
Abstract
Based on the complex aging background, more and more older people have to live in an institution in later life in China. The prevalence of cognitive frailty (CF) is more higher in institutions than in communities. Rarely studies were conducted on the relationship between institutional residence and CF. Hence, this study were performed to determine the relationship between institutional residence (living in a nursing home) and CF in older adults. A total of 1004 older community residents and 111 older nursing home residents over 50 years of age from Hefei, Anhui Province, China were recruited. CF included physical frailty (PF) and mild cognitive impairment (MCI). PF was assessed using the Chinese version of the Fried frailty scale, MCI was assessed using the Montreal Cognitive Assessment, and the common associated factors including sedentary behavior, exercise, intellectual activity, comorbidity, medication, chronic pain, sleep disorders, nutritional status and loneliness were analyzed using regression logistic models. Multivariate regression logistic analysis showed that exercise (P = .019, odds ratio [OR] = 0.494, 95% confidence interval [CI]: 0.274-0.891), intellectual activity (P = .019, OR = 0.595, 95% CI: 0.380-0.932), medication use (P = .003, OR = 2.388, 95% CI: 1.339-4.258), chronic pain (P = .003, OR = 1.580, 95% CI: 1.013-2.465) and loneliness (P = .000, OR = 2.991, 95% CI: 1.728-5.175) were significantly associated with CF in community residents; however, only sedentary behavior (P = .013, OR = 3.851, 95% CI: 1.328-11.170) was significantly associated with CF in nursing home residents. Our findings suggest that nursing homes can effectively address many common risk factors for CF, including lack of exercise and intellectual activity, medication use, chronic pain, and loneliness, better than the community setting. Thus, residing in a nursing home is conducive to the intervention of CF.
With population aging, China is facing enormous pressure to care for older adults, and an increasing number of older adults (before and after retirement) may move to nursing homes in the future.
Our findings suggest that living in a nursing home can help control some common risk factors for cognitive frailty.
Our research results can inform policy decisions in China regarding the benefits of living in nursing homes to alleviate the increasing pressure to provide care for older adults.
Introduction
According to the seventh National Population Census, China has become one of the most populous countries in the world. In 2020, people over 60 years old accounted for 18.70% of the Chinese population, and those over 65 years old accounted for 13.50%. 1 This means that China has entered a super-aging society. With rapid population aging, China is also facing great pressure to support older individuals. Currently, there are 3 main residence models used to care for older adults in China: family care, community care, and institutional care. 2 Family care namely home-base care is the most common models to care for the aged which is provided by family members or employees, community care is provided by communities, and institutional care namely older adults long-term live in an institution. According to traditional Chinese cultural values, such as filial piety, most older people to live independently (the family or community models) rather than living in an institution (such as a nursing home). With the weakening of family ties and the surge in the proportion of older individuals in recent years, an increasing number of older people have considered living in a nursing home. 2 The number of older people in institutions, such as nursing homes, assisted living facilities, convalescent hospitals and combined nursing institutions, is increasing. Additionally, research has highlighted the advantages of institutional residence, such as reducing the burden on young people, meeting the health needs of older people, and promoting healthy aging.
Frailty is an important intermediate state of aging and can be further divided into physical frailty (PF), cognitive frailty (CF), and psychosocial frailty. 3 In the context of population aging, the prevalence of CF is increasing among older people with a rate of about 10%4 -9, CF is a condition with heterogeneous manifestations and is characterized by the simultaneous presence of PF and mild cognitive impairment (MCI) among older people without dementia. 10 CF represents an early clinical stage that precedes the onset of dementia 11 and increases the risks of a variety of adverse health events,4,12 -14 such as falls, fractures, disability, poor sleep quality, and even increased mortality, in older individuals. Therefore, effective interventions for CF among older adults are urgently needed and could improve quality of life. Nevertheless, most studies of CF interventions have been conducted in the community and few have been performed in institutions, despite the high prevalence of CF among older institutional adults with a rate of about 20%.15,16
CF is significantly associated with a series of risk factors including sociodemographic factors (such as older age, female sex and lower educational level),5 -9 nutritional status,17 -19 psychological status (such as depression and loneliness),6,19 lifestyle activities,5,18,20 functional status,4,20 geriatric syndromes,5,7 comorbidities,4,5,7 polypharmacy,20,21 specific cognitive functions,19,22 structural brain changes (such as cerebral small vessel disease)23 -25 and others (such as gut metabolite).26,27 Most risk factors for CF, such as older age, female sex, and lower education levels, are difficult to control, and many studies conducted in community-dwelling populations have focused on risk factors that can be controlled, such as nutritional status and activities and obtained the preliminary effect. Few studies on CF have been performed in institutions,15,16 and studies conducted in institutions have shown that older adults living in institutions experience strong feelings of loneliness, depression, abandonment, and even suicidal ideation.28,29 These factors lead to a higher risk of CF. 9
With societal development, institutional residence has become more common for older individuals. On the one hand, institutional residence seems beneficial; on the other hand, institutional residence may also aggravate the risk of CF. Hence, research is needed to elucidate the relationship between institutional residence and CF.
In the present study, we first aimed to determine attitudes of older Chinese adults toward institutional residence by asking them to indicate their preferred residence models. Then, community residents and nursing home residents were recruited, and some common risk factors for CF were examined in both groups. Finally, we discussed the relationship between institutional residence and CF. To date, few studies have examined CF in nursing home residents, and no studies have been published on this topic. We have addressed this gap and hope to provide suggestions for the intervention of CF in the older individuals in China.
Materials and Methods
This was a cross-sectional study. In our study, people over 50 years old living in the community and in nursing homes were recruited in Hefei City, Anhui Province, China. As shown in Figure 1, 200 older participants (50 years of age and over) were randomly recruited from each of 5 large communities (5 communities were randomly selected from 50 large communities in Hefei City, these large communities are home to more older people before and after retirement), including the Wanghu community, the Jixian community, the Xingyuan community, the Haiheng community and the Baohe community. Additionally, 6 nursing homes located in or near these communities were selected (the Changjiang nursing home, Songqiaoyuan nursing home, Xingyuan nursing home, Xiyanghong nursing home, Yaodong nursing home and Baohe nursing home). The intitution sample size refers to community residents’ selections of residence models (Figure 2). Eventually, a total of 1004 community-dwelling participants and 111 participants in nursing homes were enrolled. Nevertheless, 3 participants in nursing homes withdrew from the study by failing to complete all the questionnaires, and 46 community-dwelling participants withdrew from the study. Finally, 108 participants in nursing homes and 958 community-dwelling participants completed all questionnaires and were categorized according to the presence of CF into the CF and non-CF groups.
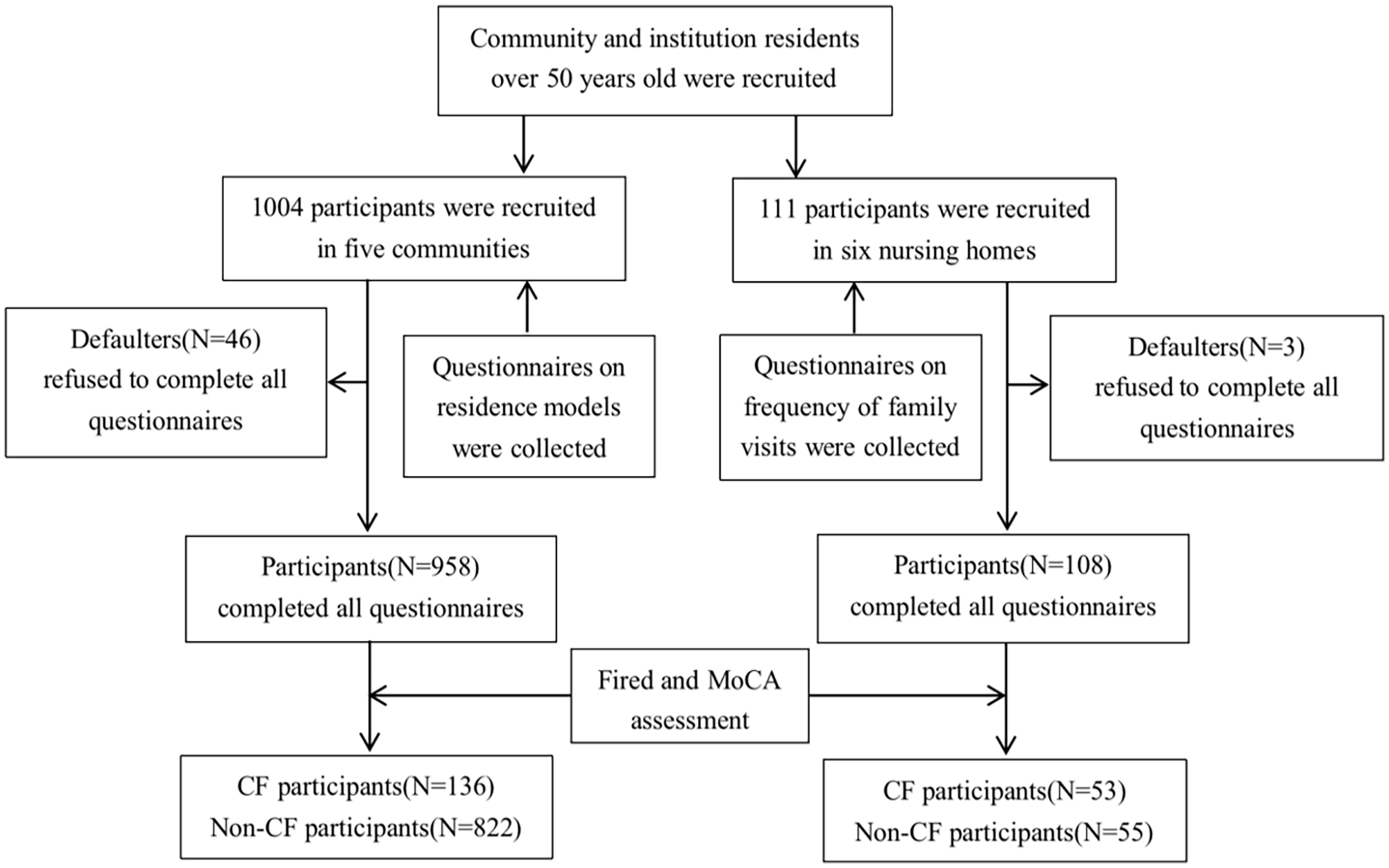
Flowchart of participant recruitment, screening, and group allocation.
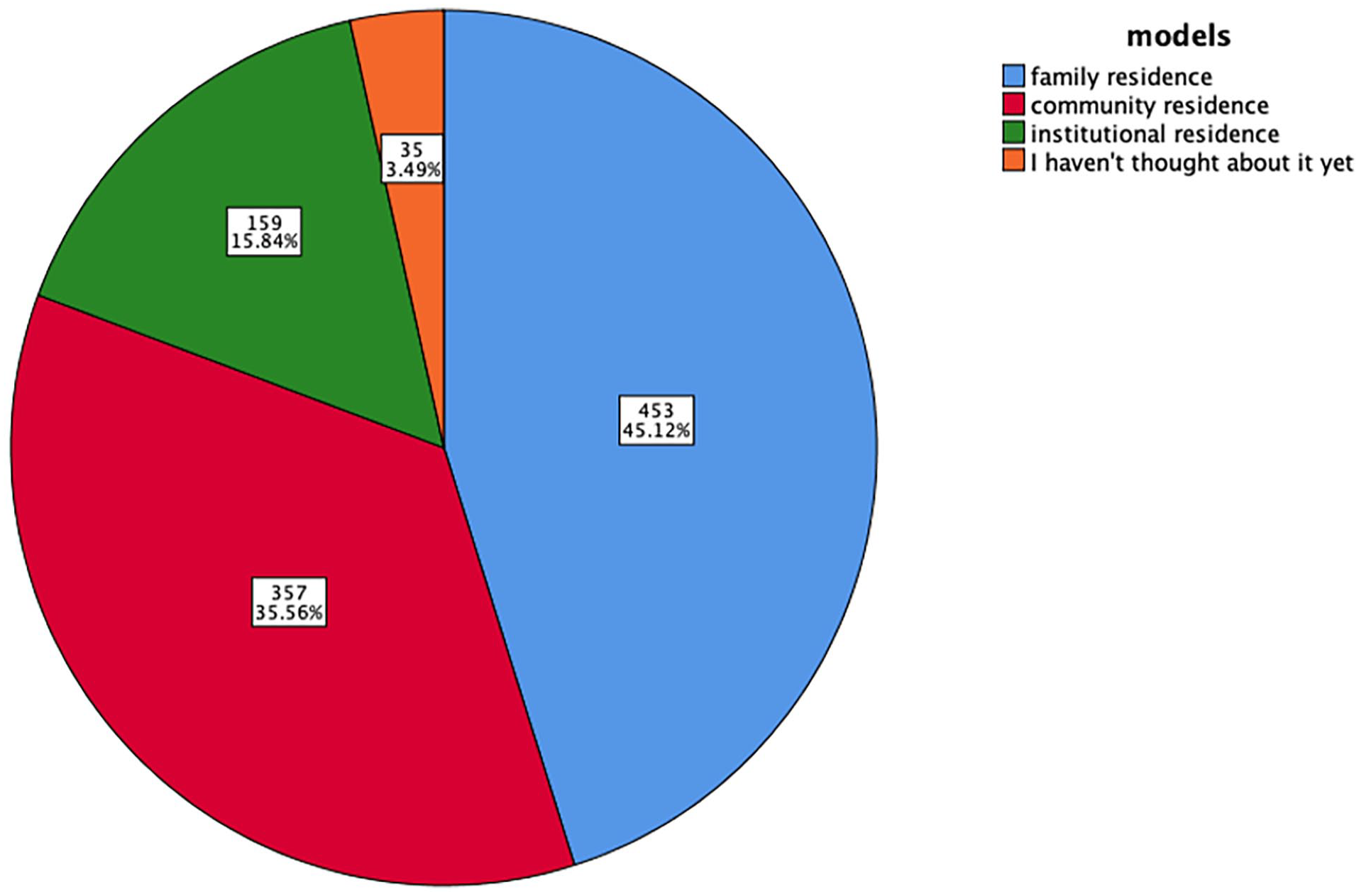
Selections of residence models by community residents over 50 years old.
This study was approved by the Institutional Review and Ethics Committee of Anhui Medical University, and written informed consent was obtained from all enrolled participants. All study procedures were performed in accordance with relevant guidelines and regulations.
Data Collection
A comprehensive questionnaire collected information on sociodemographic characteristics, lifestyle factors, neuropsychological indicators, physical function, and cognitive function from community residents and nursing home residents. Participants underwent face-to-face interview by trained experimenters. Participants were randomly recruited from July to August 2022. The inclusion and exclusion criteria for participants are detailed in Table 1. People aged 50 years and older volunteered to participate in this study and signed the informed consent form. People aged 50 years and older who had dementia; severe mental or psychological illness; or severe visual, hearing, or speech impairments were excluded. The questionnaires used in this study are validated with a Kaiser-Meyer-Olkin (KMO) score of 0.814 and a meaningful P value of Bartlett’s Test of Sphericity (P < .05).
Inclusion and Exclusion Criteria for Participants.

Operational Definition of Cognitive Frailty
The presence of both physical prefrailty/frailty and MCI was defined as CF. Frailty was assessed using the Chinese version of the Fried frailty scale, 30 and individuals with physical prefrailty and frailty were grouped together. MCI was assessed using the Montreal Cognitive Assessment. 31 The specific criteria used to detect CF are listed in Table 2. Finally, participants were classified according to the presence of CF: the CF and non-CF groups.
Operational Definitions and Classifications of Frailty and MCI.

Factors Associated With Cognitive Frailty
In our study, some common modifiable risk factors for CF were considered variables of interest and community residents and nursing home residents were screened for these factors. They included sedentary behavior (defined as spending at least half one hour per day inactive, such as sitting or reclining; self-reported), exercise (defined as engaging in physical activity, such as walking, running, and dancing, for at least half an hour per day; self-reported), intellectual activity (defined as engaging in leisure activities such as reading, writing, drawing, playing cards and so on for at least half an hour per day; self-reported), comorbidities (such as hypertension, diabetes, cancer, chronic lung disease, heart disease, arthritis, cerebrovascular disease, or kidney disease; diagnosed by a doctor), medication use, chronic pain (complained of neck pain, lower back pain, leg pain, and so on that persisted or recurred for more than3 months), sleep disorders (assessed by the Pittsburgh Sleep Quality Index [PSQI], which has a total score of 0-20; poor sleep quality was defined as a score > 7),32 -34 nutritional status (assessed by the Mini Nutritional Assessment-Short Form [MNA-SF]) 35 and loneliness (assessed with a simple question: “Do you feel lonely?,” with response options of 0 = never, 1 = rarely, 2 = sometimes, 3 = often, and 4 = always; these options were further dichotomized as yes [2 -4] or no [0 -1]). Sedentary behavior, comorbidities, use of medication, chronic pain, sleep disorders, and loneliness were previously found to increase the risk of CF, whereas exercise, intellectual activity, and healthy nutritional status were previously found to reduce the risk of CF. Owing to family visit frequency is associated with mental health among institutional residents and the frequency of family visits to nursing homes was also assessed. The frequency of visits was recorded as always (≥5 days/week), often (3-4 days/week), sometimes (1-2 days/week), occasionally (<1 day/week), or never.
Statistical Analysis
Statistical Package for Social Sciences (SPSS, Hefei, China) version 23.0 was used to generate the figures and perform statistical analyses in our study. The chi-square test (χ2) was used to compare categorical variables between groups, and the independent-sample t test was used to compare continuous variables between groups. The significance threshold was set at P < .05. Furthermore, multivariate logistic regression models were used, including only variables identified as significant in the univariate analysis as independent variables and adjusting for possible confounding factors.
Results
Only a Small Proportion of Community Residents Considered Institutional Residence
To determine the relationship between institutional residence and CF, we first aimed to determine attitudes of older Chinese adults toward institutional residence by asking them to indicate their preferred residence model. The results of the investigation showed only 15.84% reported that they would consider institutional residence in the future. Most of them (51.20%) preferred to live independently (the family and community residence models) rather than in an institution, and 12.85% were not aware of the possibility of institutional residence (Figures 2 and 3). Nursing home residents were asked to report the frequency of family visits to the nursing home, and the results indicated that nursing home residents remained close with their family members (Figure 4).

Attitudes toward institutional residence among older community-dwelling adults (before and after retirement).
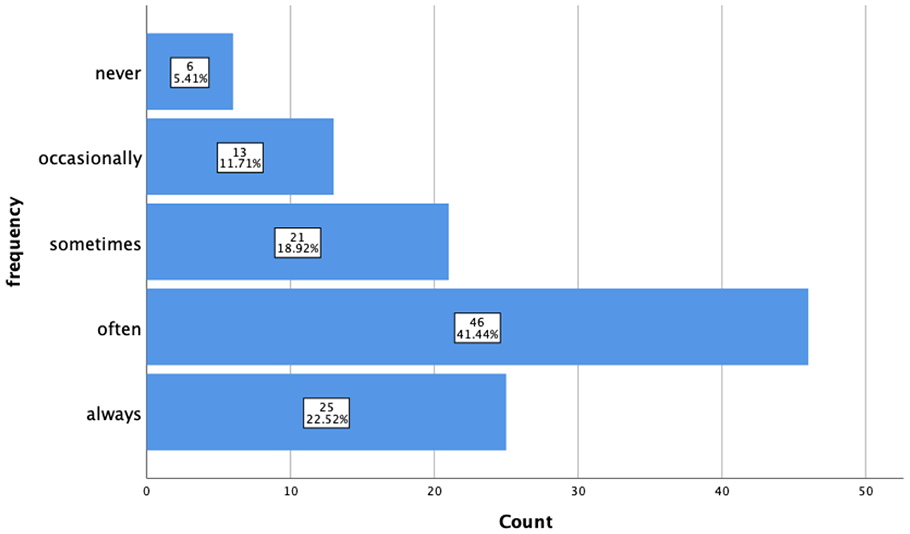
Frequency of family visits among nursing home residents.
General Characteristics of Individuals With and Without CF
As shown in Figure 1, among nursing home residents, 53 had CF (27 women) and 55 did not have CF (33 women). Among community residents, 136 had CF (106 women) and 822 did not have CF (510 women). The prevalence of CF in nursing home residents was 49.07% and that in community residents was 14.20%. The general characteristics of individuals with and without CF are presented in Tables S1 and S2. Among community residents, the average age individuals with CF was 70.82 ± 9.45 years, and that of individuals without CF was 65.06 ± 8.01 years. Among nursing home residents, the average age of individuals with CF was 81.06 ± 11.66 years, and that of individuals without CF was 73.73 ± 13.94 years. Thus, the prevalence of CF was much higher among nursing home residents, but the average age of nursing home residents was also higher than that of community residents.
Differences in CF Risk Factors in the Community and Nursing Home Groups
After establishing differences in the prevalence of CF among community residents and nursing home residents, we examined whether these 2 groups differed in common modifiable risk factors for CF (Table 3). In nursing homes, sedentary behavior and nutritional status (normal nutrition) increased the risk of CF (P < .05). In the community, sedentary behavior, comorbidities, medication use, chronic pain, sleep disorders, nutritional status (malnutrition risk and normal nutrition), and loneliness elevated the risk of CF, and exercise and intellectual activity decreased the risk of CF (P < .05).
Common Risk Factors for Cognitive Frailty in Community Residents and Nursing Home Residents.

Represents P < .05.
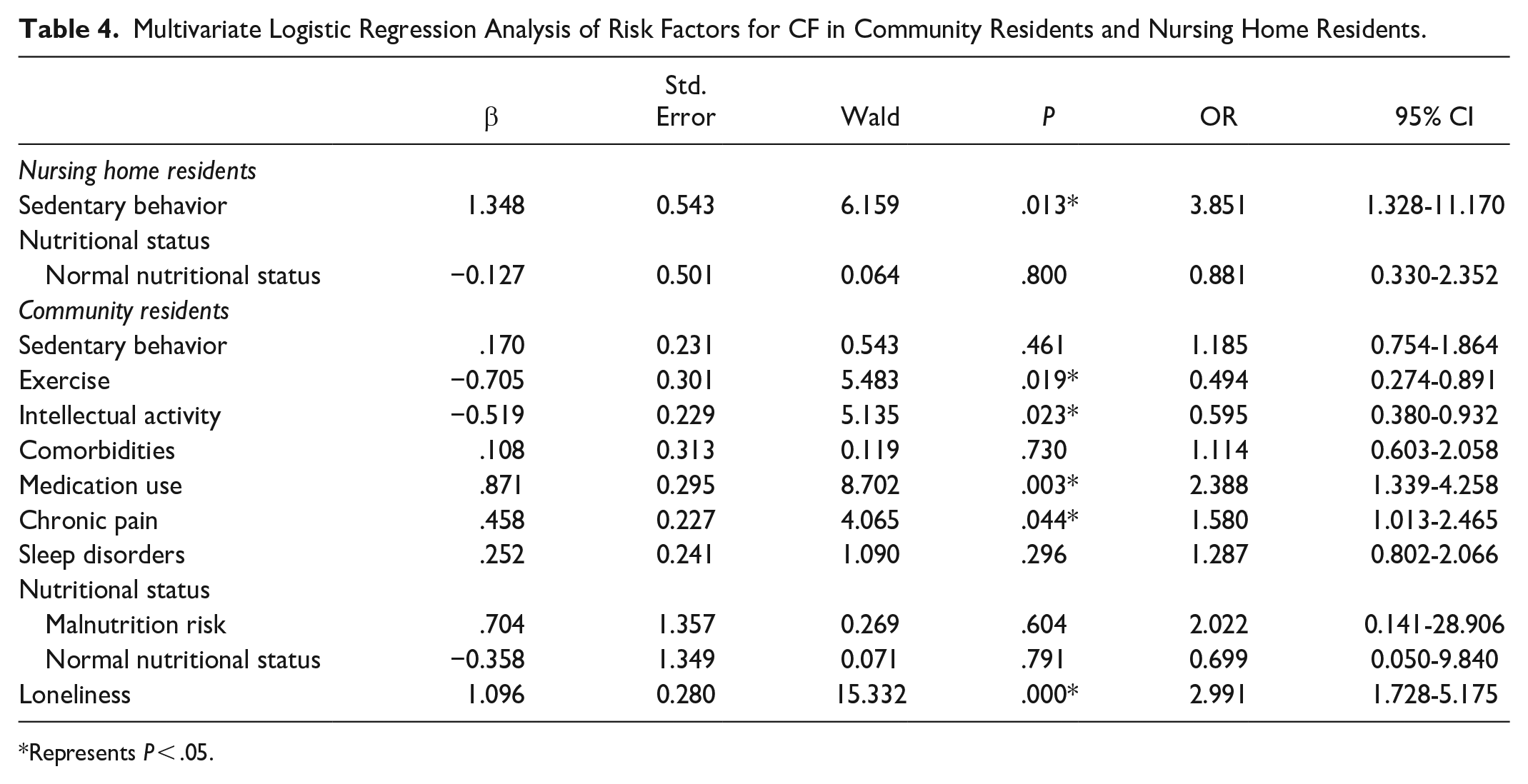
The results from the multivariate logistic regression analysis indicated that sedentary behavior (P = .013, OR = 3.851, 95% CI: 1.328-11.170) was the only risk factor for CF among nursing home residents. Among community residents, exercise (P = .019, OR = 0.494, 95% CI: 0.274-0.891) and intellectual activity (P = .023, OR = 0.595, 95% CI: 0.380-0.932) protected against CF, and medication use (P = .003, OR = 2.388, 95% CI: 1.339-4.258), chronic pain (P = .044, OR = 1.580, 95% CI: 1.013-2.465) and loneliness (P = .044, OR = 2.991, 95% CI: 1.728-5.175) increased the risk of CF (Table 4). Therefore, these 2 groups did differ in common modifiable risk factors for CF. Compared with nursing home residents, many common risk factors of CF in community residents could be obtained.
Multivariate Logistic Regression Analysis of Risk Factors for CF in Community Residents and Nursing Home Residents.
Represents P < .05.
Discussion
To determine the relationship between institutional residence and CF, our study first explored the selections of residence models and attitudes toward institutional residence among community residents over 50 years old. The results suggested that most community residents preferred to live independently (the family and community models) and had a negative attitude toward institutional residence.
There are 2 possible reasons for this aversion: on the one hand, this can be attributed to the deep-rooted influence of traditional Chinese cultural values, such as filial piety 36 ; on the other hand, negative feelings toward institutional residence are widespread among older people due to their high costs, associated feelings of abandonment by family members, intense feelings of loneliness, and increased risks of depression and even suicidal ideation. 29 However, with societal development, institutions have improved, including their facilities, services, living environment, and local transportation options. To meet the different health needs of older individuals, institutions have become increasingly diverse. For example, institutions can accommodate older people in need of medical care who are often bedridden or unable to take care of themselves due to illness. In contrast, other institutions resemble retirement homes for healthy older people. Nursing home residents who participated in our study resided such retirement homes and held a positive attitude toward living in institutions; most of these participants were single older individuals. With population aging, there will be a significant increase in older individuals living in institutions.
After establishing that most individuals would prefer not to live in a nursing home (despite the potential benefits of institutional residence, we examined the relationship between institutional residence and CF. Common modifiable risk factors for CF were compared between community residents and nursing home residents. Nursing home residents were only found to exhibit one risk factor for CF, sedentary behavior, but numerous risk factors for CF were found among community residents, including less exercise and intellectual activity, medication use, chronic pain, and loneliness (Table 4). Recent studies have found a strong relationship between sedentary behavior, PF, and cognitive impairment among older people, but most studies have been performed in community-dwelling populations.37 -39 Our study highlighted that sedentary behavior was significantly related to CF in only nursing home residents, not community residents. A possible explanation is that older community-dwelling adults in China (before and after retirement) have very busy lives, especially contributing to taking care of their grandchildren. In contrast, nursing home residents are separated from their original family life, and are more likely to exhibit sedentary behavior, especially older people with CF.
Aligning with the findings of many other studies on CF,9,40 -42 our findings suggest that exercise and intellectual activity protected against CF in community residents. In nursing homes, residents were scheduled to regularly engage in physical exercises, such as walking and dancing, and some simple intellectual activities, such as playing mahjong and cards. In contrast, most older community-dwelling adults (before and after retirement) are not aware of how to schedule their daily lives effectively, even though they know including such activities is good for their health. Therefore, community residents are more likely to feel lonely than nursing home residents. Additionally, as their children grow up and start their own families, older community-dwelling adults may feel increasingly lonely. Loneliness has a negative impact on physical and cognitive function.43,44 We did not observe loneliness in nursing home residents, perhaps because their daily lives were filled with effective and reasonable activities or because they remained close with their families, as shown in Figure 4.
Additionally, we found that medication use and chronic pain were significantly associated with CF in community residents. With population aging, an increasing number of older people suffer from chronic pain due to a variety of chronic diseases, such as diabetes and heart disease; thus, they need to take one or more drugs. 45 Drug therapy often limits physical function46,47 and affects cognitive function. 48 However, older people in nursing homes have professional doctors and nurses that perform regular check-ups, help them to take appropriate medicine, and engage in moderate physical and intellectual activities.
Our findings reveal the prevalence of CF in 2 samples of adults over 50 years old: community residents and nursing home residents. The prevalence of CF was 14.20% in community residents and 49.07% in long-term nursing home residents. It is obvious that the prevalence of CF is much higher among people in nursing homes,15,16,49 probably because of some uncontrollable risk factors for CF, including older age, female sex, low personal income, and lower education levels, which were not target variables in our study.
The limitations of this study are as follows. First, we utilized a cross-sectional design to assess the relationship between institutional residence and CF. There are a lot of confounding factors that could affect the results, and of course the conclusions can be affected. For example, the age and sex ratios of the 2 samples are not at the same level. Further longitudinal follow-up and well-designed studies are needed to confirm the present findings. Second, the sample size could be expanded to further verify the conclusions. Finally, if nationally representative samples were available, these data could confirm the validity of our research conclusions.
Conclusion
Although institutional residence is becoming more common, only a small proportion of older people (before and after retirement) voluntarily considered institutional residence. Our findings suggest that compared to living in the community, living in a nursing home can effectively address many common risk factors for CF, including lack of exercise and intellectual activity, medication use, chronic pain, and loneliness. Thus, institutional residence is conducive to the intervention of CF. Further studies about whether the daily life of nursing home residents can control the common risk factors for CF are needed to confirm this conclusion.
Supplemental Material
sj-docx-1-inq-10.1177_00469580231220180 – Supplemental material for Institutional Residence Protects Against Cognitive Frailty: A Cross-Sectional Study
Supplemental material, sj-docx-1-inq-10.1177_00469580231220180 for Institutional Residence Protects Against Cognitive Frailty: A Cross-Sectional Study by Jin Hua Huang, Qing Song Wang, Rui Min Zhuo, Xin Yu Su, Qing Yuan Xu, Yu Hao Jiang, Yu Han Li, Song Bai Li, Lan Lan Yang, Rui Wen Zang, Chen Yang Meng and Xue Chun Liu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-2-inq-10.1177_00469580231220180 – Supplemental material for Institutional Residence Protects Against Cognitive Frailty: A Cross-Sectional Study
Supplemental material, sj-docx-2-inq-10.1177_00469580231220180 for Institutional Residence Protects Against Cognitive Frailty: A Cross-Sectional Study by Jin Hua Huang, Qing Song Wang, Rui Min Zhuo, Xin Yu Su, Qing Yuan Xu, Yu Hao Jiang, Yu Han Li, Song Bai Li, Lan Lan Yang, Rui Wen Zang, Chen Yang Meng and Xue Chun Liu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-3-inq-10.1177_00469580231220180 – Supplemental material for Institutional Residence Protects Against Cognitive Frailty: A Cross-Sectional Study
Supplemental material, sj-docx-3-inq-10.1177_00469580231220180 for Institutional Residence Protects Against Cognitive Frailty: A Cross-Sectional Study by Jin Hua Huang, Qing Song Wang, Rui Min Zhuo, Xin Yu Su, Qing Yuan Xu, Yu Hao Jiang, Yu Han Li, Song Bai Li, Lan Lan Yang, Rui Wen Zang, Chen Yang Meng and Xue Chun Liu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
Not applicable.
Abbreviations
CF, cognitive frailty; PF, physical frailty; MCI, mild cognitive impairment; MoCA, Montreal Cognitive Assessment; PSQI, Pittsburgh Sleep Quality Index; BMI, body mass index; and MNA-SF, Mini Nutritional Assessment-Short Form.
Author Contributions
J.H.H. and Q.S.W. were responsible for study conception and design. J.H.H. interpreted the data. R.M.Z., X.Y.S., Q.Y.X., Y.H.J., Y.H.L., S.B.L., L.L.Y., R.W.Z., and C.Y.M. prepared the figures and tables. J.H.H. wrote the first draft of the manuscript, interpreted the data, and wrote the final version. All authors critically revised the article for important intellectual content and read and approved the final version.
Availability of Data and Materials
The datasets generated and analyzed during the current study are not publicly available but are available from the corresponding author upon reasonable request.
Consent for Publication
Not applicable.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Project of Natural Science Research of Anhui Province (KJ2021A1229), the Innovation Training Program (S202113618002), University-level Quality Engineering from Clinical College of Anhui Medical University: First-class Professional Cultivation Point: Clinical Medicine (2020XJ003), the Key Research and Development Plan of Anhui Province (2022e07020029) and grants from the National Key Research and Development Program of China (2016YFC1305900).
Ethics Approval and Consent to Participate
The study was approved by the Institutional Review and Ethics Committee of Anhui Medical University, and all participants provided written informed consent to participate in this study, which was performed in accordance with relevant guidelines and regulations.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.