
Abstract
This study aimed to investigate the understanding and experiences of mothers who have suffered perinatal loss regarding their needs after being discharged from the hospital. Data were collected through semi-structured face-to-face and telephone interviews using purposive sampling with maximum diversity. The sample included 15 mothers and 6 midwives who had experienced fetal loss and perinatal bereavement. The interviews were audio-recorded and transcribed verbatim. Conventional content analysis was used to analyze the data. Sampling was conducted from July 2022 to March 2023, continuing until data saturation was reached. The study identified 2 main categories of needs for mothers who have experienced perinatal loss: continuous healthcare (including the Comprehensive Mother Tracking System, provision of psychological welfare, and educational needs) and provision of a support network, including “spouse and family support” and “peer and colleague support.” The primary theme of this study was “Deliberating Care for Grieving Mothers.” The study results indicate that mothers who experience perinatal loss require continuity of care after being discharged. Psychological screening and counseling support are essential for both parents. Considering the significant impact of spousal, familial, and community support on an individual’s life, it is crucial to prepare the community to comprehend and embrace grieving parents.
Mothers who have experienced perinatal bereavement have different physical and psychological needs during the recovery process of perinatal loss.
Often, bereaved mothers are unaware of their needs or neglect them when they leave the hospital. To preserve maternal health, it is crucial for policymakers and health planners to understand and meet the needs of mothers who suffer from perinatal loss.
Prioritizing the maintenance of a mother's health can greatly alleviate the negative impact of physical and mental illnesses after perinatal loss, as well as the resulting economic and social costs.
Introduction
The loss of a fetus is a devastating event that can shatter the hopes and dreams of parents.1,2 Losing a fetus in the perinatal period can refer to a miscarriage (before 20 weeks), stillbirth (after 20 weeks gestation), or neonatal death (within 28 days of life), and is one of the most painful experiences an individual can go through. 3
While most women experience natural grief responses to the loss of a fetus, about 25 to 30% of them may experience long-lasting, severe, and complicated grief reactions that can negatively affect their mental health. 4 Unfortunately, this event puts mothers at risk of grief, anxiety, guilt, and self-blame, and these feelings can even continue into subsequent pregnancies. 5 Research shows that the psychological consequences of fetal loss experienced by mothers can last for months.4,6,7
Moreover, this event has short-term and long-term psychological and social consequences for family members.8,9 Grieving mothers face many challenges after being discharged from the hospital, and it is necessary for them to receive care to improve their psychological and physical well-being. 9
Perinatal bereavement care involves physical, psychological, emotional, and spiritual support after fetal loss. 10 Emotional care is an essential part of comprehensive care, as demonstrated by Furtado-Eraso et al. 11 The studies have identified various psychological and supportive needs of grieving mothers,12,13 such as coping with grief, dealing with self-blame and guilt, 14 seeking help to overcome emotional distress, 15 counseling on the nature and duration of grief, 16 and managing mood swings due to emotional fluctuations. 17
Mothers’ needs are diverse, and some grieving mothers have reported feeling unprepared for the physical changes of postpartum and feeling lost when facing these symptoms. For instance, they may be unaware of how to deal with milk flow after stillbirth, vaginal bleeding, whether it is natural or abnormal, and their individual needs for follow-up visits. 18
Efforts have been made to provide standard care for mothers with perinatal mortality.
However, these guidelines are designed based on the cultural characteristics of countries, their available resources, and some evidence-based research. Australia and New Zealand, 19 Canada, 20 England, 21 and Ireland 10 have developed guidelines, but most of the content is focused on dealing with and caring for the mother in the hospital. Australia, on the other hand, has included a section on comprehensive post-discharge care in its Clinical Practice Guideline. 19 In Iran, however, no care has been provided beyond brief physical care, despite the fact that mothers have a range of needs. This research was conducted to identify these needs, prioritize the provision of care, clarify the necessary support program and enhance clinical performance, taking into account cultural backgrounds. In the Iranian public healthcare system, midwives provide free postpartum care to mothers who visit government clinics for 3, 10, and 40 days after delivery. In the case of miscarriage or stillbirth, mothers can visit healthcare centers for physical care whenever they want, depending on the circumstances. The national midwifery and childbirth services guidebook provides diagnosis and treatment for miscarriage or stillbirth, chromosomal analysis in recurrent fetal deaths, and examination of the fetus after death. Additionally, attention is given to maternal health indicators such as bleeding, blood pressure, and care of the episiotomy to ensure the health of mothers after miscarriage or stillbirth. However, most of these mothers do not seek care until several weeks after losing their fetus due to shock.
Despite the extensive prenatal care program for mothers, no comprehensive program has been developed for the care of mothers who have lost their pregnancy. Researchers have focused on various aspects of care in their studies, “Allah Dadian” and colleagues have shown that support from spouses, families and healthcare centers are among the most important needs of mothers who have experienced stillbirth. 22 “Sadeghi” and colleagues focused on the spiritual needs of family members after the loss of a newborn, 23 while Hosseini Chavoshi and colleagues discussed the psychological consequences of induced abortion for mothers. 24
Interventions have also been implemented to improve the well-being of mothers after abortion, 25 counseling following miscarriage 26 and stillbirth. 27 However, these interventions have mostly concentrated on alleviating symptoms of anxiety and depression.
Mothers who have experienced perinatal loss have diverse needs after being discharged from the hospital. Their experiences and perceptions can help the healthcare system develop guidelines and necessary protocols, and prepare staff to respond and provide appropriate care for these mothers. A deeper understanding of these mothers’ needs can help identify the most significant issues and provide effective services to support them.
Material and Methods
Design
This qualitative study utilized the conventional method of content analysis, which is a research technique that allows for valid and reproducible inferences from texts to their respective fields of application. 28
Participants
In order to gain insight into the experiences of maternal health in Iran, researchers conducted interviews with a cohort of mothers and midwives. The sampling method used in this study was purposive sampling, which aimed to maximize diversity. The selection of mothers was based on various factors, including their obstetric history, regarding perinatal loss, such as the number of spontaneous miscarriages, stillbirths, ectopic pregnancies, molar pregnancies, early neonatal deaths, as well as parity. Other factors considered were their education and employment status, as well as their place of residence, whether in an urban or rural area.
The researchers believed that most mothers would initially seek midwifery services at health centers because they are free and easily accessible. Midwives, as primary caregivers, are the best sources of information to comment on the needs of bereaved mothers, as they have closely interacted with and experienced the needs of these mothers. The midwives who participated in the study had at least 5 years of experience working in a hospital or clinic and were Iranian and married. The interviews were conducted one-on-one at the midwives’ workplaces. The researchers continued conducting interviews until they no longer obtained new information. Lincoln and Guba proposed that sample size determination be guided by the criterion of informational redundancy, that is, sampling can be terminated when no new information is elicited by sampling more units.
This study included 15 mothers and 6 midwives who were interviewed and saturation of information was achieved. The researchers identified potential participants by reviewing hospital records and contacting individuals who had recently been hospitalized. Due to COVID-19 restrictions, 10 of the interviews were conducted over the phone, while the remaining 5 were conducted face-to-face at a nearby health center.
In summary, the researchers conducted a qualitative study using content analysis to examine the experiences of mothers and midwives with maternal health in Iran.
Sampling ended when no new data was obtained, and the findings in the last interview were repetitions of previous codes.
Data Collection
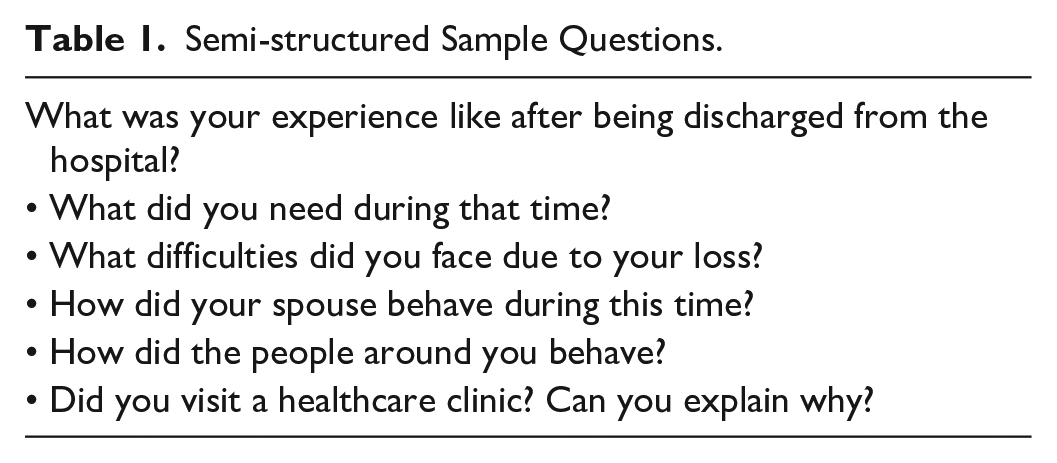
Data was collected through semi-structured interviews. After reviewing several articles and piloting 2 interviews with mothers, an interview guide was developed. The research team then reviewed and revised the interview questions. The interviews began with general questions and progressed to exploratory questions (see Table 1).
Semi-structured Sample Questions.
The interviews were conducted by GA from July 2022 to March 2023, and each interview lasted between 20 and 45 min. We obtained permission to record the interviews and transcribed them exactly as spoken after listening to them multiple times. We assured the participants that their interviews would remain confidential and that the recordings would be deleted once the project was finished. Verbal consent was obtained during telephone interviews, and written consent was obtained during in-person interviews. We made it clear to the participants that they were free to withdraw from the interview at any time, and if discussing certain memories became too distressing for them, they did not have to continue. The location for in-person interviews was chosen based on the participants’ preferences and availability at a health center.
Data Analysis
We used qualitative content analysis and Graneheim & Lundman’s method 29 to analyze the data. We employed MaxQda 10 software to code the data. We carefully read through the text multiple times until we fully immersed ourselves in the data. We selected sentences as the units of meaning and identified significant and key words, which we assigned initial codes. We provided our interpretations of the text and extracted inferential codes. We cyclically reviewed the codes by condensing and summarizing the text until we obtained the final codes.
Next, we grouped the codes based on their similarities and connections using an inductive approach. Lastly, we identified 1 theme, 2 categories, and 5 subcategories.
Trustworthiness
To ensure the accuracy and reliability of the data, we utilized the Lincoln and Guba 30 criteria and employed several methods. These methods included participant validation through member checking and returning interview transcripts to participants to confirm the research findings. We also used bracketing to prevent the researcher from misrepresenting perceptions, 31 data triangulation, and the use of multiple data sources (mothers and midwives). Additionally, we had colleagues review the study and an external observer rechecked the texts and codes. Finally, we sent the texts and codes to an external academic with experience in qualitative research who gave their approval, resulting in a high level of agreement on the obtained results.
Results
The demographic information of the participants is presented in Table 2. Fifteen mothers, aged between 27 and 40, participated in this study, with an average age of 31.1 years old. All of them were married and had experienced fetal loss due to spontaneous miscarriage or stillbirth. The educational level of the mothers ranged from elementary school to master's degree, and most of them were homemakers. Additionally, 6 midwives with an average work experience of 16.8 years participated as key informants.
Demographic Information of the Participants.
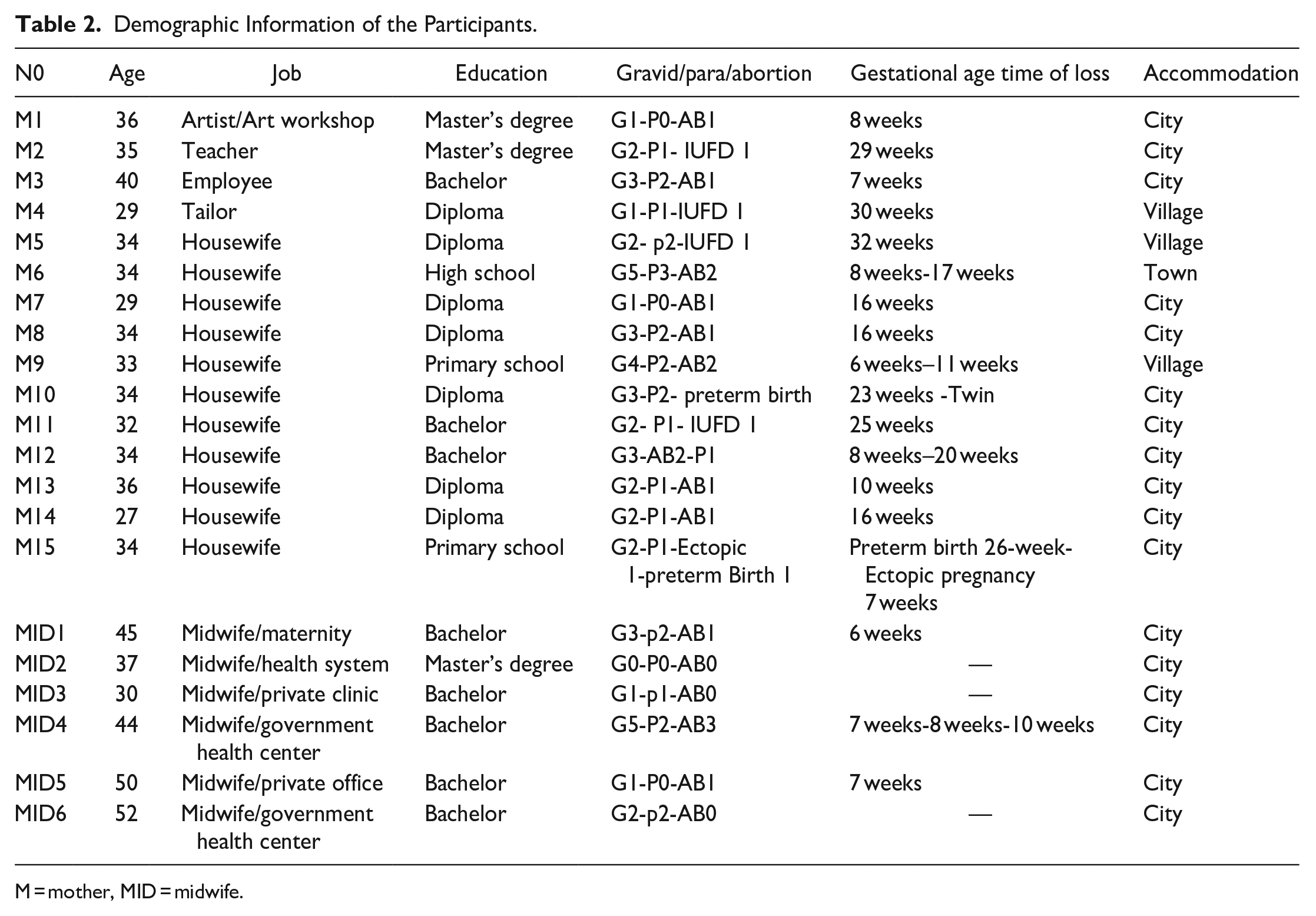
M = mother, MID = midwife.
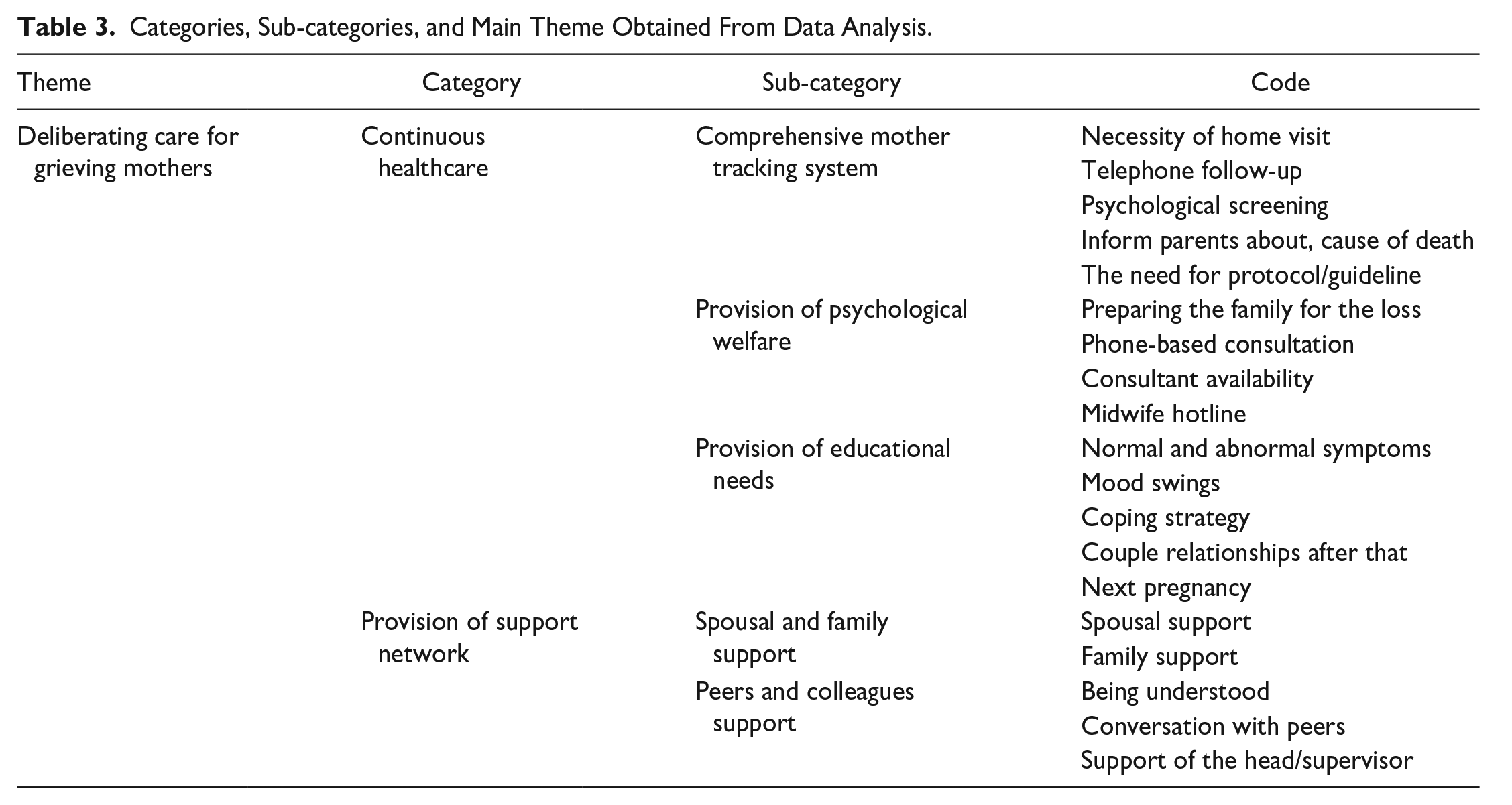
The data analysis revealed 2 categories: “continuous healthcare” and “provision of support network,” as the pressing needs of the mothers. The primary theme of this study, “Deliberating care for Grieving Mothers,” was derived from these categories. The first category of continuous healthcare includes 3 sub-categories: “Comprehensive Mother Tracking System,” “Psychological Welfare Provision,” and “Educational Needs Provision” are the categories described below in Table 3.
Categories, Sub-categories, and Main Theme Obtained From Data Analysis.
Comprehensive Mother Tracking System
Many mothers and midwives have reported that mothers still require comprehensive care after being discharged from the hospital and should not be left on their own. The existence of a system that can provide coverage for these mothers is necessary.
A 37-year-old midwife with 12 years of experience in managing healthcare systems says, “If there is a liaison midwife who informs the health center when a mother is discharged from the hospital, the midwife at the clinic can take care of her. Many of these mothers did not establish a pregnancy file at the health center from the beginning, and the midwife at the clinic has no information to follow up with them. Now, if this mother experiences a physical or mental problem, such as psychosis, and we, as the responsible party for care in the healthcare system, are not aware of it, it can have worrying consequences for her and her family. We had a mother who wanted to commit suicide. . ..”
A 52-year-old midwife with 27 years of experience in the delivery room and health services said, “A plan needs to be developed, and these mothers need to be followed up. At least two weeks later, they should be screened psychologically by phone. How are they feeling? Are they eating? How is their sleep? Someone who is grieving may really need active intervention, in my opinion. They need a special counseling hotline.”
One issue raised by several participants was the ability to communicate with their own midwife when needed. Although making calls after office hours is not officially available in the public healthcare system, the existence of mass communication media such as Whats App, text messaging, and mobile phones, as well as the friendly relationship between mothers and midwives in government clinics, has been very useful for some mothers to share their needs, issues, and problems with their midwives. This has given them a sense of value during their times of despair.
A 35-year-old mother, who experienced a stillbirth at 29 weeks of pregnancy, shared her experience: “I was being supervised by a midwife at a government clinic. When the incident occurred and my baby was stillborn, I reached out to her through a message. She called me back, which made me feel better. I really wanted her to reach out to me.
She advised me to visit the clinic as soon as I could after being discharged from the hospital. If I couldn’t make it, she offered to come to my place instead. This follow-up made me feel reassured. After leaving the hospital, I experienced discomfort from my stitches, so I messaged her about it. She responded in a very kind manner. It was really beneficial for me.” (M2)
One of the issues highlighted in the study was the importance of informing mothers or parents about counseling centers or clinics that are available for their use when needed.
Psychological Welfare Provision
A midwife with 9 years of experience from a private center stated, “Based on my experience, mothers who have experienced loss, especially stillbirth, should be referred from the hospital to a center. This way, they can receive support from a strong team consisting of midwives and, if necessary, a psychologist. These individuals not only provide psychological support but also offer midwifery consultation to address any questions they may have.” (MID3)
The findings of the study revealed that most parents expected to receive a thorough explanation of the process for requesting fetal autopsy and sample testing. Furthermore, during the post-discharge visit, the cause of death should be explained to the parents using simple and easily understandable language.
A 34-year-old mother shared, “The hospital sent the sample to the laboratory themselves, but they did not inform us that we had the option to request an autopsy. We were unaware that we could do it ourselves, even if we had to cover the expenses. They only provided us with the result of the sample test, which stated that the problem was blood clotting. However, the doctor did not explain it well. What does that mean?” (M5)
One of the recurring themes in the participants’ discussions was the need for counseling to improve their psychological well-being. Although counseling services are available free of charge, with clinical psychologists available in health centers, many mothers were unaware of this service. At the time of discharge from the hospital, no reference was made to available counselors or their contact information.
A 40-year-old working mother stated, “Everyone, from my acquaintances to my doctor, advises me on what to do for the next pregnancy and what not to do. But I’m still grieving; I haven’t come to terms with it yet. I still feel burdened, and I wish there was a counselor I could talk to who could help me feel better. But I didn’t know anyone, and when I asked my friends, they didn’t know anyone either.”
Not only should mothers receive psychological support, but the psychological well-being of family members should also be taken into consideration.
It is an important responsibility of healthcare and treatment staff to prepare family members for coping with a traumatic event. This preparation should begin at the time of the event. However, the consequences of such an event will undoubtedly persist for a long time, making counseling for family members essential.
To illustrate this point, a 34-year-old mother who gave birth to premature twins at 23 weeks shared her experience.
She stated: At the hospital, my wife and mother-in-law were not prepared for the sudden and devastating news about our children. They had arrived at the hospital filled with joy and hope, expecting the medical staff to place our twins in the machine [means neonate incubator] and ensure their survival. Instead, they were instructed to pray for wife survival. They were all sat there crying uncontrollably. After we return home, my husband’s coworkers kept calling him sensing a change in his demeanor and asking if he was alright. He chose not to disclose the extent of his emotional turmoil and sadness to his colleagues. His sadness persisted for a significant period of time. (M10)
A 34-year-old mother who had experienced fetal death at 32 weeks said, “I feel more pain for my husband than anything else. He really wanted this baby, and he had big dreams. I wish there was a counselor who could help him cope with his emotions.”
Familiarizing family members with the normal grieving process will lead to appropriate reactions. Some family members who were taking care of the mother believed that she should not think about the lost child at all. Others, due to lack of knowledge about the grieving process, asked the mother not to cry and considered it inappropriate to cry for a fetus. Mother number 5 said: If the doctor or midwife had talked to my mother or family, it would have been very beneficial. It would have had a great impact. At that time, they allowed me to cry as much as I wanted and let out my feelings. When I cried softly, I felt lighter, and better. But since I was at my mother’s house, she didn't allow me and said I shouldn’t mourn for an innocent child because it would prevent me from getting pregnant again! This is a superstitious belief.
Educational Needs Provision
Many of the participants expressed a need for information related to their health and wellbeing. They felt uncertain about how to address these concerns without visiting a clinic or health center.
These mothers had tried to fill their educational gaps by searching the internet or asking friends and relatives, but they were uncertain about the accuracy of the information they received. Therefore, access to reliable and scientific sources of physical and psychological information was essential.
A 34-year-old mother who had experienced 2 unsuccessful pregnancies and a premature birth at 26 weeks shared, “I used to go to the clinic and ask for information, but it was difficult for me to do so because it brought back memories of my pregnancy care. However, if there was a reliable source where I could obtain information, such as the hospital website or the internet, it would have been helpful. They could have provided me with information tailored to mothers in similar situations.”
Another mother who had a miscarriage at 16 weeks shared, “When I was discharged and went home, my breasts started to produce milk after a day or two. I was extremely upset and cried a lot. I felt a lot of pressure and didn’t know what to do. The people around me suggested massaging my breasts until they were empty. The hospital didn’t provide any guidance. The specialist’s clinic was always busy, and I didn’t have the patience to wait for hours.”
A 40-year-old mother and employee who had previously experienced a miscarriage at 7 weeks, also expressed her thoughts on the importance of guidance and support for mothers who have gone through a miscarriage.
She says: “Mothers really need guidance on what to expect when it comes to bleeding, pain in the lower abdomen, and weakness. How long should they use pregnancy prevention methods? How can they cope with their suffering? Does the emotional turmoil continue? Is All this crying normal? You know, for the first two weeks, one is not even in this world. . .
But afterwards, one needs to know. I wish they would schedule a session for us in the hospital after two or three weeks.”
Second Category
Provision of a Support Network
This category consists of 2 sub-categories: “spouse and family support” and “support from peers and colleagues.”
“Spouse and family support.”
For the majority of participants, support from their spouse was considered crucial in fostering a sense of calm and resilience amidst the pain of loss. The understanding and support received from their spouse made the bitter experience more manageable.
My spouse provided immense support. He reassured me that it was an accident. . . there’s no need to be upset, we still have our youth. His actions brought me peace. (M12) When your spouse empathizes with you and stands by your side, you feel better equipped to endure it. (M6)
Support from family members and acquaintances had both positive and negative aspects. From the perspective of mothers, some close family members expressed their grief over their own loss with sharp reactions toward the mother. One mother shared her experience, saying: “My mother had prayed a lot for me to get pregnant. When she heard the news of my pregnancy, she gave sweets to people around me. Then when I had a miscarriage, she didn’t call me for four days and was angry with me. . . She kept saying it was my fault. . . Are you happy now?” (M9)
Providing the desired conditions and environment for mothers is a crucial aspect of the support that family members and acquaintances can provide. However, some mothers often feel isolated and alone.
“After leaving the hospital, I went to my mother’s house. I wished for more people to be around me, but I didn’t want to have to explain my situation to everyone. Whenever they asked, even my family members would just laugh. I kind of enjoyed that, but I didn’t want anyone else, like neighbors or extended family, to come over and make me explain everything. I really didn’t like that at all.” (M11)
“All I wanted was to be alone and cry.” (M8, M5, M6)
“I just wanted to be discharged from the hospital soon so I could go to a remote place and scream, letting everything out.” (M12)
Support from peers and colleagues
According to some participants, having conversations with other mothers who have experienced a miscarriage or pregnancy loss can provide comfort and empathy.
One mother shared, “Talking to my family members who have gone through a miscarriage themselves was reassuring. They said things that helped me feel at peace. For example, my cousin told me: ‘Don’t be sad. Maybe it wasn’t meant to be. God knows better’.” (M15)
An experienced working mother who also had a miscarriage mentioned, “Just talking to other mothers like myself and realizing that you’re not alone in this situation, helps. It gives you hope that you can start over again. I had a colleague who went through this, and talking to her was a great support for me.” (M3)
Working mothers mentioned that support from their colleagues was one of their essential needs. They expressed a need for understanding from others, particularly from other mothers.
A midwife who has suffered 3 miscarriages herself stated, “Sometimes, even experts in the medical field make insensitive remarks to these mothers. When our staff’s knowledge is insufficient, they do not know what to say or how to comfort these mothers. For example, even when the head of the Maternity Ward, a head nurse, or a staff member under their supervision suffers a miscarriage and is not feeling well, they often say, ‘What’s the big deal? Let’s try again!’ These kinds of comments are heartbreaking!” (MID4)
“Understanding from those who have gone through the same reduces the pain. It is important for them to know that others are concerned about their well-being.” (M11, M1)
Discussion
The findings of this study suggest that mothers in Iran society and culture who have experienced perinatal loss, have specific needs that that require attention. The analysis of their experiences revealed that their most crucial need was ongoing post-hospital care as well as a support system encompassing family, community, and the workplace.
In Iran, post-loss maternal follow-up only focuses on physical symptoms and complaints, neglecting psychological care in the care plan. Participants noted that the lack of knowledge about the expected changes after a loss, whether natural or unnatural, can lead to physical and psychological consequences. These consequences can impact not only the mother’s health but also the overall functioning of the entire family, including potential separation from the spouse, marital conflicts, 32 and feelings of fear, guilt, and anxiety in children. 33 These issues have been highlighted in previous studies. It is important to acknowledge that the goal of qualitative studies is not to generalize the findings to the entire population but rather to provide a rich, contextualized understanding of some aspect of human experience. Iranian mothers residing in Iran were encountering these needs providing an opportunity for managers to plan and address their specific needs.it is possible that the needs of these mothers may differ from those living in larger cities.
While psychological screening 6 weeks after the postnatal period can detect early psychological disorders, 34 it is also crucial for parents to be aware of mood changes during grief and understand coping mechanisms to reduce stress and prevent adverse outcomes. These findings can be incorporated into prevention programs. Early psychological screening, such as the Perinatal Grief Intensity Scale (PGIS), can assist in the early detection of psychological disorders. 35 Furthermore, the study’s finding suggest that parent awareness of mood changes during grief and knowledge of coping strategies can decrease stress and prevent potential consequences.
The study also revealed that mothers lacked awareness and information about common physical problems during the postpartum period as well as their own needs. Although health workers, midwives, and obstetricians may provide general education before discharge, Parents may not be immediately ready to understand or retain the information provided. Therefore, emotional and informational support is necessary until they transition out of the shock phase and return home. 36
In our study, the participating mothers expressed concern about the healthcare system’s disregard for fathers’ psychological well-being. Many of them discussed fathers’ feelings of sadness, despair, and anger. Previous studies have also found that fathers react to unexpected news with shock, experience pain from loss, feel grief, helplessness, and despair, and have a sense of emptiness.37,38 Horsch and colleagues have observed that society's focus on fathers’ role in providing physical and emotional support to mothers has led to the neglect of their own needs. 39 Therefore, it is crucial to prioritize their psychological well-being and provide counseling as needed. Faleschini’s findings also highlight the importance of offering psychological support to men who have experienced prenatal loss. 40
Camacho Ávila’s study and colleagues emphasize the importance of social support following stillbirth and infant death for parents, as it can help prevent negative emotional consequences. 38 This finding supports our own research on the significance of providing a supportive network. Family support, especially from a spouse, plays a significant role in promoting the health and well-being of grieving mothers. Bhat and colleagues’ study has shown that the lack of social support is a risk factor for prolonged grief. 41 Additionally, Watson and colleagues have identified family members, partners, and healthcare providers as sources of support. 13
Supporting a grieving mother through listening and companionship from friends is also described as a soothing and supportive factor. 42 In this regard, the work environment and coworkers’ behavior are also essential parts of society. Some mothers reported difficulty returning to work due to insufficient support or uncompassionate behavior from their superiors. 43 In this research, some working mothers were afraid of expressing their sadness, work pressure, and hurtful words from colleagues or managers due to being stigmatized. The researcher’s empathy and assurance that the name would not be revealed led to the interview taking place in a confidential environment, allowing them to express their needs. Mothers’ lack of self-confidence and fear of their manager could limit their ability to express their thoughts. On the other hand, some studies have reported support from supervisors, compassionate behavior, or approval of leave for grieving individuals. 44 It appears that teaching organizational behavior that emphasizes empathy and compassion is a fundamental aspect of human behavior. Therefore, it is necessary to include such training in management programs and employee training programs.
Limitations
Due to the COVID-19 pandemic, some grieving mothers were unable to participate in face-to-face interviews and were instead interviewed over the phone. This study aims to address the issue of post-discharge care needs, which has received limited attention in previous qualitative studies conducted in Iran Country.
Conclusion
The healthcare system, long with family and social support systems, plays a crucial role in meeting the needs of mothers who have experienced perinatal loss. To prevent negative outcomes and promote maternal well-being, it is essential to provide ongoing bereavement care and psychological support for both parents. This can be accomplished through the implementation of psychological screening programs, addressing educational and counseling needs, and preparing society and workplaces to understand the challenges faced by grieving mothers and offer support as they navigate their way back into daily life.
Supplemental Material
sj-docx-1-inq-10.1177_00469580231223763 – Supplemental material for Desired Care for Perinatal Bereavement: Meeting the Needs of Mothers After Discharge From the Hospital—a Qualitative Study
Supplemental material, sj-docx-1-inq-10.1177_00469580231223763 for Desired Care for Perinatal Bereavement: Meeting the Needs of Mothers After Discharge From the Hospital—a Qualitative Study by Giti Atashsokhan, Maryam Farjamfar, Ahmad Khosravi, Mahboobe Taher and Afsaneh Keramat in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580231223763 – Supplemental material for Desired Care for Perinatal Bereavement: Meeting the Needs of Mothers After Discharge From the Hospital—a Qualitative Study
Supplemental material, sj-docx-2-inq-10.1177_00469580231223763 for Desired Care for Perinatal Bereavement: Meeting the Needs of Mothers After Discharge From the Hospital—a Qualitative Study by Giti Atashsokhan, Maryam Farjamfar, Ahmad Khosravi, Mahboobe Taher and Afsaneh Keramat in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
This study was part of the results of the Ph.D. thesis approved by Shahroud University of Medical Sciences (code 904). We are grateful to the Vice Chancellor of Research and Technology, staff, colleagues, and all participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent for Participation
Written and oral informed consent was obtained from all participants including a telephone interview the study also received ethical approval from the ethics committee of Shahroud University of Medical Sciences code IR.SHMU.REC.1400.011.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.