
Abstract
Pregnant women are at increased risk of influenza-related complications. However, the rate of influenza vaccination among pregnant women in Taiwan is low. By analyzing real-world data in this study, we investigated the factors associated with influenza vaccination during pregnancy in Taiwan. This study was a cross-sectional study. We collected real-world data from 2 databases in Taiwan: the Birth Certificate Database and the National Health Insurance Research Database. The study population was pregnant between October 2014 and December 2016 in Taiwan. The multivariate logistic regression was performed to identify factors associated with influenza vaccination, including maternal sociodemographics, trimester, comorbidities, and health-care utilization. The vaccination rate of among pregnant women was 8.2%. Factors significantly associated with a high likelihood of influenza vaccination were age between 30 and 34 years (odds ratio [OR]: 1.14; 95% confidence interval [CI]: 1.10-1.19), second trimester (OR: 1.80; 95% CI: 1.75-1.85), income equal to or exceeding NT$ 38 201 (OR: 1.92; 95% CI: 1.86-1.99), hypertension (OR: 1.16; 95% CI: 1.05-1.29), cardiovascular disease (OR: 1.29; 95% CI: 1.17-1.42), autoimmune disease (OR: 1.47; 95% CI: 1.38-1.58), and chronic pulmonary disease (OR: 1.24; 95% CI: 1.18-1.31). A low level of urbanization, at least 1 hospitalization in the previous year, and the presence of pregnancy complications (eg, gestational diabetes, preeclampsia, and placenta previa) were associated with a lower likelihood rate of influenza vaccination. The influenza vaccination rate among pregnant women in Taiwan was low. Age, gestational age, income level, urbanization level, hypertension, cardiovascular disease, autoimmune disease, chronic pulmonary disease, and pregnancy complications may be associated with influenza vaccination among pregnant women.
Pregnant women who receive an influenza vaccine protect themselves and also their unborn children, but the vaccination rate is still low.
Trimester, age, income level, urbanization level, health-care utilization, hypertension, cardiovascular disease, autoimmune disease, chronic pulmonary disease status, and pregnancy complications were associated with influenza vaccination in pregnant women.
The present study was based on a nationwide database which covers over 99.9% Taiwanese population. Our findings suggest a low vaccination rate among pregnant women and provide real-world evidence of associated factors for the government to promote influenza vaccination and increase the vaccination rates.
Introduction
Influenza (flu) is an infectious disease caused by influenza viruses. Globally, flu epidemics result in approximately 3 to 5 million cases of severe illness and approximately 290 000 to 650 000 respiratory deaths every year. 1 According to the estimation of the Taiwan Centers for Disease Control, which is based on secondary data (2011-2020) from the National Health Insurance Research Database (NHIRD) and data from the National Infection Disease Report System, approximately 12% to 14% of individuals in Taiwan visit a physician for pneumonia or flu every year; of them, 0.6% require hospitalization. Furthermore, among patients with a severe case of the flu, flu-related mortality is approximately 25%. 2 Flu prevention is an important public health goal.
Vaccination is the safest and most effective method for preventing flu.3 -5 Pregnant women are at particularly high risks of severe complications from the flu and should therefore be vaccinated against it. The US Advisory Committee on Immunization Practices and US Centers for Disease Control have stated that pregnant women can safely receive a flu vaccine at any point during pregnancy. 6
Pregnant women who receive a flu vaccine protect themselves and also their unborn children.7,8 The rate of flu vaccination among pregnant women in several countries is low. Flu vaccination rates were approximately 35.6% in the United States in 2017, 9 7.4% in France in 2016, 10 0.5% to 58.6% in European countries between 2016 and 2017, 11 and 4% and 59.6% in South Korea between 2006 and 2019. 12 The rate of flu vaccination is still substantially lower than the Healthy People 2020 target of 80% in most countries. 13
Since 2014, flu vaccines have been made free for pregnant women in Taiwan. Few studies have explored flu vaccination intention or behavior among pregnant women in Taiwan. To the best of our knowledge, no nationwide population-based study has been conducted on this topic. Therefore, in the present study, we analyzed data from a national database to investigate the rate of flu vaccination among pregnant women in Taiwan. We further explored factors influencing flu vaccination behaviors in this cohort. Our findings may help promote flu vaccination behaviors and increase vaccination rates among pregnant women.
Methods
Data Source
Data (2013-2016) were obtained from Taiwan’s NHIRD and Birth Certificate database. These databases are managed by the Health and Welfare Data Science Center of the Taiwanese Ministry of Health and Welfare. The NHIRD includes details of beneficiaries enrolled in the National Health Insurance program. Approximately 99% of all residents of Taiwan are enrolled in this insurance program. The NHIRD includes detailed clinical records related to outpatient department visits, hospitalizations, diagnostic codes, and prescriptions. The Birth Certificate database is a nationwide database of birth records that contains information about mothers, perinatal periods, and newborn characteristics. This database and the NHIRD exhibit high levels of information integrity and have been validated as powerful research databases for real-world evidence-based studies in Taiwan.14,15 For the present study, we used data from the aforementioned databases and investigated the factors influencing the rate of flu vaccination among pregnant women in Taiwan.
Ethics Approval
The database used to support the findings of this study was anonymized for privacy. The requirement for informed consent was waived. This study protocol was approved from a completely ethical review by an Institutional Review Board in central Taiwan.
Study Cohort
Women who were pregnant between October and December in 2014, 2015, or 2016 were retrospectively included in this study. These months were selected because the Taiwan government holds an annual flu vaccine campaign between October 1 and December 31, during which pregnant women can receive flu vaccines for free. Pregnant women aged <14 years or >50 years or with incomplete records were excluded from this study. The included pregnant women were divided into 3 subgroups on the basis of trimester determined according to the American College of Obstetricians and Gynecologists criteria. The first, second, and third trimesters encompassed a gestational age of <14 weeks, 14 to 28 weeks, and 29 to 40 weeks, respectively. We included 477 383 pregnant women; of them, 212 185 (44.45%), 100 079 (20.96%), and 165 119 (34.59%) women were in the first, second, and third trimesters, respectively.
Study Design
This was a population-based cross-sectional study. Diagnostic data in the NHIRD were coded as per the diagnostic codes outlined in the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) and International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM). The following factors were investigated: age, insured salary (income level), urbanization level, trimester, health-care utilization during the previous year, comorbidities, and pregnancy complications. Comorbidities considered in the present study (and their ICD-9-CM and ICD-10-CM codes) were as follows: asthma (493 and J45), hypertension (401-405, I10-I13, and I15), diabetes mellitus (250 and E10-E14), kidney disease (580-584, 586-588, N00-N08, N14, N17-N19, and N25-N26), cardiovascular disease (390-398, 410-414, 430-438, 440-444, 446, I00-I02, I20-I22, I24, I25, I60-I63, I65-I74, G45, G46, I77, I79, M30, and M31), autoimmune disease (040-044, A48-A49, B20, B95-B96, K90, and M60), and chronic lung disease (490-496, 500-508, 510, 514-519, J40-J47, J60-J66, J68-J70, J80-J82, J84, J86, J96, J98, J99, B44, and R91). The following pregnancy complications were assessed: gestational diabetes (648.00-648.04, 648.81, 648.83, 648.84, and O24), gestational hypertension (642.30-642.34 and O13), preeclampsia (646.10-646.14, 646.20-646.24, 646.80-646.83, 642.40-642.43, 642.50-642.54, O12, and O14), placenta praevia (641.0-641.1 and O44), and placental abruption (641.20-641.23, 641.30, 641.31, and O45).
Statistical Analysis
Data were analyzed using SAS (version 9.4; SAS Institute, Cary, NC, USA). Descriptive statistics were used to analyze cohort characteristics, health-care utilization, comorbidities, and pregnancy complications; the distributions, percentages, means, and standard deviations of the study cohort were determined. Multivariate logistic regression was performed to investigate the associations of various factors with the rate of flu vaccination. Data are presented in terms of odds ratio (OR) and the corresponding 95% confidence interval (CI) values. Statistical significance was set at P < .05.
Results
The baseline characteristics of the cohort are summarized in Table 1. The average age of the cohort was 31.84 ± 4.89 years. Regarding age groups, 9.19% of the pregnant women were aged <24 years, 23.46% were aged 25 to 29 years, 40.69% were aged 30 to 34 years, and 26.66% were aged 35 to 50 years. Regarding comorbidities, 13 777 women (2.89%) had asthma, 4373 (0.92%) had hypertension, 5119 (1.07%) had diabetes mellitus, 1574 (0.33%) had kidney disease, 4410 (0.92%) had cardiovascular disease, 8612 (1.80%) had autoimmune disease, and 30 302 (6.35%) had chronic lung disease. Regarding pregnancy complications, 10 949 women (2.29%) had gestational diabetes, 318 (0.07%) had gestational hypertension, 6765 (1.42%) had preeclampsia, 2466 (0.52%) had placenta praevia, and 815 (0.17%) had placental abruption.
Baseline Characteristics of Pregnant Women.

1NTD ≈ 0.33USD.
GDM = gestational diabetes mellitus; CVD = cardiovascular disease; HTN = hypertension; DM = diabetes mellitus.
The rate of flu vaccination and factors associated with this rate are presented in Table 2. A total of 39 146 women received a flu vaccine (vaccination rate, 8.20%). The vaccination rates for women in the first, second, and third trimesters were 6.44%, 11.00%, and 8.76%, respectively. The average age of women who received a flu vaccine was 32.20 ± 4.62 years. The rate of vaccination was 6.30% among women aged <24 years and 8.59% among women aged 35 to 50 years. This rate was 10.40% in women with an income equal to or exceeding NT$ 38 201. After covariate adjustment, the adjusted OR (aOR) for flu vaccination in women in the second trimester was 1.80 and that for flu vaccination in those in the third trimester was 1.32, compared with the findings in women in the first trimester. Compared with the aOR for women aged <24 years, those for women aged 25 to 29, 30 to 34, and 35 to 50 years were 1.12, 1.14, and 1.11, respectively. The aOR for flu vaccination was positively correlated with income level (P < .001). Regarding comorbidities, pregnant women with hypertension, cardiovascular disease, autoimmune disease, and chronic lung disease were more likely to have received a flu vaccine. Regarding pregnancy complications, pregnant women with gestational diabetes, preeclampsia, and placenta praevia were less likely to have received a flu vaccine. Furthermore, aOR was positively correlated with the number of outpatient visits (P < .001). Pregnant women who had been hospitalized in the previous year were less likely to have received a flu vaccine than were those who had not been hospitalized in the previous year.
Vaccination Rate and Risk Factors of Influenza Vaccination in Pregnant Women.
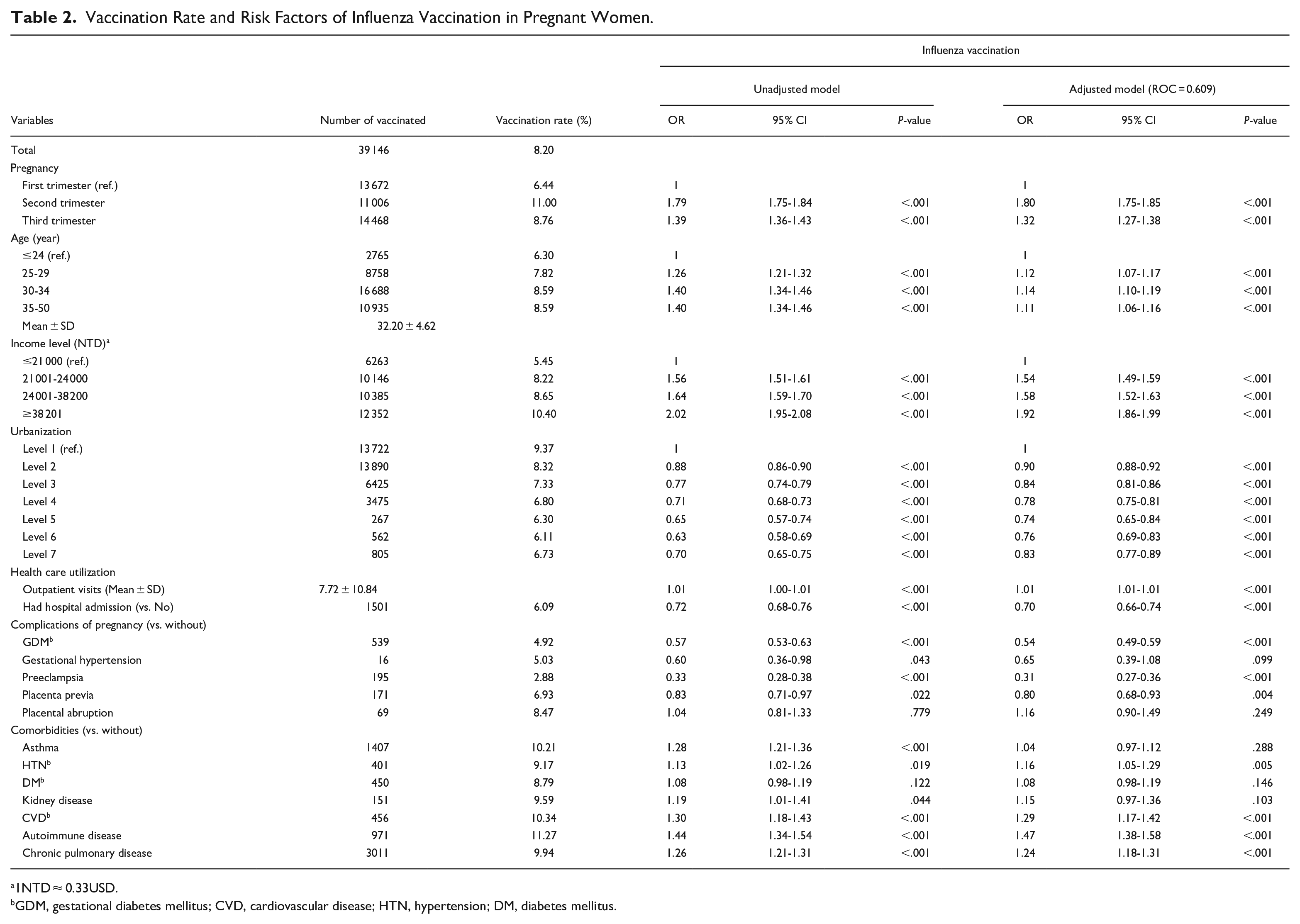
1NTD ≈ 0.33USD.
GDM, gestational diabetes mellitus; CVD, cardiovascular disease; HTN, hypertension; DM, diabetes mellitus.
Discussion
The rate of flu vaccination among pregnant women in Taiwan was 8.20% between 2014 and 2016. Factors associated with this rate were trimester, age, income level, urbanization level, health-care utilization, comorbidities, and pregnancy complications. Furthermore, this rate was found to be lower than that noted in other countries.9,11,12 Pregnant women in Taiwan were not eligible for free flu vaccinations before 2014. We analyzed relevant data corresponding to the first 3 years (2014-2016) after flu vaccines were made free for pregnant women in Taiwan. The lack of awareness regarding the free flu vaccination program might have contributed to the low rate of flu vaccination. Additional studies are warranted to investigate whether the free flu vaccination program influences the rate of vaccination among pregnant women.
The rate of flu vaccination among pregnant women was positively correlated with age. Various studies have reported that the rate of flu vaccination among older pregnant women was higher because these women had a better understanding of effective preconception health behaviors than did younger pregnant women.16 -22 Because pregnant women in Taiwan were eligible for free flu vaccinations during the study period, financial concerns might not have influenced vaccination behaviors; however, income level was positively correlated with vaccination rate, consistent with findings of other studies.18,19,23 Additionally, urbanization level was positively correlated with the rate of flu vaccination, consistent with the findings of another study. 24 This finding may be attributed to the fact that medical resources are abundant in urban areas, making flu vaccinations in these areas relatively convenient. Pregnant women were more likely to have received a flu vaccine if they had a comorbidity. A study reported that the OR for flu vaccination among individuals with health problems, such as asthma, heart disease, chronic liver disease, chronic kidney disease, chronic obstructive pulmonary disease, diabetes, and autoimmune disease, was 9.3 times higher than that for flu vaccination among healthy individuals. 25 Furthermore, pregnant women with preexisting diabetes, lung disease, kidney disease, or heart disease were more likely to have received a flu vaccine than those without these conditions. 26
However, pregnant women with pregnancy complications were less likely to have received a flu vaccine than were those without pregnancy complications; this finding is consistent with previous studies.25 -27 A prospective study explored factors influencing flu vaccination behaviors among pregnant women and reported that pregnant women with pregnancy complications (eg, placenta previa, preeclampsia, gestational hypertension, and gestational diabetes) were less likely to receive a flu vaccine than those without pregnancy complications. 23 Vaccination safety is the primary concern for pregnant women deciding whether to receive a flu vaccine.16,25 -27 Despite previous studies have confirmed that vaccination is the safest and most effective method for preventing flu,3 -5 concerns about serious vaccine-related side effects and underestimating the risks of severe adverse outcomes during pregnancy still contribute to vaccine hesitancy, in turn, leads to reluctance in getting vaccinated.28 -31 A cross-sectional multicenter study in Italy assessed pregnant women’s knowledge, beliefs, and misconceptions about vaccines. The study results showed that only 9% of women completely believed in the safety of vaccinations and almost 20% of women had misconceptions or lack of knowledge about flu vaccinations during pregnancy. 31 Another survey revealed that the influenza vaccine uptake among surveyed pregnant women was only 21.1%, despite 68.4% acknowledging strong evidence supporting the safety of vaccinations during pregnancy. The study found that those who expressed concerns about potential adverse events for the unborn child from vaccine received during pregnancy were significantly less willing to receive the influenza vaccine (OR = 0.76). 30 From the aforementioned literatures, it is evident that unrealistic perceptions of risk can be associated with barriers that might influence the decision to vaccinate. Therefore, training women to trust accurate healthcare professional information and advice is crucial for making informed choices and increasing vaccine uptake.28 -31
One of the important factors influencing the rate of flu vaccination among pregnant women was the recommendation from healthcare providers (HCPs). The number of outpatient clinic visits was positively correlated with the flu vaccination rate; this finding is consistent with those of other studies. A study reported that the frequency of contact with medical professionals was positively correlated with the rate of vaccination. 32 Offering flu vaccinations for free during antenatal visits increased the likelihood of receiving flu vaccinations. 33 HCPs’ recommendation was the factor that most strongly influenced the intention to receive a flu vaccination among pregnant women; this factor increased the intention to receive a flu vaccination and consequently the rate of vaccination among pregnant women.16,34 The rates of flu vaccination were 43% to 69% among pregnant women with a recommendation from HCPs and only 4% to 10% among those without HCPs’ recommendation. 18 Despite this, several recent survey studies have found that while the majority of HCPs understand the importance of pregnant women receiving a flu vaccination and recommend vaccination during pregnancy, there is still a significant proportion of HCPs lacking up-to-date and accurate knowledge.35 -37 They underestimate the risk of infection with vaccine-preventable diseases and overestimate the risks of vaccine side effects.29,35 -37 The influenza vaccine coverage rates for pregnant women in several countries are still less than ideal.9 -12 Therefore, continuous intervention through education and information is necessary and crucial to enhance HCPs’ understanding of the safety and effectiveness of vaccination for pregnant women, thereby further increasing vaccination rates.29,35 -37
In terms of pregnancy duration, An Italian study investigated attitudes toward flu vaccinations among pregnant women and revealed that pregnant women were more likely to receive flu vaccinations in the second and third trimesters than in the first trimester. 38 A South Korean study conducted through a questionnaire survey revealed that pregnant women were more likely to receive a flu vaccine during the third trimester than during the first trimester. 39 A Canadian study also revealed that pregnant women in the third trimester were more likely to be vaccinated against the flu. 40 The findings of the present study are consistent with those of other studies, which indicate that pregnant women are more likely to receive a flu vaccine during the second and third trimesters than during the first trimester. This behavior may be associated with the intention to protect newborns. Studies have indicated that compared with the first trimester, flu vaccination during the second and third trimesters is less dangerous for newborns.41,42
A strength of the present study lies in its population-based design implemented using a nationwide database. We included the entire Taiwanese population; therefore, the qualitative sample size was sufficiently large to ensure high statistical power and reduce selection bias.
The study also has several limitations. First, the study was a secondary data analysis based on the NHIRD which only contained the medical details coverage by the National Health Insurance Program in Taiwan. Thus, the information on self-paid medical care utilization is lacking in the present study. Although the Taiwan government provides free influenza vaccines for pregnant women from October to December each year, a small part of pregnant women may receive the flu vaccine by self-pay. Therefore, the influenza vaccination rate for pregnant women in this study may be underestimated. Second, various factors known to influence the flu vaccination behavior of pregnant women were not analyzed in the present study because of the unavailability of relevant data. These factors included marriage, educational level, religion, reproduction experience, lifestyle, and health behavior (eg, attitude toward preventive health care). Third, the information related to healthcare provider recommendations is also lacking in the present study. We used healthcare utilization (outpatient visits and hospital admission) as a substitute to reduce the bias. Further prospective research is still required to clarify the effect of healthcare provider recommendations on the willingness to receive flu vaccination among pregnant women in Taiwan.
Conclusion
The rate of flu vaccination among pregnant women in Taiwan was low between 2014 and 2016. Trimester, age, income level, urbanization level, health-care utilization, hypertension, cardiovascular disease, autoimmune disease, chronic pulmonary disease status, and pregnancy complications were associated with the flu vaccination status in these women.
Footnotes
Acknowledgements
The study was supported in part by the National Quemoy University, Taiwan. This study is based, in part, on data released by the Health and Welfare Data Science Center, Ministry of Health and Welfare. The interpretation and conclusions contained herein do not represent those of the Ministry of Health and Welfare.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the National Science and Technology Council Taiwan (MOST109-2410-H468-009) and China Medical University Taiwan (CMU112-MF-109 and CMU112-S-39).
Ethical Statements
The database used to support the findings of this study was anonymized for privacy. The requirement for informed consent was waived. This study protocol was approved from a completely ethical review by the Institutional Review Board of the Taichung Jen-Ai Hospital, Taiwan (Approval date: 14 February 2020, No. 109-01).
Data Availability Statement
The National Health Insurance Database used to support the findings of this study was provided by the Health and Welfare Data Science Center, Ministry of Health and Welfare (HWDC, MOHW) under license and so cannot be made freely available. Requests for access to these data should be made to HWDC (![]() ).
).