
Abstract
Noncommunicable chronic diseases among the elderly population represent a significant economic burden in China. However, previous disease-related health cost studies lacked representation of older adults and comparability of the burden of multiple chronic diseases. The objective of this study was to determine the fraction of health care costs attributable to the 6 most prevalent chronic diseases and comorbidities in the sample of older adults. This study employed data from the Chinese Longitudinal Healthy Longevity Survey (CLHLS), with 3 waves in 2011, 2014, and 2018, and included 18 349 observations in total. Outpatient costs, inpatient costs, and total health care costs were included in this study. Based on a 2-part random effects model, the effect of chronic disease on health service utilization was first explored by constructing a dummy variable for whether or not to utilize health care, followed by estimation of attributable costs in the population with health care utilization. Among the older adults in the sample, hypertension, heart disease, cataracts, arthritis, stroke or Cerebrovascular disease (CVD) and chronic lung disease are the 6 most prevalent chronic conditions. The costs attributable to the 6 chronic diseases mentioned above were 36.00% of outpatient costs, 55.92% of inpatient costs, and 45.05% of total health care costs for older adults. Of these, heart disease, stroke or CVD, and chronic lung disease accounted for 22.11%, 13.24%, and 10.56% of total health care costs, respectively. Moreover, the proportion of health care costs attributable to chronic diseases was higher for older adults who were male, lived in urban areas, and had a lower level of education. The proportion of health care costs attributable to chronic diseases is substantial among older adults in China. Health care costs associated with chronic diseases can be decreased with well-targeted interventions and comprehensive access to health services.
Patients with chronic diseases have higher health care expenditures than those without chronic disease.
The findings of this study make 3 contributions to the financial burden of chronic disease treatment for older adults in China. First, we selected the 6 most prevalent chronic diseases among older adults nationwide and estimated the likelihood for outpatient or inpatient service utilization for chronic disease treatment. In addition, we provide estimates of cost fractions attributable to chronic conditions at the individual level. Finally, we analyze the costs attributable to chronic conditions among older adults based on gender, educational attainment, and rural-urban differences.
By estimating healthcare utilization and cost fractions for chronic disease treatment, as well as heterogeneity analysis of individual characteristics, our findings provide foundational data for the design and development of health insurance coverage, health care policy development, and implementation to address the rising costs of chronic disease treatment.
Introduction
From a global perspective, the aging of the population and the changes of the disease spectrum have resulted in an ongoing increase in demand for health services and have significantly impacted social and economic growth.1,2 On the one hand, the demographic structure is evolving as a consequence of the rapid expansion of social economy, and all nations face the challenge of aging to varying degrees. The seventh national census of China, released by the National Bureau of Statistics of China in May 2021, revealed that 18.7% of the population is over 60 years old, and 13.5% is over 65. 3 The growth of the elderly population has been accompanied by a substantial escalation in healthcare spending, which has surged from 458.66 billion CNY in 2000 to 5259.83 billion CNY in 2017, representing a nearly 10.47-fold increase. 4 More than a quarter of the total medical expenses were incurred by the elderly. 5 This indicated that the financial burden of health care for the older people is much greater than for other groups, exacerbating the burden of social development in China, which is “growing old before becoming wealthy.”
On the other hand, aging is a significant contributor to the majority of non-communicable chronic diseases, including cardiovascular diseases, chronic respiratory diseases and tumors, among others.6 -8 According to estimates, by the end of 2019, out of 254 million older people in China, approximately 120 million older adults suffer from chronic diseases, and 40.63 million older adults are paralyzed or partially disabled. 9 This places a heavy financial burden on individuals and their families. The study on population aging and economic burden in developed countries found that the per capita total medical cost of the United States would increase from 2093 USD in 2000 to 3543 USD in 2050 due to population aging, with kidney disease, heart and vascular disease, and urinary system disease experiencing the greatest cost increases. 10 The similar pattern is observed in developing countries. Chronic diseases account for 63.96% of the total personal medical costs incurred by senior citizens in rural China. Chronic diseases can increase the rate of healthcare utilization by 1.74 times and the annual medical expenditure per capita by 88% in comparison to those without chronic diseases. 11 Moreover, the prevalence of chronic diseases among the older population living in urban areas is 79.1%, and the medical expenditure per capita related to chronic diseases in the previous 6 months was 4656 CNY. 12
In addition to exacerbating poverty for patients and their families, the prevalence of NCDs among older adults poses a substantial threat to national development and economic growth. China’s participation rate in basic medical insurance is currently stabilized at above 95%. 13 Increased insurance coverage increases the utilization and cost of health care for older adults.14,15 This implies that the national health care system is sharing the rising cost of health care for the elderly.16,17 China has built a multi-level medical security system, with different types of health insurance for different groups of population. These include publicly funded medical care, urban employee basic medical insurance, and urban resident basic medical insurance, etc. 18 Different types of insurance have different effects on health care expenditures of older adults, as well as varying reimbursement rates and scopes.19,20 As a result, we selected total health care costs for the study, which will more accurately reflect an individual’s actual health care utilization than out-of-pocket or reimbursed costs.
The World Health Organization (WHO) devised a 15-year plan to reduce NCDs in 2011 chronic for the prevention and treatment of NCDs. 21 China has released policies such as the Healthy China 2030 Plan and Recommendations, 22 and China’s Medium-to-Long Term Plan for the Prevention and Treatment of Chronic Diseases (2017-2025) 23 since 2016, which aim to reduce the prevalence of chronic diseases as well as the cost of treatment. However, there is still a lack of cost estimates and specific policy documents on the prevention and treatment of chronic diseases with a high prevalence among the elderly, such as cardiovascular disease and chronic obstructive pulmonary disease. 24 Numerous studies have evaluated the impact of different chronic diseases on health care utilization or costs in an effort to quantify the health and economic burden of chronic diseases.25 -29 Existing studies, however, lack representation of the older populations and do not allow for intuitive diseases comparisons due to differences in study populations, timing, and methodologies.11,20,30 Consequently, the data from a longitudinal survey of the older person were utilized in this study. The prevalence of chronic diseases among the elderly was first determined. Then, the 6 most prevalent chronic diseases, including hypertension, arthritis, heart disease, cataracts, chronic lung disease, and stroke or cerebrovascular disease (CVD) were selected for the analysis of the effect of chronic disease on health care utilization and costs. Due to the consistency of the study population and the identification of the disease, we can assess the severity of the economic burden of different chronic diseases in the older adults with greater precision.
In summary, this study aimed to analyze the effects of chronic diseases on the utilization of inpatient services, outpatient services, and total health care services among the older people, considering both single chronic diseases and chronic comorbidities. Furthermore, the costs of health care for the older people attributable to specific chronic diseases and comorbidities were estimated. This has significant implications for policymakers endeavoring to understand which chronic diseases and categories of costs are the primary drivers of health care costs.
Methods
Study Design and Population
The data utilized in this study came from the Chinese Longitudinal Healthy Longevity Survey (CLHLS), an ongoing, open cohort study of the older adults conducted jointly by Peking University Center for Healthy Aging and Development and National Development Institute. The survey collected health-related information on Chinese seniors aged 65 and older in 23 provinces in China, including socio-demographic characteristics, socioeconomic status, cognitive function, lifestyle, health status, and health care utilization. The purpose of the survey is to explore the factors related to the health and longevity of the Chinese population. Details of CLHLS can be accessed elsewhere. 31
The CLHLS baseline survey was conducted in 1998, followed by 2000, 2002, 2005, 2008, 2011, 2014, and 2018. The survey content regarding health care cost varied in different waves. From 1998 to 2008, only the total health care costs of respondents in the previous year were collected. After 2011, both outpatient and inpatient costs were collected. The study examined, from the viewpoints of outpatient, inpatient, and total health care services, the impact of different chronic diseases on the health care utilization and costs among the older adults.
Therefore, we selected a sample of older adults surveyed during the most recent 3 waves of CLHLS (2011, 2014, and 2018). 18 349 observations were used for analysis after removing missing values and outliers for key variables.
Health Care Utilisation and Costs
Individual-level health care costs are the total cost to the individual, that is, the sum of reimbursement from health care insurance and out-of-pocket costs. Outpatient costs are characterized by the question: “How much did you spend on outpatient costs last year?” These costs included consultation fees, medication purchases, outpatient laboratory tests and treatment. The question “How much did you spend on inpatient costs last year?” referred to inpatient costs, which included the costs of bed tariffs, laboratory tests, medication, treatment, and care. The total cost of health care is the aggregate of outpatient and inpatient costs. Costs were adjusted on the basis of the medical consumer price index and expressed in Chinese Yuan (CNY) for 2018. 32 The exchange rate between USD and CNY on December 3, 2018, was: 1.0 USD = 6.8974 CNY. Due to the extremely skewed distribution of the medical cost data, it was logarithmically transformed.
We created dummy variables for whether individual utilized health care services based on their health care costs, including whether they used outpatient services (an indicator of positive outpatient costs), inpatient services (an indicator of positive inpatient costs), and health care services (an indicator of positive health care costs).
Chronic Disease
We selected the top 6 chronic diseases with the highest prevalence in our sample, including Hypertension, Arthritis, Heart disease, Cataracts, Chronic lung disease (bronchitis or emphysema or asthma or pneumonia), and Stroke or Cerebrovascular disease (CVD) to conduct cost attribution analysis. In this study, the primary explanatory variables were the dummy variables for these 6 chronic diseases (1 indicates having the chronic disease, 2 indicates not having the chronic disease).
Covariates
Referring to existing studies,11,33,34 we controlled for a number of variables that influence the utilization and cost of health care services for the older adults, including age, gender (male = 0, female = 1), residence (rural = 0, urban = 1), education level (primary and below = 0, middle and above = 1), marital status (other = 0, cohabited = 1), health insurance coverage (no = 0, yes = 1), comorbidity (no = 0, yes = 1), smoking status (none = 1, quit = 2, still = 3), drinking status (none = 1, quit = 2, still = 3), body mass index (BMI) (underweight = 1, normal weight = 2, overweight = 3, obesity = 4), activities of daily living (ADL) score, annual household income per capita.
The educational level was categorized into 2 groups according to the years of education, primary and below (≤6 years) and middle and above (>6 years); The comorbidity refers to the presence of 2 or more chronic diseases; BMI was determined as the weight in kilograms divided by the height in meters squared, kg/m2. The guidelines for prevention and control of overweight and obesity in Chinese adults was utilized as the BMI criteria in the study. 35 It was specifically divided into 4 categories: underweight (<18.5 kg/m2), normal weight (18.5-23.9 kg/m2), overweight (24.0-27.9 kg/m2) and obesity (≥28.0 kg/m2); The ADL scale is one of the most widely used instruments for evaluating the ability to perform activities of daily living, and the items evaluated include 1) Bathing, 2) Dressing, 3) Toilet, 4) Indoor Transfer, 5) Continence, and 6) Eating. 36 Each item is categorized as either 0 (Completely independent) or 1 (Needs help). The total ADL score ranged from 0 to 6, with greater values indicating more restricted activities of daily living.
Statistical Analyses
First, descriptive statistics were employed to compare the basic characteristics of participants across years. Frequency/percentage and mean/standard deviation (SD) were utilized to characterize categorical and continuous variables, respectively.
Then, to further analyze the impact of chronic diseases on health care costs of the older adults, we referred to studies on the impact of smoking 37 or obesity 38 on health care costs and developed the following 2-part random effects model to evaluate the impact of chronic diseases on health care utilization and cost in older adults.
Equation (1) investigates the impact of chronic disease on health care utilization among older adults, and equation (2) explores the impact of chronic disease on health care costs among older adults.
We used the parameters in equations (1) and (2) to predict health care costs in both the presence and absence of chronic disease scenarios. Referring to the existing studies38,39 first, the estimated parameters were utilized to predict the annual per capita health care cost of the older adults based on the actual situation, as an actual value (
It should be further noted that the equations can be used to predict the costs attributable to a specific chronic disease using the estimated coefficients for only one chronic disease, or they can be combined with the estimated coefficients for all chronic diseases to predict the total costs attributable to the 6 chronic diseases.
Additionally, we performed a robustness analysis. To better control for unobservable factors that do not vary over time but may influence individual health care costs, we selected participants who were surveyed in all 3 waves from the available sample to create a balanced panel data. And, based on this, we conducted equations (1) and (2) to obtain the estimation results (See Supplemental Tables). After comparing the 2 estimates, we found that there is no significant change in the main findings despite a slight change in magnitude. The effect of chronic conditions on health care utilization and health care costs, as well as the cost fraction attributable to chronic conditions, have not changed significantly. Comparison of the robustness analysis results and main results further demonstrates the robustness of the estimation.
The p-value < .1 could be identified as statistical significance. All data were compiled and analyzed using STATA version 16.0 (Stata Corp, College Station, TX, USA).
Results
Characteristics of Participants
A total of 18 349 observations, including 6222 observations in 2011, 4261 observations in 2014, and 7866 observations in 2018 were analyzed. In 2018, the prevalence of hypertension, heart disease, cataract, arthritis, Stroke or CVD and chronic lung disease were 41.20%, 16.59%, 13.88%, 13.31%, 10.70%, and 10.54%, respectively. As the chronic disease with the highest prevalence, the prevalence of hypertension in the 3 waves were 29.01%, 32.86%, and 41.20%, respectively. Participants in the baseline survey had an average age of 84.44 (standard deviation, 10.79) years, and 47.97% were male (Table 1).
Descriptive Statistics of Study Sample, CLHLS, 2011, 2014, and 2018.

Cohabited covers married and cohabitating.
Other covers single, separated, divorce, and widowed.
The Effect of Chronic Diseases on Health Care Utilisation and Costs Among the Older Adults in the Sample
After controlling for other factors influencing health care utilization and cost in older adults, the results of the 2-part model indicated that compared to their counterparts, older adults with hypertension (OR = 1.595, P < .01), arthritis (OR = 1.487, P < .01), heart disease (OR = 2.254, P < .01), cataracts (OR = 1.173, P < .01), chronic lung disease (OR = 2.174, P < .01), stroke or CVD (OR = 1.816, P < .01) have significantly higher health care utilization; Among older adults who utilized health care services, hypertension (β = .105, P < .01), heart disease (β = .644, P < .01), chronic lung disease (β = .429, P < .01), stroke or CVD (β = .562, P < .01) are associated with increased health care costs. However, there was no statistically significance between arthritis, cataracts (P > .05) and health care costs (Table 2).
Parameter Estimates and Test Statistics, CLHLS, 2011, 2014, and 2018.

Note. All subsample results are based on 2-part model. Chronic diseases were used as independent variables, and the availability of medical care and health care costs were used as dependent variables, respectively.
Annual health care costs are the natural counterpart of actual costs.
Including age, BMI, education level, residence, gender, activities of daily living score, marital status, drinking status, smoking status, health insurance coverage, annual household income per capita.
P < .01. *P < .1.
Based on the breakdown analysis of outcomes for both outpatient and inpatient settings. There exists a positive correlation between the presence of 6 chronic diseases and the utilization and associated costs of outpatient services among older adults, albeit to various extents. The presence of heart disease (OR = 1.709, P < .01), chronic lung disease (OR = 1.843, P < .01), stroke or CVD (OR = 1.984, P < .01) was found to be associated with higher utilization of inpatient services. Furthermore, heart disease (β = .577, P < .01), chronic lung disease (β = .255, P < .01), stroke or CVD (β = .379, P < .01) were significantly associated with increased hospitalization costs for older adults.
Predictions of Health Care Costs
Overall, the total CDAF is 45.05%. With the exception of arthritis and cataracts (which are not statistically significant in the health care costs model outlined in Table 2), the chronic diseases ranked in descending order of their CDAF were heart disease, stroke or CVD, chronic lung disease, and hypertension. Annual per capita health care costs attributable to heart disease amount to 386.456 CNY, with a CDAF of 22.11%; Similarly, the annual per capita health care costs attributable to stroke or CVD are 231.498 CNY, with a CDAF of 13.24%; Chronic lung disease incurs annual per capita health care costs of 184.544 CNY, with a CDAF of 10.56% (Panel A in Table 3).
Estimated Personal Medical Cost Attributed to Chronic Disease (CNY).
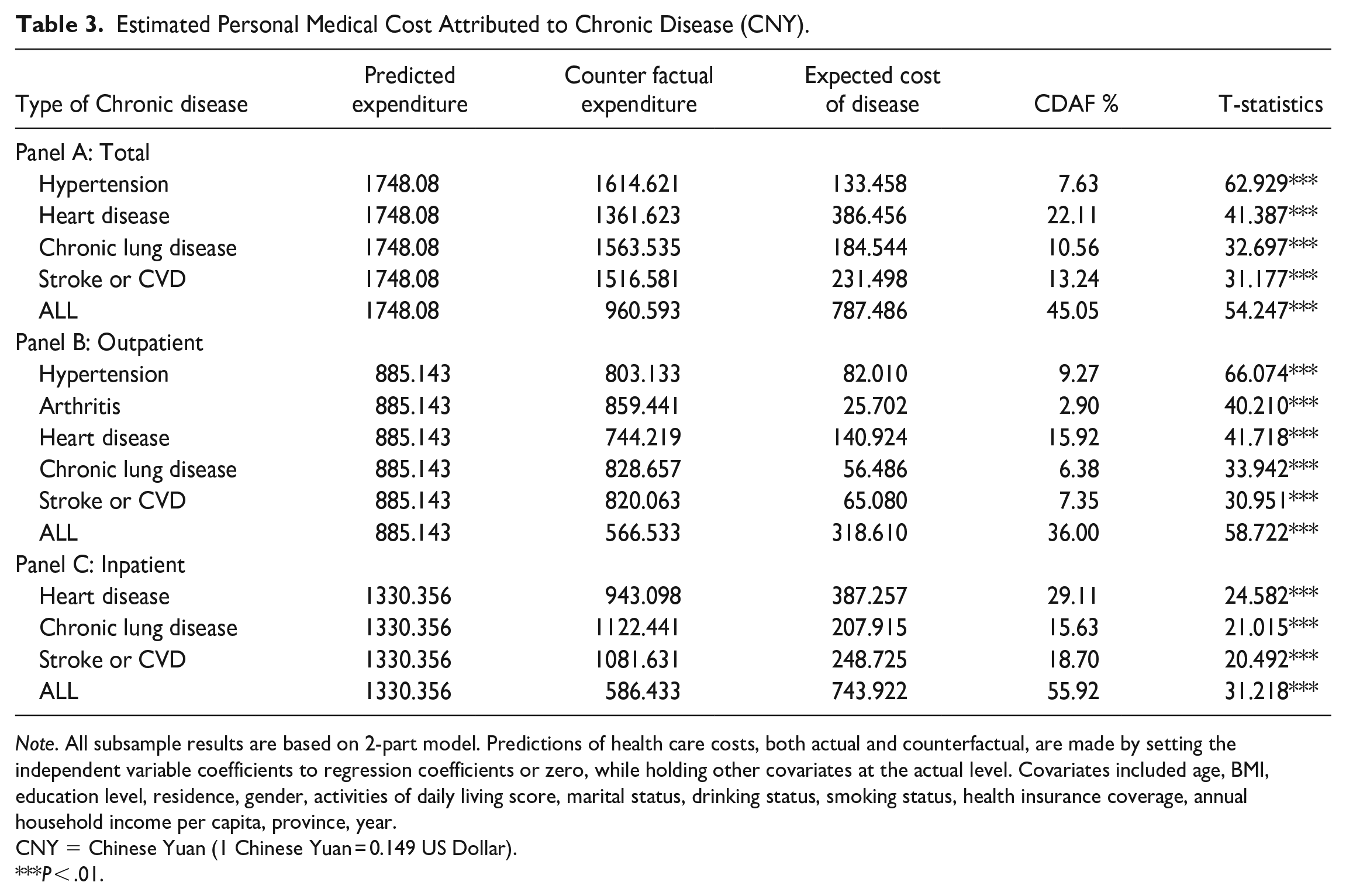
Note. All subsample results are based on 2-part model. Predictions of health care costs, both actual and counterfactual, are made by setting the independent variable coefficients to regression coefficients or zero, while holding other covariates at the actual level. Covariates included age, BMI, education level, residence, gender, activities of daily living score, marital status, drinking status, smoking status, health insurance coverage, annual household income per capita, province, year.
CNY = Chinese Yuan (1 Chinese Yuan = 0.149 US Dollar).
P < .01.
The breakdown analysis of the outpatient costs is presented in Panel B of Table 3. Chronic diseases accounted for 36.00% of the total outpatient costs for older adults. Among them, the CDAF prioritized heart disease, hypertension, chronic lung disease, and stroke or CVD as the most significant conditions. The outpatient CDAF of heart disease was 15.92%. The annual per capita outpatient costs of the older adults would fall by 140.924 CNY if heart disease were absent and all other characteristics remained unchanged. The CDAF of hypertension outpatient costs was 9.27%, and the annual per capita outpatient costs attributable to hypertension was 82.010 CNY, which was significantly greater than chronic lung disease, stroke or CVD.
Analysis of hospitalization revealed that the CDAF for hospitalization costs owing to heart disease was 29.11%, and the annual hospitalization costs per capita attributable to heart disease was 387.257 CNY. The CDAF of stroke or CVD was 18.70%, and the annual hospitalization cost per capita was 248.725 CNY. Furthermore, 15.63% hospitalization costs were attributable to chronic lung disease, resulting in an rise of 207.915 CNY per capita in annual hospitalization costs (Panel C in Table 3).
Results of Heterogeneity Analysis
To further examine differences in health care costs attributable to chronic diseases among the older adults by gender, education level, and place of residence, we separated the sample into groups based on a variety of characteristics and utilized the same calculation procedure mentioned previously. Health care costs attributed to chronic diseases among older individuals with various characteristics were estimated. The results were shown in Figure 1.

The heterogeneity analysis of health care cost attributable to chronic diseases.
Overall, there was a higher proportion of health care costs attributable to chronic disease among males, individuals with a secondary education and above, and residents living in urban areas, regardless of outpatient, inpatient, or total health care costs. Specifically, females had a greater proportion of costs attributed to heart disease and arthritis than males; Older adults with a primary education or below displayed a higher proportion of costs attributable to chronic lung disease in comparison to individuals with a higher level of education.
Discussion
Chronic diseases have emerged as a substantial economic burden among the older population in China. The findings of this study indicated that chronic diseases significantly increase the utilization of outpatient and inpatient services among older adults, with their attributable health care costs accounting for approximately 50% of the total costs. Moreover, it is worth noting that males, individuals with a higher education level, and those residing in urban areas incurred a greater proportion of health care costs for chronic conditions.
Regarding specific chronic conditions, hypertension exhibits the highest prevalence, necessitating long-term medications for blood pressure control. 40 Consequently, the majority of its health care costs were attributed to outpatient services; the CDAF for outpatient costs among the older adults in the sample is 9.27%. In addition, as a result of the characteristics of hypertension needing long-term maintenance and the limited disease management abilities of the older adults, 41 the course of hypertension is prolonged, leading to an increase in health care costs, with a CDAF of 7.63%. Many studies have demonstrated that the low rate of hypertension control is the leading cause of its high prevalence and significant health care costs.42 -45 Improving the effectiveness of self-management for hypertensive patients is the focus of the current intervention. Heart disease, stroke or CVD, and chronic lung disease accounted for 22.11%, 13.24%, and 10.56% of total health care costs, respectively. The majority of the costs attributable to stroke or CVD and chronic lung disease were associated with hospitalization. Despite the fact that many chronic diseases can be prevented and managed with daily medication, they carry the risk of acute aggravation and severe results, including stroke, cerebral infarction, asthma, COPD. Consequently, hospitalization is necessary in such cases. In the case of asthma treatment, for example, it is evident that there are differences between China and the United States. The United States is more inclined to limit the risk of acute exacerbation by employing short-acting drugs over an extended period.34,46 Conversely, older adults in China has insufficient self-management skills, leading them to choose for treatment during the acute stage. In accordance with previous research,47,48 the majority of health care costs associated with brain diseases were found in hospitalizations. More than one-third of the total hospitalization expenditures were attributable to the costs of stroke-related inpatient medications. 47 For stroke or cerebrovascular disease and chronic lung disease, acute exacerbation prevention is more important.
Heart disease accounted for the largest proportion of health care costs among older adults (CDAF = 29.11%), and its CDAF is the highest for both outpatient costs (15.92%) and inpatient costs (22.11%). This posed a substantial financial burden for both patients and health care systems. Consistent with previous studies, 49 there is a positive correlation between the increasing prevalence of heart disease and the corresponding rise in hospitalization rates, predominantly attributed to acute exacerbations necessitating short-term therapeutic interventions. Moreover, heart disease is often accompanied by various complications. For instance, hypertension is a major risk factor for heart disease,50,51 and the treatment of heart disease frequently often leads to increased health care costs for blood pressure control, oral disease therapy, blood glucose and lipid control.52,53 Outpatient costs linked to heart disease increased with the treatment of comorbidities and medications for heart disease. Consequently, preventing underlying illnesses and minimizing the risk of acute exacerbation is necessary to reduce the enormous health loss and economic burden associated with heart disease.
The findings of the heterogeneity analysis revealed that urban older adults have a greater proportion of chronic health care costs compared to their rural counterparts, which is consistent with previous research findings.30,54,55 Due to the relatively lower income, rural older adults has a lower rate of health care service consumption. Combined with the lack of medical resources, diseases are frequently inadequately diagnosed and treated. Consequently, chronic health care for the older adults in rural areas is less expensive, but they experience a higher prevalence of severe injuries. 11 It is imperative to consider gender disparities in the context of chronic illnesses. Women have a higher risk of cardiovascular disease, whereas men demonstrate a greater prevalence of cerebrovascular disease, owing to inherent physiological distinctions. Differences in the response of sex hormones to medications and therapies contributed to variations in disease progression and exacerbation, as well as the burden of disability and mortality.56 -58 These gender disparities are also seen in individuals with chronic lung disease and chronic kidney disease.59 -61 This may explain why the economic and mortality burdens of the same disease are different for older persons of different genders. Therefore, it is imperative to acknowledge gender disparities in the prevention and management of chronic illnesses, as tailored interventions have the potential to yield superior outcomes.
The findings of this study underscore 2 components in light of prevailing policies. There is a need to make moderate enhancements to reimbursement policies for older persons afflicted with diseases that incur substantial outpatient or inpatient expenses. This measure aims to alleviate the economic strain experienced by patients and their families. Also, there is a need to enhance the implementation of health promotion policies targeting chronic diseases in the elderly population, with the aim of fostering better habits and facilitating the adoption of positive behavioral modifications among older individuals. Specifically: 1) Lifestyle: smoking, alcohol consumption, an unhealthy diet and lack of physical activity are modifiable risk factors for various chronic diseases; 62 The adoption of a healthy lifestyle, preferably initiated at a younger age, can effectively reduce the risk of chronic diseases in older people; 2) Disease management: Enhancing medication adherence among the older adults is an effective intervention that can alleviate and improve the symptoms of most chronic diseases and lower the likelihood of acute exacerbations. If necessary, artificial intelligence, remote monitoring and other technologies can be applied to enhance the capacity for drug management;63,643) Social support: the assistance and guidance of family members, peers and medical staff has a positive effect on patients’ long-term self-care, increasing patients’ self-regulation abilities and self-efficacy; 65 4) The medical care system can contribute significantly to the management of chronic diseases by implementing a comprehensive 3-level prevention strategy. This strategy involves enhancing the coverage and acceptance of primary health care services, establishing support systems for chronic diseases within communities and villages, improving the overall process of chronic disease management, and leveraging modern internet technology to augment medical resources in underdeveloped regions. 66 In addition, the influence of sociodemographic and economic factors, particularly gender differences, should be considered throughout the entire process of prevention and treatment of chronic diseases.
Strength and Limitation
The strength of this study is that we employed a longitudinal dataset for older adults to explore health care costs attributable to the 6 most prevalent chronic conditions in the sample. Furthermore, differences in costs attributed to chronic diseases were analyzed and compared across subgroups of the older adults. The findings of this study would offer valuable insights into disease prevention and treatment as well as potential avenues for improving the quality of life among the older adults.
There are several limitations to this study. First, because the data for this study were obtained from public databases, some diseases (eg, stroke and cerebrovascular disease) were grouped together. In contrast to previous studies on specific diseases, the findings of this study do not provide sufficient evidence for a clear distinction between the 2 CDAFs, and it is challenging to conduct a comprehensive comparison with prior studies focusing on specific diseases. The second limitation is the emphasis placed on the older adult population. Our study population was limited to a sample of surviving older adults, and deceased older adults were not included in our study sample, which could introduce potential estimation bias. Nevertheless, the findings from the balanced panel data validate the robustness of main results. Third, the study’s findings may be limited in their generalizability due to the reduction in sample size caused by the absence of crucial variables and the inability to include weighting variables for weighted analysis. Fourth, standard diagnostic procedures for chronic diseases were not implemented in the survey. The prevalence of chronic diseases is self-reported by participants, which may differ from the actual situation. Lastly, individual-level health care costs are self-reported by participants and thus may be susceptible to recall bias.
Conclusions
The proportion of outpatient costs, inpatient costs, and total health care costs attributable to the 6 most prevalent chronic disease comorbidities among older adults in the study were 36.00%, 55.92%, and 45.05%, respectively. The evidence suggests that chronic diseases impose a substantial economic burden. The proportion of health care costs attributable to chronic diseases was greater among males, older adults living in urban areas, and those with a higher level of education. The reduction of health care costs attributable to chronic diseases can be achieved through well-targeted interventions and broad access to health services. The study emphasized the importance of disease management and self-efficacy in the prevention and treatment of chronic diseases among the older adults. The information provided plays a crucial role in determining the planning decisions and resource allocation for efforts related to the prevention and management of chronic diseases.
Supplemental Material
sj-DOC-1-inq-10.1177_00469580231214469 – Supplemental material for Individual-Level Health Care Costs Attributable to Noncommunicable Diseases: A Longitudinal Study Based on the Older Adults in China
Supplemental material, sj-DOC-1-inq-10.1177_00469580231214469 for Individual-Level Health Care Costs Attributable to Noncommunicable Diseases: A Longitudinal Study Based on the Older Adults in China by Shi-qi Zhao, Li-ping Zhao, Xin-peng Xu and Hua You in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors appreciate the participants and staff involved in the data collection and management in the Chinese Longitudinal Healthy Longevity Survey (CLHLS).
Author Contributions
HY and XPX designed the study and critically reviewed, commented and revised important intellectual content. SQZ and LPZ performed the final statistical analyses and interpretation of data, and drafted the article. XPX revised the draft grammatical sentences.
List of Abbreviations
NCD: non-communicable diseases; CDAF: chronic disease attributable fraction; CLHLS: the Chinese Longitudinal Healthy Longevity Survey; CVD: Cerebrovascular disease; COPD: chronic obstructive pulmonary disease.
Availability of Data and Materials
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Cultivation Project of Decision-making Consultation, Institute of Healthy Jiangsu Development, Nanjing Medical University (7).
Disclaimers
All authors declare that the views expressed in the submitted articles are their own and not the official position of the institution or funder.
Ethics Approval and Consent to Participate
The biomedical ethics committee of Peking University approved the study (IRB00001052-13074), and all participants or their proxies provided written informed consent. All methods were carried out in accordance with relevant guidelines and regulations or Declaration of Helsinki.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.