
Abstract
Internal medicine departments must adapt their structures and methods of operation to accommodate changing healthcare systems. The present paper discusses some challenges departments of medicine face as healthcare providers and consumers continue to change. A co-pilot model is described in this article for augmenting physicians rather than replacing them. The paper presents the co-pilot models to improve diagnoses, treatments, and monitoring. Personalized variability patterns based on the constrained-disorder principle (CDP) are described to assess chronic therapies’ effectiveness in improving patient outcomes. Based on CDP-based enhanced digital twins, this paper presents personalized treatments and follow-ups that improve diagnosis accuracy and therapy outcomes. While maintaining their professional values, departments of internal medicine must respond proactively to the needs of patients and healthcare systems. To meet the needs of patients and healthcare systems, they must strive for medical professionalism and adapt to the dynamic environment.
Highlights
• The paper discusses some challenges departments of medicine face as healthcare providers and consumers continue to change.
• A co-pilot model is described for augmenting physicians rather than replacing them for improving diagnoses, treatments, and monitoring.
Introduction
The healthcare system is constantly evolving. There are changes in the type of patients admitted to hospitals, the need for high-quality, low-error care, and the implementation of digital systems based on artificial intelligence (AI). Internal medicine departments and their methods for diagnosis and treatment need to change significantly to meet these challenges.
A schematic model for future medicine departments is described in the present paper, which reviews some of the challenges healthcare systems face. Healthcare systems in different countries may differ, but the principles outlined here can be adapted to fit all of them. Models for improving diagnosis and treatment using algorithms are presented in the paper. This paper aims to investigate second-generation artificial intelligence systems that use constrained-disorder principle-based techniques to enhance the response to chronic therapies for better patient outcomes.1 -3 CDP-based enhanced digital twins are presented to improve diagnosis accuracy and personalized treatments and follow-ups. 4
Study Design
The paper presents a narrative review explaining the existing knowledge on a topic based on all the published research available. It describes some relevant studies on the current challenges of the healthcare system. It then presents the CDP-based models incorporating second-generation artificial intelligence (AI) systems for improving diagnosis, treatment, and monitoring and describes the suggested models for the medicine departments.
Results and Discussion
Some of the Current Challenges of Healthcare Systems
Healthcare has faced numerous challenges over the last decade. An increase in ambulatory care over inpatient care is one example, as are the numbers of acutely ill inpatients requiring close monitoring, high-quality outcomes at lower costs, improving patient experience, increasing interdisciplinary teams, and increasing biological and clinical phenotypic information. 5 A skilled multidisciplinary team is essential to achieving high-value care and is expected to play an important role in clinical care. Medicine departments must be flexible, decentralized, and responsive to patient preferences. 1
It is challenging for healthcare organizations to integrate their supply chains. The pharmaceutical supply chains of Italian healthcare organizations were examined through an exploratory multi-case study. According to a recent study, 7 critical barriers to digitally enabled SCI in healthcare are primarily motivated, unwilling to change, not cost-effective, and lacking initiative from health authorities and dominant players. 6 Based on a recent study, 65% of pharmacists working in public health facilities are unsatisfied with their jobs. Remuneration, co-worker relations, and facility conditions were all major influencing factors. There is a need for a comprehensive strategic review in the health sector that focuses on remuneration, working conditions, and interpersonal relationships to boost job satisfaction and retention. 7
With the advent of digitalization, more and more sectors, including the healthcare sector, are being affected. Electronic records and the ability to control the patient outside the doctor’s office are becoming increasingly necessary. Medicine and hospitals can benefit from digitalization in some fields and cannot in others. 8 Challenges include what can be accomplished with digital systems, what they require to do themselves, and what risks they bear or how they are controlled. In the wake of the COVID-19 pandemic, AI/robotics have become mandatory since the utilization requirements, particularly in logistics and health, have increased. Human life and basic needs are protected by the solutions proposed by these technologies to reduce the risks. 9
Digital health systems and digital twins have introduced a new player to diagnosis and treatment algorithms.10 -13 These systems can be used to improve diagnostic accuracy and provide personalized treatments. 6 Due to the COVID epidemic, remote treatment and monitoring improved, resulting in the need to enhance home therapies and hybrid departments, which divide healthcare between the department of medicine and the patient’s residence. 6 Internal medicine departments must develop cutting-edge approaches to diagnosing and treating to provide better-value clinical care. By implementing virtual medicine, assistive and intelligent technologies, and care processes, healthcare delivery can be transformed. 15
A significant challenge in technology management is sustaining competitive advantage through radical and incremental market innovations. The pharmaceutical industry was described as a problem-driven innovation environment and showed that consequential problems and their solutions co-evolve to produce radical innovations. In an environment where innovation-based competition drives technological and industrial change, it explains one of the sources of innovation. 14
Motivation and the creation of favorable conditions are critical elements of incentive-based management aimed at motivating people and supporting organizational development. Motivation and performance of employees in public organizations are supported by intrinsic and extrinsic incentives. 15 Intrinsic incentives give personal satisfaction to individuals, including autonomy, reputation, self-confidence, trust, empowerment, and expense, and support the development of personalities in organizations. Those who work for public organizations are more likely to perform well and be satisfied due to intrinsic incentives that enhance job engagement and affective commitment. Pay, fringe benefits, gifts, promotions, advancement opportunities, and other extrinsic incentives contribute to employee loyalty. 16
Providers can enable value-in-use (VIU) in complex healthcare contexts using digital technologies. Public healthcare organizations and technology providers may not understand one another, hampering opportunities for value-in-use to emerge. By creating value for themselves, healthcare providers can justify the price of new technologies and improve their operations. They can also acknowledge the value of new technologies for patients as well. For example, automated screening technology in hospitals or robotics dispensing medicine at home are examples of how digital technologies can impact healthcare practices and lead to VIUs. By altering how care is delivered with digital technology, providers can enable value-in-use without compromising patient outcomes. 17
Digital technologies are limited in adoption by system factors related to inconsistent normative and regulatory criteria for assessing surgical expertise. The development of the innovation system can be improved significantly if these systems’ weaknesses are addressed with evidence-based training programs. 18 Algorithms can program themselves by learning from a large set of examples demonstrating desired behavior using deep learning technology. Medical imaging methods can assist pathologists in detecting cancer subtypes, gene mutations, and metastases to apply appropriate therapies. A high mortality rate of some types of cancer is driving AI technology’s application in cancer imaging to improve the detection and characterization of cancer, as well as to apply effective anti-cancer therapies. This technology can revolutionize diagnostic assessment of any cancer. 19 By applying deep learning technology to cancer imaging, pathologists can detect and classify cancer early in its development, allowing patients to receive treatment that increases their survival. 20 From the statistical analyses, one can learn a lot about introducing new technologies, as transcatheter aortic valve implantation (TAVI) is becoming an increasingly popular procedure to treat aortic stenosis. Scientific products and technological production of TAVI have disproportionately grown in the last few years, driven by technological advances to solve consequential problems to treat valvular heart diseases. Developing and adopting TAVI in cardiology is driven by diffusion via learning and diffusion by learning. 21
It is essential to provide clinical care tailored to each patient’s needs and preferences. 6 The ability to personalize care uses biomarkers and technology, including point-of-care testing, biomonitoring, telemedicine, and mobile apps.22 -24 Expanding the partnerships between departments of medicine and community physicians is required. 25
As a result of their inherently conservative nature, healthcare systems are hard-pressed to adapt to changes relating to costs and how to harness doctors to do so. The way medicine departments operate in many parts of the Western world is similar to how they did 2 or 3 decades ago.26,27 Caregivers often suffer from the “more of the same” syndrome. The rapid changes that occurred over the past decade and those to come require these departments to adapt their structure and modes of operation to the post-digital age. Patient-centered care can only be achieved by following patient-centered models. Providing intelligent, flexible solutions to health care requires moving beyond traditional patient-caregiver interactions.
Models for structures and modes of operation of the Department of Medicine are described in the following sections.
A New Structure for the Department of Medicine
There has been a marked change in the type of patients medicine departments treat. Patients who require close monitoring are admitted. 12 Parallel to this, there is a shift toward ambulatory care. It is a place where many patients who used to be in these departments can now receive care at home, in hybrid care or day hospitals. 28 Unless subjects require close monitoring, health care should be accessible wherever they are. 29
Figure 1A illustrates a model for a suggested structure for a department of internal medicine. About 20% of beds are allocated to medical intensive care, and 50% are for intermediate-level care. About 15% of the beds are to become hybrid beds, designed for patients who arrive at the emergency room and require additional in-hospital diagnostic procedures or monitoring for less than 48 h while continuing treatment at home under telemedicine supervision or at a day hospital or using hybrid mode where physicians or nurses visit the patient at home. 30 Opening low-level care beds, including geriatric beds, as part of the department of medicine depends on the local structure of senior services and aims to provide an outflow for overflow medicine departments.31,32
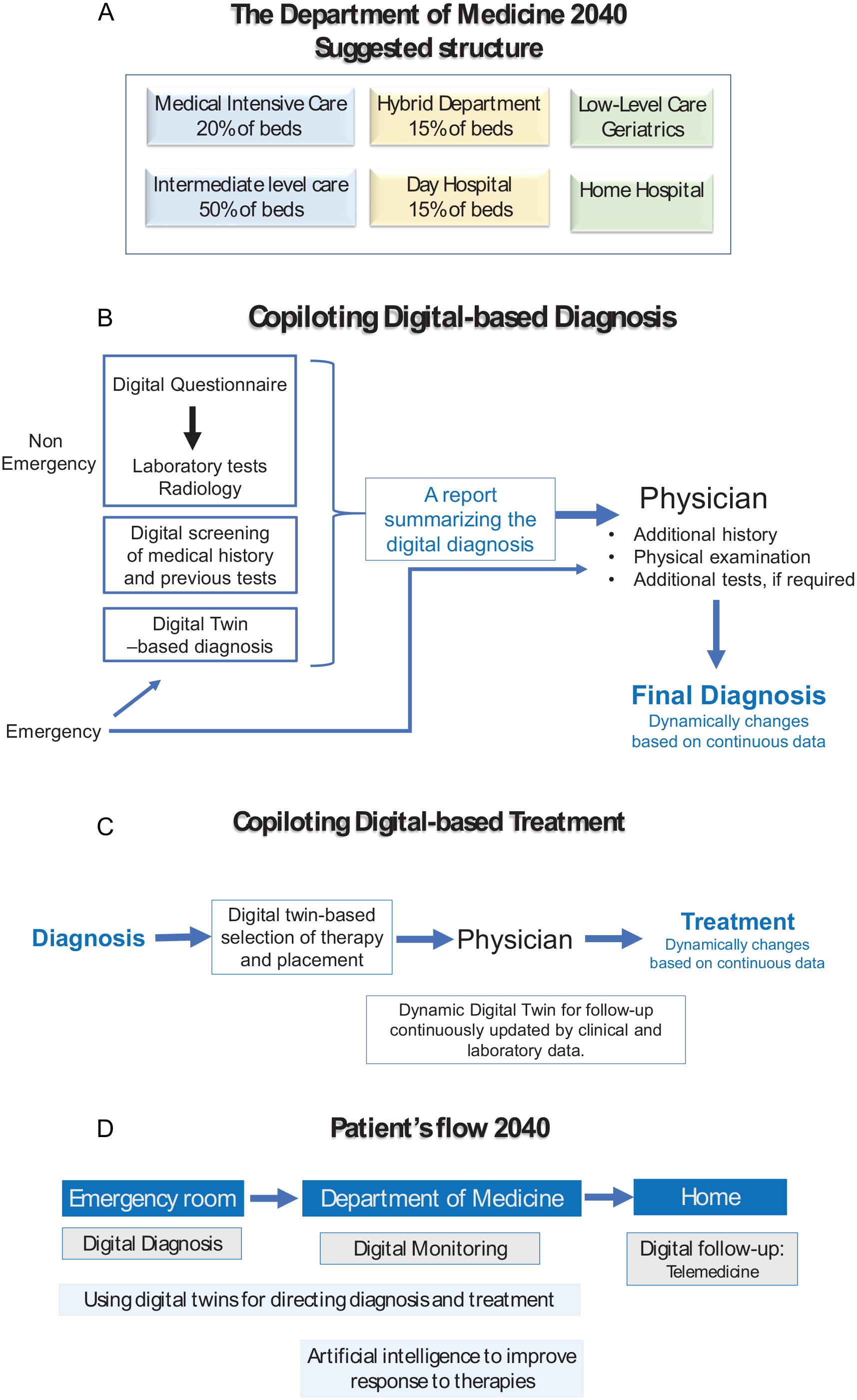
A schematic model for The Department of Medicine 2040 (all figures are personal elaborations): (A) the proposed structure of the Department of Medicine, (B) digital-based diagnosis co-pilot model, (C) digital-based treatment co-pilot model, and (D) schematic representation of a patient flow.
Medicine departments can partner with or control home hospitals.33,34 Patients with chronic diseases benefit from these departments. Heart failure patients and patients with chronic obstructive pulmonary disease are treated at home by nurses under the supervision of physicians and regularly monitored via telemedicine.34 -36
The Co-pilot Model: Augmenting Physicians and Not Replacing Them
Physicians are not going to be replaced by robots anytime soon. It is primarily driven by 2 confounding factors: physicians’ and patients’ lack of engagement with digital systems and the limitations of AI systems in complex situations.37 -39 Existing systems cannot think like an experienced physician.40,41
Co-pilot models are being developed to assist, augment, and reduce errors but do not replace the physician. Decision support systems powered by artificial intelligence are designed to help physicians analyze data and improve diagnosis and treatment. 42 For these systems to be adopted by physicians, they must be more explainable and adaptable to shared decision-making. 42
A schematic model for implementing the co-pilot model in diagnosis and treatment is shown in Figure 1B and C. A digital system can screen extensive historical and laboratory data, reducing errors and personalizing the output.
The following sections describe the co-piloting model’s use for improved diagnosis, therapy, and monitoring.
An improved diagnosis model based on co-piloting
By adding digital tools to diagnosis, errors can be reduced, accuracy can be increased, and time and human resources can be saved.43,44 The concept presented in Figure 1B aims to provide the physician with a diagnosis summary prepared by a digital system. Artificial intelligence-based tools can screen patients and select the clinical, laboratory, and radiology tests they need. 45 After reviewing the patient’s medical history, a personalized digital twin is also used to finalize the suggested summary. A patient approaches the physician with an overview of the top 5 to 10 diagnoses based on their likelihood and recommendations for additional tests. Before making a final diagnosis, the physician may ask additional questions and perform additional tests depending on the condition. Healthcare providers can handle increasing data and optimize professional skills while reducing cognitive and clerical burdens with digital systems. 29
In the proposed scheme, the physician is not replaced but saves time, reduces errors, and helps the physician make a final diagnosis. In addition to assisting physicians, the digital system allows them to spend more time with patients and better utilize their limited time with them. 46 Based on the patient’s collected data, the digital system continuously analyzes clinical and laboratory data to give the physician a dynamic diagnosis.
Improved treatment through co-piloting
A scheme for co-piloting treatment algorithms is shown in Figure 1C. Following a diagnosis, the digital system suggests treatment options based on priority. Predicting deterioration can direct the appropriate placement for the patient (eg, intensive care unit, hybrid department). It is common for physicians to select therapies based on approximations derived from large populations. The use of digital twins can allow for the creation of personalized treatment algorithms based on subjective factors.
Clinical and laboratory parameters can be continuously monitored with digital twins for a response, and treatment algorithms can be adapted accordingly. The physician is continuously updated on suggestions for treatment modifications. Using existing health risk scores for chronic diseases, the digital phenotype of digital twins presents predictive analytics tools. Care plans are proactively developed and shared virtually with patients. 29 Through early prevention, these interventions can prevent conditions from developing.
A CDP-based second-generation AI system was shown to overcome diuretic tolerance in patients with heart failure, improving the clinical and laboratory measures. 47 Similarly, improvement was shown in patients with immune-mediated disease and patients with chronic pain with loss of effects of their chronic therapies. 48
Monitoring and follow-up model based on co-piloting
New healthcare delivery models need to be improved to meet patients’ needs. Healthcare delivery with patients in examining rooms must catch up to other industries’ innovation. 29 “Morning and evening rounds” are standard in most medicine departments. Monitoring is based on placement in intensive care units and the availability of human resources. Digital twins can monitor all patient data, clinical data (structured and non-structured from EMR), electronic biosensors, laboratory and radiology data, and other data. Physicians receive continuous alerts when their subjects’ status changes so they can change their diagnosis, treatment, or further testing accordingly. Providing a continuous tool that reduces errors and enables early intervention, this type of follow-up reduces errors and provides a continuous tool that reduces errors. It improves patient care and reduces the burden on physicians.
An illustration of a patient flow from an emergency room to an internal medicine department, followed by a follow-up at home, is shown in Figure 1D. The digital twin system dynamically follows the process based on incoming inputs, enabling continuous output.
A second-generation artificial intelligence system based on constrained-disorder variability to improve treatment response
The healthcare system differs from other service providers. These systems are used by patients not because they want to but because they have to. The outcome becomes mandatory in every interaction between a healthcare provider and its customers. Co-pilot schemes for diagnosis and treatment must be implemented to improve outcomes.
Chronic disease patients are the primary burden on healthcare systems. Chronic therapies are often ineffective for these patients due to primary or secondary loss of response. 49 Costs increase when chronic diseases fail to respond to treatment, requiring more expensive interventions and admissions.
Using the constrained-disorder principle (CDP), living and non-living systems are defined by their degree of variability bounded by dynamic boundaries. 3 Biological systems are characterized by variability in genomes, cells, and whole organs.50 -63 Such variations include heart rate, blood pressure, gait, respiration, and brain function.64 -69 Adaptability and flexibility are essential for systems’ proper operation under continuous internal and external perturbations, according to the CDP. 3 Disease states are characterized by reduced variability or variability beyond dynamic boundaries. 3
CDP-based second-generation AI systems incorporate variability signatures into diagnostic and treatment algorithms to improve the response to therapies and overcome the loss of response to chronic medications.1,2,70,71 Dosing and medication administration times are altered in these systems to ensure sustainable responses to treatments.62,70 -92 CDP-based systems can also improve digital twin accuracy by accounting for biological noise in a personalized manner. An illustration of how second-generation AI systems can be implemented into therapies is shown in Figure 1D.
This review presents the concept of implementing the CDP-based system for improving care. Large amounts of real-world data are required for validation of the platform. As tiers of health systems vary across regions, implementing these models in both limited-resource and high-resource settings remained to be shown.
Conclusion
Internal medicine departments have shared values and attributes for decades. In response to current external realities, they must adjust. The commitment to medical professionalism for clinical excellence does not change, but the structures and methods must. Suggestions for the management of healthcare and departments of medicine, not only with personnel but also with new AI technologies, must consider the appropriate incentive measures. In the future, departments of internal medicine must respond proactively to the changing expectations and needs of healthcare systems and patients while maintaining traditional professional standards. 5
Footnotes
Acknowledgements
N A
Abbreviations
AI: artificial intelligence; CDP: constrained disorder principle.
Author Contributions
YI wrote the manuscript.
Availability of Data and Materials
All data is available on public resources.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Disclosure
YI is the founder of Oberon Sciences
Ethical/Consent Statement
The study did not require ethical board approval because it is a review paper.
Ethics Approval and Consent to Participate
NA
Consent for Publication
Yes
Guarantor Statement
YI conceptualized and wrote the manuscript