time-space orientation, collaboration, 50 and even caregivers’ burden. 55 These suggest that patients with HF can be managed at home while achieving equivalent outcomes and using fewer resources than those patients managed in inpatient settings.56,57 This information is especially valuable in Israel due to the shortage of rehabilitation beds in long-term facilities. 58
PRO data provided a richer understanding of the outcomes, functionality, and well-being of patients with HF over time. As expected, patients’ physical and functional status were altered by the fracture. However, our findings suggested that HF affects general, emotional, and mental health and social functioning. A sharp decline in SF36 scores post-HF with only partial recovery after rehabilitation have been reported previously.40,41 Jaglala 59 reported that the same trend continued through to 6 months post-fracture.
Strengths and Limitations
The current study demonstrated several strengths that had not been reported previously. Others 15 have stressed the importance of conducting studies that compare the outcomes of home-based and hospital-based care post-HF, and indeed, the current study examined the PROs of patients post-HF undergoing home and hospital rehabilitation. In contrast, previous studies compared quality of life between patients with HF undergoing home rehabilitation and those undergoing no treatment at all,18,51,53,55,60 -62 or had small sample sizes.50,63 As such, we performed a more balanced comparison between the 2 rehabilitation settings. This study had relatively higher response rates (100%-91%) at T1, T2, and T3, in all age groups than other HF PRO studies (54%-15%), which reported a lack of representation of older adults.64 -66 The high response rates could be due to the use of a single questionnaire that reduced survey fatigue 67 and the use of sequential methods, in-person and phone-based assessment, both of which have been associated with higher survey response rates. 68 Unlike other studies, 39 we collected patient pre-fracture PROs and evaluated the effect of the HF on our study participants. The study was conducted in 2 large tertiary hospitals and the results can serve as a benchmark for the comparison of future PROs in patients with HF.
A possible limitation is that naturally, this study cannot evaluate whether patients who received rehabilitative care in-hospital would have had similar results had they been cared for at home and vice versa. Additionally, factors, such as socioeconomic status, may have influenced the referral of patients for home or hospital rehabilitation. Assessment at 3 months and part of the assessments at 2 weeks were performed by telephone interviews. Previous studies have reported that telephone-administered questionnaires usually result in a more optimistic health-related quality of life,69 -71 suggesting that the recovery of patients with HF may be worse than the reported outcomes described in the study. This study did not control for social support or pre-fracture self-perceived efficacy that have been reported to influence patient outcomes.72,73
The COVID-19 pandemic has had an effect on rehabilitation services, with increased use of home-based rehabilitation and tele-rehabilitation that were designed to ensure the safety of patients and their staff. 74 In keeping with this new reality, studying the outcomes and efficacy of HF rehabilitation in different settings is necessary. Findings from the current study can help with decisions on where to rehabilitate the patient and support policy planning regarding the development of future rehabilitation services. We suggest that future research further explore the differences in the 2 setting while using functional assessment tools such as the Lower Extremity Functional Scale 75 and the Short Physical Performance Battery. 76
Conclusion
PROs of hospital versus home rehabilitation were similar, suggesting that rehabilitation at home can be as effective as hospital rehabilitation. Using PROs for outcome assessment enables a deeper and more complete understanding of the different rehabilitation settings. Using this approach as part of national HF registries can improve quality of care and promote patient-centered care. Future studies are warranted to explore the use of PROs in other healthcare fields and in a randomized controlled trial setting.
Supplemental Material
sj-doc-1-inq-10.1177_00469580241230293 – Supplemental material for Home Versus Hospital Rehabilitation of Older Adults Following Hip Fracture Yields Similar Patient-Reported Outcome Measures
Supplemental material, sj-doc-1-inq-10.1177_00469580241230293 for Home Versus Hospital Rehabilitation of Older Adults Following Hip Fracture Yields Similar Patient-Reported Outcome Measures by Hanna S. Schroeder, Avi Israeli, Meir (Iri) Liebergall, Omer Or, Wiessam Abu Ahmed, Ora Paltiel, Dan Justo and Eyal Zimlichman in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We thank the patients and the medical caregivers from the Orthopedic and Rehabilitation departments in Hadassah medical center and Sheba medical center for the participating in the study. The views expressed do not necessarily represent those of the organizations in which the authors work or worked.
Author Contributions
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethic Committee
The study was approved by the ethics committees (#SMC-7933-20) and (#HMO-0691-21).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.