
Abstract
The implications of population aging for economic growth is not only the shrinking working-age population, but also the increasing health care burden of the elderly population. It is difficult to explain clearly the relationship between a country’s aging population and its economy without considering health effects. Based on the Solow economic growth model, the aims of this study are to estimate the economic effects of the health care burden for elderly population, and to access whether reducing effective labor input for economic production. The analysis employs a set of econometric approaches including fixed effects, generalized method of moments, instrumental variable, and mediation regression analyses using a multinational multi-database covering the years 2000-2019. The empirical evidence indicates that the health care burden was negatively correlated with economic growth during the study period, with every 1% increase in the health care burden leading to a 0.083% decrease in the GDP growth rate. The results of heterogeneity analysis and mediating analysis further confirmed that worsening health in the elderly population could be associated with the deceleration in economic development through the indirect pathway that lowering the employment rate of working-age population. This study provides new empirical evidence on the economic impact of population aging that the poor health of elderly population can be one critical factor of limiting economic growth, for the reason the labor inputs in household production are likely crowded out by family caregiving.
As population aging is the predominant demographic phenomenon today, its potential risks and impacts on economic development have become a common major concern in countries worldwide.
This study proposes a new explanation for the economic impact of population aging from the health perspective: the working population may leave the labor market due to the burden of their parents’ health care, leading to reduce effective labor input for economic production.
The findings of this study help to propose policy recommendations that focusing on health promotion for the elderly population, enhancing employment protection for the working-age population, and increasing third-party care services provision.
Introduction
Many countries face significant challenges in their search for answers related to health care, work and retirement, and the burden of disease. The ongoing demographic transition to an aging society suggests that the simultaneously increasing number of elderly and retired people and shrinking scale of working-age people constitutes a long-term trend that may result in profound societal change. 1 Moreover, the health condition of a country’s population is critical for its macroeconomic performance. 2 Thus, the sustainability of economic development is an increasingly significant question, given the demand for growth in social security and public health.
The growing global burden due to population aging has drawn much attention as it threatens economic growth. Statistics show that the global disability-adjusted life years (DALYs) of the elderly population increased by 32% between 1990 and 2019, a number that is expected to increase by 55% between 2004 and 2030. 3 Research on the elderly population’s health condition is important for a better understanding of economic goals during the demographic transition and to ensure that socioeconomic policies are suitable for this increasing population.
Population aging is a demographic phenomenon that is occurring for the first time in human history. In the broader context of this global demographic change, the macroeconomic implications of population aging have been considered by many scholars in past studies. There are very different views of the relationship between population aging and economic growth, including that it is negative,4-7 positive,8-10 and U-shaped.11-13 Despite these contrasting research findings, population aging has been recognized by most countries as requiring serious attention. Moreover, in terms of indirect effects, population aging is significantly associated with macroeconomic factors such as the labor force, 14 physical capital, 15 human capital, 16 savings, and consumption.17,18 Although these path mechanisms are very important for inspiring and informing subsequent studies, there are also some areas that can be decomposed and improved. Most prior studies treat the elderly population as homogeneous and equate the rise in the number of elderly people with population aging. In fact, there is great heterogeneity in the older population, especially in terms of health status. These differences have diverse economic consequences, due to the important economic contributions of healthy older adults to both their families and society. Differences in the health statuses of the elderly population may also be one of the reasons past studies have reached different conclusions.
In recent years, the economic implications of elderly health have been a major concern in many countries. Studies have suggested that higher disease burdens generally lead to limited economic growth.19,20 One probable reason is that poor health makes it difficult to accumulate human capital and create an effective labor force, 21 while another is that the burden of disease may increase families and countries’ health-related expenditure.22,23 In fact, the burden of disease among the elderly population could increase families’ caregiving burden, affecting resource allocation and labor employment within the household.24,25 The family caregiving burden depends primarily on the health status of older adults, for example, their ability to perform the activities of daily living and instrumental activities of daily living, and their need for assistance with activity limitations, as well as time spent in a hospital or in bed with a serious illness. 26 Previous literature seemly provide us one logical pathway regarding the economic impact of elderly health status, that is, population aging increases the families’ caregiving burden, that make most families have no choice but to reduce their working hours to provide the needed care, which could reduce a country’s overall effective labor input, decelerating economic growth.
Although the economic effects of population aging have been extensively studied in the literature, few studies have focused on the elderly population’s health status and disease burdens. Moreover, there is a lack of country-level empirical evidence. Therefore, revisiting the economic impact of population aging from the health perspective and examining the relationships between elderly health, labor input, and economic growth may result in new insights and findings for policy practice.
Based on Solow economic growth theory, 27 this study’s goal is to determine whether the burden of health care for the elderly population affects effective labor input and economic growth and to assess which countries are most strongly associated with these effects.
Methods
This study is a cross-sectional empirical study using panel data from multiple databases involving 111 countries for the years 2000 to 2019.
Theoretical Model
To determine the relationship between population health and economic growth, we followed the model proposed by Acemoglu and Johnson. 2 Assuming a closed economy and that the factors of production are land, labor, capital, and technology, the aggregate production function can be written as follows:

where A denotes technology, K is total amount of capital formation, L is the land supply, and H is the effective labor input. For simplicity of analysis, the land supply is normalized to unity such that

Further, we assume that society’s total population, Nall, has only 2 generations, the younger generation, Nyoung, and the older generation, Nold, as follows:

The effective labor input, H, represents the total working hours of the younger population, namely the product of the younger population,

Following Grossman’s model, 28 we suppose there every young person’s time is allocated to 2 components: working time, Twork, and caring time, Tcare. We can also consider them as the labor participation time and the non-labor participation time. Then, we introduce the labor force participation rate, R, as an approximate proxy for labor force participation time. Thus the ratio of time allocation can be represented as follows:

Similarly, each older person’s time is allocated to either sickness time, Tsick, or wellness time, Twell. We then assume that all sick older people are cared for by the younger people. Therefore, the sick time of those in the older generation equals the caring time of those in the younger generation. Let

Substituting equation (5) into equation (4), we have:

Substituting equation (6) into equation (7), we have:

Substituting equation (8) into equation (2), we have:

Taking the logarithm of both sides, equation (9) can be simplified to the following:

From the above equation, we can see that economic production is related to health care burden of the old generation, capital formation, technology, and labor force participation rate.
Empirical Strategy
The fixed effects model in equation (11) was constructed based on equation (10), where G denotes economic growth, the health care burden is denoted as X, and the set of control variables is denoted as Z. Then,

The mediation models in equations (12) and (13) were constructed to perform a mediating effects analysis, where M denotes effective labor input according to the derivation of theoretical model above,


Variable Measurement
Economic growth was measured as the annual GDP growth rate (Growth). The annual GDP per capita growth rate (pcGrowth) was used as an alternative indicator.
The health care burden was measured as the DALY rate of persons aged 65 and over among the total population (DALY65). According to the World Health Organization, DALY is a measure of the overall disease burden and refers to population health expressed as the number of healthy life years lost due to disability caused by disease.
Effective labor input was used as the mediating variable in this study and was measured by 3 employment indicators: the total employment rate (Employment), part-time employment rate (PartTime), and self-employed employment rate (SelfEmployed).
The control variables were selected firstly according to the section of theoretical model above. Capital formation (Capital) is measured by the ratio of gross capital formation ratio to the country’s GDP. Total factor productivity (Technology) was calculated as the total factor productivity at constant national prices for the United States. Labor force participation rate (Labor) was measured by the percentage of the population keeping economically active for work. Secondly, some other control variables commonly used in economic growth studies also were selected from the previous literature.29-32 Foreign direct investment (Foreign) was measured as the ratio of net foreign direct investment to the country’s GDP. Foreign funds usually could help economies to invest for reproduction of enterprises, promoting economic development. Trade (Trading) was measured using the ratio of total import and export trade to the country’s GDP. It is well known that trading is important for optimizing the production of goods and may also affecting economic growth. Forest area (Forest) was measured as the ratio of forested areas to the country’s total land. The effect of the green environment on economic has received increasing attention in recent years and needs to be controlled while studying economic development issues.
In addition to these variables, several situational dummy variables from economic, demographic, and lifespan perspectives were used for the heterogeneity analysis, including whether a country was an OECD member (OECD_dummy), the elderly population proportion (AGED_dummy), and healthy life expectancy (HALE_dummy).
Sample Selection
The sample selection followed the principle of data availability based on all countries in the World Development Indicators (WDI) database from the World Bank. Data completeness of the indicators for the explanatory and core explanatory variables was the priority criterion, and those samples with missing critical data were excluded. A final sample of 111 countries, listed in Appendix Table A, was selected to constitute the panel data for the subsequent analysis. The sample selection process is shown as in Figure 1.

Sample selection process.
Data Collection
This study consolidated data from several databases. First, the annual GDP growth rate, annual GDP per capita growth rate, employment rate, part-time employment rate, self-employed employment rate, capital formation, foreign direct investment, trade amount, health expenditure share of GDP, forested area coverage, and population proportion of those aged 65 and above were taken from the WDI database. Subsequently, DALYs and healthy life expectancy were taken from the Global Health Data Exchange (GHDx) database. Finally, total factor productivity was sourced from the Penn World Table 10.0 (PWT 10.0) database. Table 1 summarizes the descriptive statistical characteristics of the indicators mentioned above.
Variable Definition and Descriptive Statistics.

Note. OECD_dummy denotes whether the country is a member of OECD (The Organization for Economic Co-operation and Development); AGED_dummy denotes whether the proportion of population over the age of 65 in the country is above or below 7% of the total population; HALE_dummy denotes whether the healthy life expectancy of the country is above or below 65 years.
Statistical Analysis
Various statistical analysis methods were used in this study, depending on the purpose of the analysis. Fixed effects model (FE) was used for the basic regression to directly estimate the effects of the health care burden on economic growth. To consider endogeneity concerns, the generalized method of moments (GMM) was used to estimate the dynamic panel model with lagged terms, while two-stage least squares (2SLS) with instrumental variables (IV) was used to identify causal effects. The heterogeneity among countries was examined by applying the grouped regression method. Finally, mediating effects were analyzed by employing various mediation analysis methods, including stepwise regression, 33 Sobel tests, 34 and the bootstrapping method. 35 STATA 16.0 was employed for all the statistical analyses.
Results
Basic Regression
The results of the basic regression are reported in Table 2. Column 2.1 shows that the regression coefficient of the health care burden (DALY65) was −0.083, indicating that, after including all the control variables, it has a significantly negative effect on economic growth (Growth) at the 1% significance level. This suggests that a 1% increase in the health care burden is associated with a 0.083% decrease in the GDP growth rate. Considering the control variables, the results demonstrate that countries with higher gross capital formation (Capital), labor force participation (Labor) and trade volume (Trading) have better economic growth. Moreover, the effect of forested area coverage (Forest) on economic growth was significantly negative.
Estimation Results of Basic Regression.
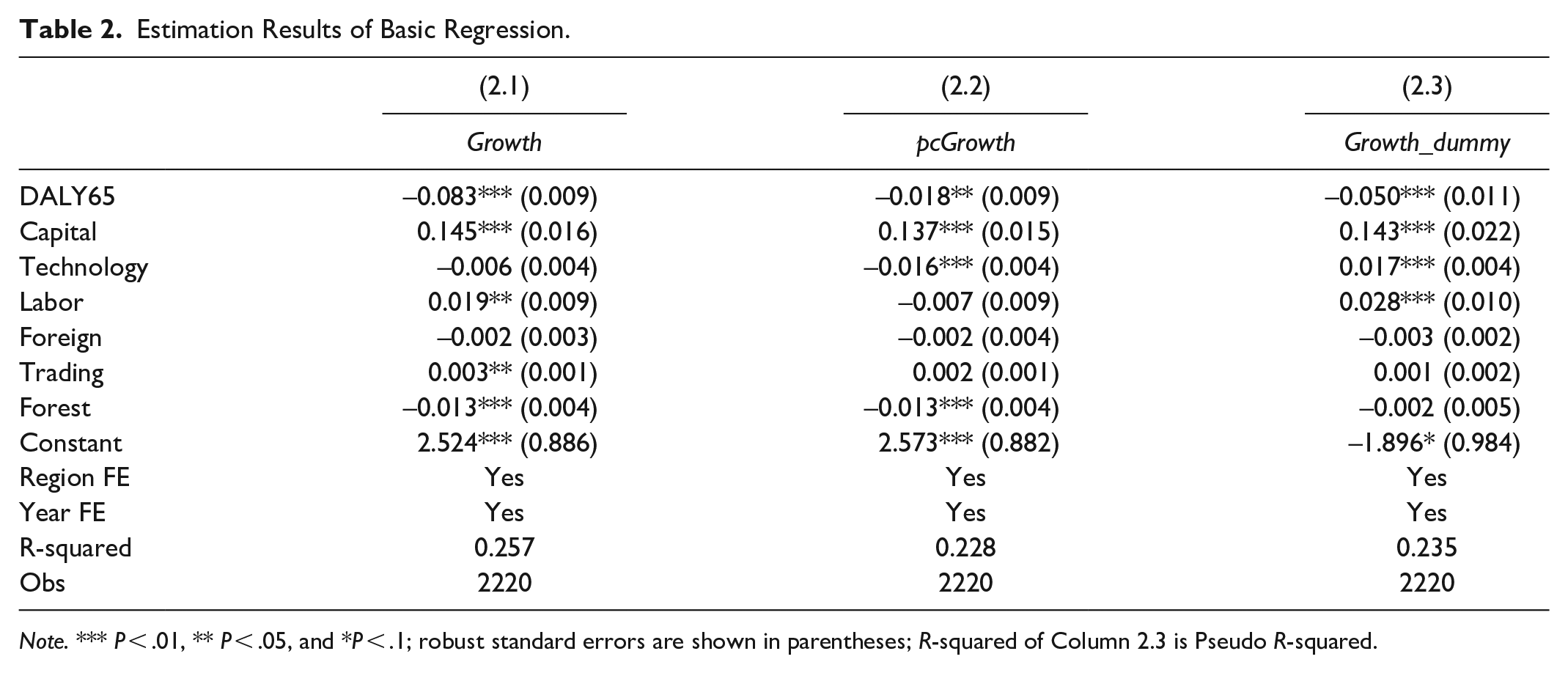
Note. *** P < .01, ** P < .05, and *P < .1; robust standard errors are shown in parentheses; R-squared of Column 2.3 is Pseudo R-squared.
To minimize concerns about measurement errors, the original economic growth measure was replaced with the annual GDP per capita growth rate (pcGrowth), which is often used as an alternative to the annual GDP growth rate. After re-estimating the regression, the results in Column 2.2 show that the regression coefficient of the health care burden was −0.018, which indicates that a 1% increase in the health care burden is associated with a 0.018% decrease in the GDP per capita growth rate. The result remained significantly negative at the 5% statistical level.
For the same reason, redefining economic growth as a dummy variable (Growth_dummy) could clarify economic growth trends. A value of 1 was assigned for a positive GDP growth rate, and a value of 0 was assigned for a negative GDP growth rate. According to the logistic regression results in Column 2.3, the regression coefficient of the health care burden was −0.050 and still kept significantly negative at the 1% level, indicating that increasing health care burden of the elderly population could lower the probability of economic growth.
Endogeneity Concerns
Since there may be serial correlation of economic growth in adjacent years, the lagged one-period term of economic growth is added into the baseline regression model, extending it to a dynamic panel model. Column 3.1 shows that the estimated coefficient of the first order lagged term of economic growth (Growtht-1) is significant at the 1% statistical level, indicating that the economic growth rate in the prior year does affect the current year’s rate. After controlling for this lagged effect, the impact of the health care burden on economic growth remains significantly negative at the 1% statistical level. Since dynamic panel models can also suffer from endogeneity problems, the systematic generalized method of moments estimation (SYS-GMM) is often required for further analysis. 36 The results of the SYS-GMM estimation are presented in Column 3.2, indicating that the estimated coefficient of the health care burden remains significantly negative at the 1% statistical level, while the parameters of the model specification are reasonable as shown as that appropriate-errors are uncorrelated of order 2 (AB test P-value > .1), there are no overidentifying restrictions (Hansen test P-value > .1).
To address potential endogeneity, we also applied the instrumental variable (IV) approach to strengthen the causal inferences. As the instrumental variable should be correlated with the endogenous variable, but uncorrelated with the error term, we used the prevalence of tobacco use among the elderly (IV_Tobacco*Old) as the instrumental variable for the health care burden (DALY65). The literature suggests that there is a strong positive relationship between tobacco use and elderly health.37,38 Consequently, the IV satisfies the relevance condition. It also appears to satisfy the exogeneity condition, since tobacco use among the elderly could not be directly related to economic growth, but only indirectly related through the health pathway. However, due to the lack of available data to directly measure IV, we employed the interaction term of the prevalence of current tobacco use and the percentage of elderly population as the measurement. The data of relevant indicators source from the WDI database.
The regression analysis using the two-stage least square (2SLS) method in Column 3.3 shows that the effects of the IV on the health care burden is significantly positive at the 1% level in the first-stage regression. Column 3.4 reports the results of the second-stage regression and shows that the IV has a negative impact on economic growth. The IV estimation passed the insufficient identification test (Kleibergen-Paap rk LM statistic P < .001) and weak instrumental variable test (Cragg-Donald Wald F statistic > 10). The results indicate that the health care burden has a significantly negative impact on economic growth (Table 3).
Estimation Results of Endogeneity Concerns.

Note. ***P < .01, **P < .05, and *P < .1; robust standard errors are shown in parentheses; data for calculating the variable (IV_Tobacco*Old) comes from the WDI database.
Heterogeneity Analysis
We conducted heterogeneity testing via subgroup regression according to a country’s economic, demographic, and lifespan status. Table 4 presents the results.
Estimation Results of Heterogeneity Analysis.
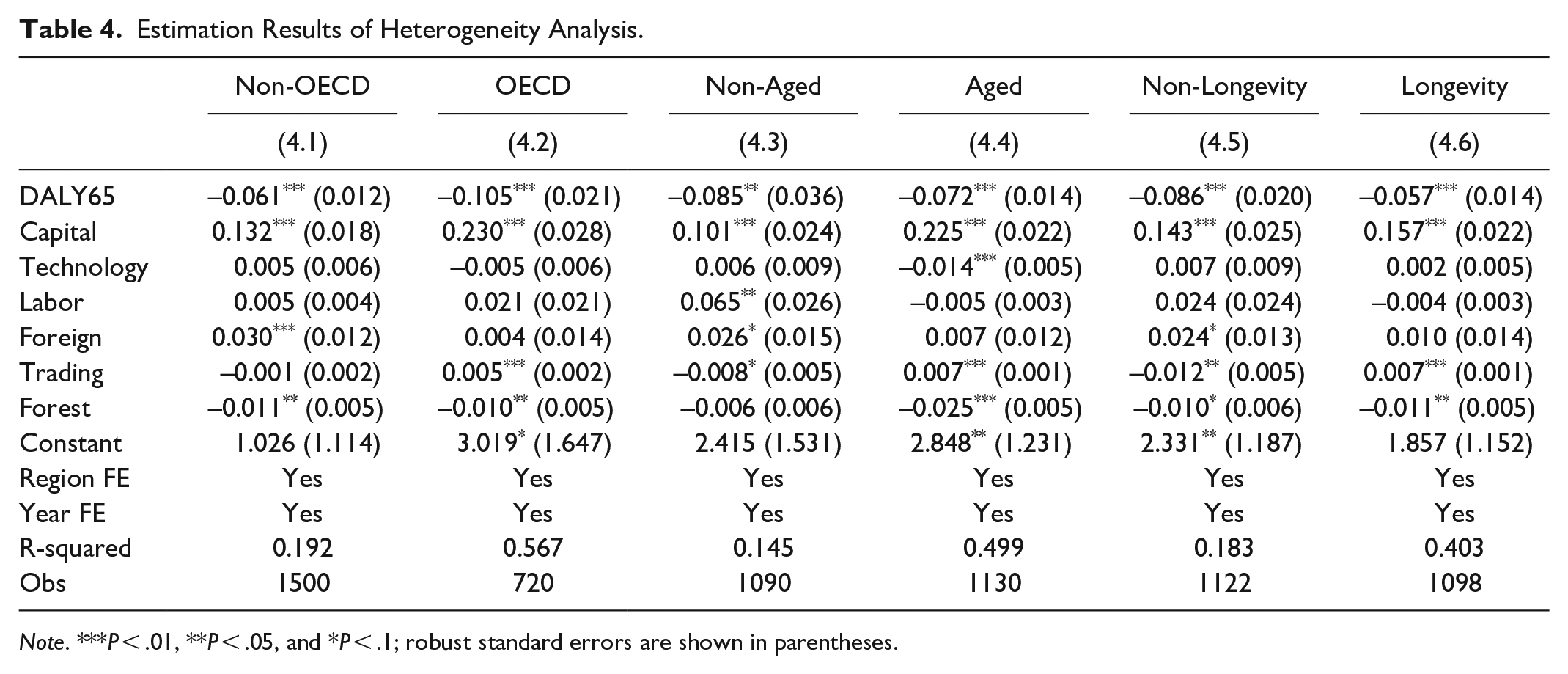
Note. ***P < .01, **P < .05, and *P < .1; robust standard errors are shown in parentheses.
First, the results of the non-OECD and OECD groups are shown in Columns 4.1 and 4.2, respectively. The coefficients of the health care burden were −0.061 and −0.105, respectively; both are significant at the 1% statistical level. This suggests that the regression coefficient of the OECD group is approximately 2 times that of the non-OECD group.
Second, the United Nations has defined an “aging society” as one where the share of people aged 65 years or above constitutes more than 7% of the total population. Countries with less than 7% were classified as non-aged, while countries with more than 7% were classified as aged. The results presented in Columns 4.3 and 4.4 show that the health care burden has significantly negative effects on economic growth at the 1% significance level both in the non-aged and aged groups, as the coefficients were −0.085 and −0.072.
Third, we set a healthy life expectancy of 65 years as the dividing line because the median value of healthy life expectancy for the countries in this study sample is approximately 65 years. We defined a healthy life expectancy below 65 years as the non-longevity group and a healthy life expectancy above 65 years as the longevity group. The results presented in Columns 4.5 and 4.6 demonstrate that the coefficients of the health care burden were −0.086 in the non-longevity group and −0.057 in the longevity group; both were significantly negative at the 1% statistical level. Overall, these results demonstrate that the effect of the health care burden on economic growth varies in magnitude, but there is no prominent heterogeneity among groups.
Mediating Effects
Next, the mediating effect of effective labor input was examined by introducing a mediating variable into the model. Three different measurements of effective labor input—the total employment rate (Employment), part-time employment rate (PartTime), and self-employed employment rate (SelfEmployed)—were used in the mediation model. These results are reported in Table 5.
Estimation Results of Mediating Effects.
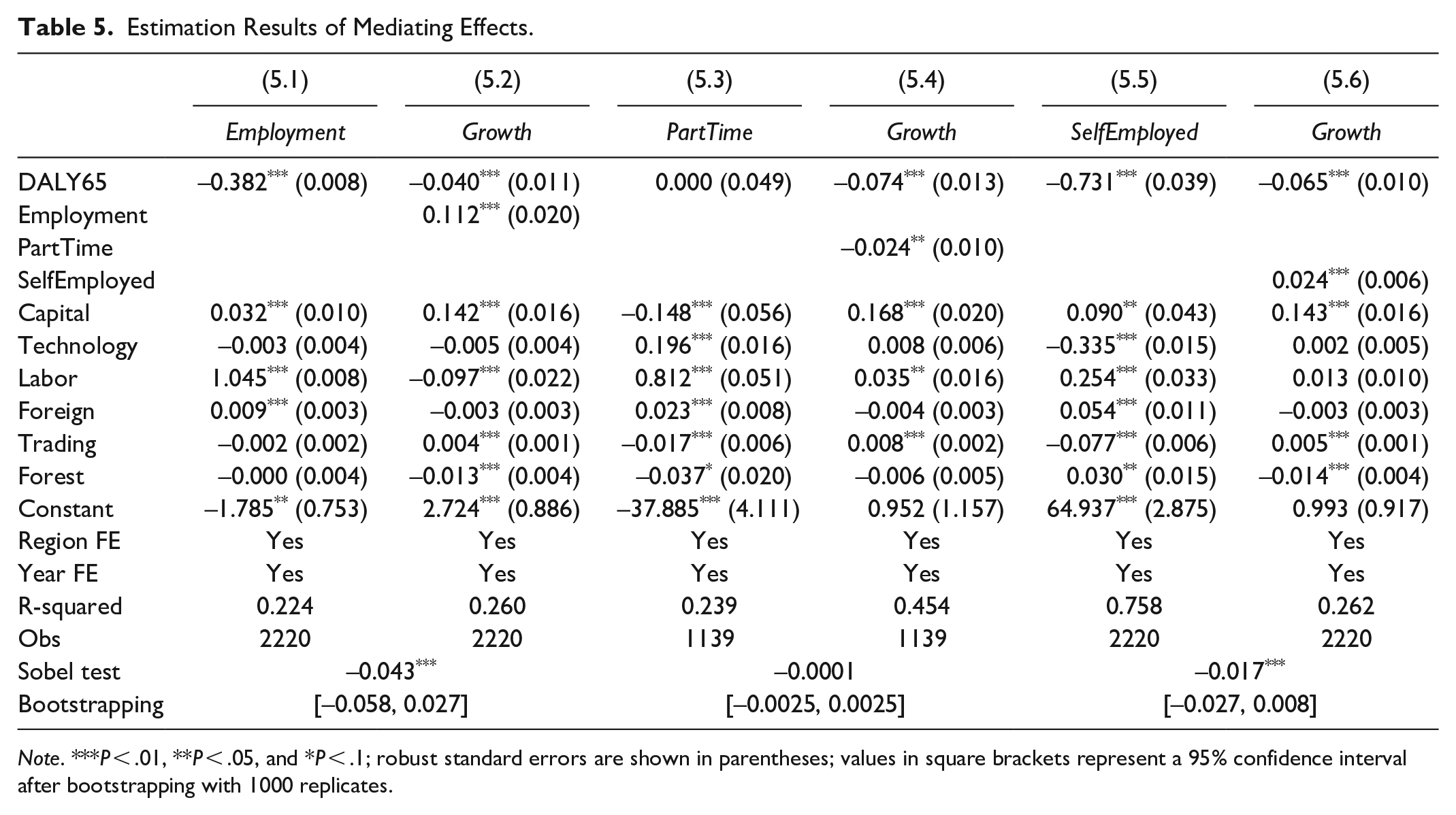
Note. ***P < .01, **P < .05, and *P < .1; robust standard errors are shown in parentheses; values in square brackets represent a 95% confidence interval after bootstrapping with 1000 replicates.
First, Columns 5.1 and 5.2 show that both the estimated coefficients of the health care burden (DALY65) on the total employment rate (Employment), of which on the economic growth (Growth) were statistically significant at the 1% level, and the indirect coefficient (−0.382 × 0.112) of the total employment rate (Employment) as the mediating variable was significant at the 1% level according to the Sobel test. In addition, the 95% confidence interval of the upper and lower limits of the mediating coefficient did not contain zero (LLCI = −0.058, ULCI = −0.027) for 1000 bootstrap resamples.
Second, Columns 5.3 and 5.4 demonstrate that the mediating effect of the part-time employment rate (PartTime) was not significant. The mediating coefficient did not pass the Sobel test and the 95% confidence interval contained zero (LLCI = −0.0025, ULCI = 0.0025) for 1000 bootstrap resamples.
Third, Columns 5.5 and 5.6 demonstrate that both the estimated coefficients of the health care burden (DALY65) on the self-employed employment rate (SelfEmployed), of which on the economic growth (Growth) were statistically significant at the 1% level, and the indirect the mediating coefficient (−0.731 × 0.024) of the self-employed employment rate (SelfEmployed) as the mediating variable was significant at the 1% level according to the Sobel test. Moreover, the 95% confidence interval did not contain zero (LLCI = −0.027, ULCI = −0.008) for 1000 bootstrap resamples.
These estimation results confirm the mediating role of the total employment rate (Employment) and the self-employed employment rate (SelfEmployed), suggesting that an increase in the health care burden could lead to a decrease in the total or self-employed employment rates, decelerating economic growth.
Robustness Tests
To exclude influence by outliers, we re-estimated the mediating effects with selected samples to enhance robustness. First, we excluded countries with an absolute GDP growth rate value over 10%; second, we excluded countries with populations of less than 1 million. Finally, we excluded 2008 to 2010, the years of the financial crisis.
The estimation results are shown in Table 6, which still indicate that the total employment (Employment) and self-employed employment (SelfEmployed) rates have significant mediating effects, but the mediating role of the part-time employment rate (PartTime) was not significant since failing to pass the bootstrap hypothesis test.
Robustness Test of Mediating Effects.

Note. ***P < .01, **P < .05, and *P < .1; robust standard errors are shown in parentheses; values in square brackets represent a 95% confidence interval after bootstrapping with 1000 replicates.
Discussion
This study empirically investigated the macroeconomic effects of the health care burden using cross-country panel data. The study produced some main findings that need to be explored in further depth.
First, the regression results demonstrated that the health care burden had a significantly negative effect on economic growth. The results remained consistently robust in a set of estimations that included a fixed effects model, dynamic panel model, and instrumental variable approach. These findings illustrate that the burden of elderly health care is one of the main reasons population aging could decelerate economic growth. The traditional view of the relationship between demographic structure and economic growth usually concentrates on changes in the working-age population. For example, it is widely believed that a decrease in the working-age population results in a less productive demographic structure, which leads to a decline in economic growth. 39 However, it is possible that the shrinking labor force combined with the aging population may not impact economic growth as previously understood due to labor-saving technological advances. 40 Currently, the rates of labor force participation and employment are insufficient, and much of the labor force remains unemployed. 41 In fact, the elderly population is also the main driving force of the growth in social welfare expenditure including public health and social security. 42 It is concerning that social welfare consumes scarce resources for unproductive social services, and thus, economic development is bound to be stifled in the long run.43,44 Therefore, the cause of the economic slowdown is not merely the shrinking working-age population, but also the increasing health care burden of the retired-age population.
Second, the heterogeneity analysis, which grouped countries by economic, demographic, and lifespan status demonstrated that the health care burden had a significantly negative economic effect under different conditions. This suggests that the relationship between the health care burden and economic growth is robust, and there is no situational interaction produced by external social conditions. As shown as in this study, the reason why the economic effect performed more significant in OECD countries might be the OECD countries that are more market-oriented also have more economic efficiency on the factors of production. When the health care burden for elderly population increases, the crowding-out effect on labor and other factors of production will lead to more economic slowdown than the non-OECD countries. However, there is much debate in the literature regarding this finding. It is thought that there is no clear relationship between health and GDP in OECD countries. 45 In contrast, there is evidence showing that the burden and costs of health care can affect GDP growth in low- and middle-income countries. 46 Theoretically, good health conditions indicate more human capital investment, which is a significant factor for economic growth. In addition, health improvement can expand the boundaries of production possibilities and increase labor efficiency at both the micro and macro levels. 47 It has been demonstrated that improvements in population health need to start with active health awareness and health literacy in the elderly population. 48
Third, the mediating roles of total employment and self-employed employment in the relationship between the health care burden and economic growth were significant. Numerous studies have confirmed the impact of population aging on employment rates and labor force participation.49-51 Although little research has explored this pathway from the perspective of the health care burden, the finding in our study is consistent with those of other similar studies. As far as similar studies are concerned, the health care burden of the elderly population affects employment rates because it increases the family’s need to provide caregiving to the elderly.52-55 Would it be better if there was long-term care insurance? The situation is similar to the evidence from Japan, which was one of the first countries worldwide to begin implementing long-term care insurance. 56 However, many solutions have been suggested to avoid unemployment, especially those emphasizing the use of formal caregiving and healthcare use. It is important to provide appropriate formal and informal home-based care services according to the different needs of elderly adults to improve the efficiency of the entire social system. 57 Moreover, an alternative opinion suggests that offering third-party long-term care provides new opportunities for employment creation by creating the need for a larger workforce to meet the increase in the demand for caregiving. 58 However, it is out of expectation that the mediating effect of part-time employment did not perform significant. Theoretically speaking, the part-time employment should have opposite effects of full-time employment that full-time employment rate goes down and part-time employment rate goes up when families take on additional responsibilities for care of elderly family members. The reason might be the incomplete data of part-time employment rate in this study, or perhaps the other reasons that need to be explored further.
Strengths and Limitations
This empirical study estimated the macroeconomic consequences of the health care burden in the context of population aging. Further, it provided more in-depth evidence to identify the mediating role of effective labor input. These findings indicate a new pathway through which population aging affects economic growth—through reduced effective labor input due to the burden of health care for the elderly—a topic that has been less discussed in previous studies. The study limitations include the lack of a strictly causal mechanism analysis, and using only employment to measure effective labor input, which could mean other important effects remain undiscovered. Future research can address these shortcomings and strengthen the study’s conclusions.
Conclusions
In line with the current trend of global population aging, this study has provided a new perspective to confirm the relationship between the elderly health and economic growth that the increasing health care burden of elderly population could decelerate economic growth through reducing the effective labor input of working-age population. The findings of this study are helpful to propose some policy recommendations to reduce the economic risks from the demographic transition. First, a multilevel elderly care service system should be established, including institutions, communities, and families, comprehensively covering all of the elderly’s care needs. Second, health literacy in elderly people should be enhanced to actively promote good health. Finally, labor policies should be reformed to be more flexible to reduce family caregiving for the elderly and protect against unemployment.
Footnotes
Appendix
Sample List of 111 Countries.

| Name | Code | Name | Code | Name | Code |
|---|---|---|---|---|---|
| Angola | AGO | Guatemala | GTM | Niger | NER |
| Argentina | ARG | Honduras | HND | Nigeria | NGA |
| Armenia | ARM | Hungary | HUN | Norway | NOR |
| Australia | AUS | Iceland | ISL | Panama | PAN |
| Austria | AUT | India | IND | Paraguay | PRY |
| Bahrain | BHR | Indonesia | IDN | Peru | PER |
| Barbados | BRB | Iran, Islamic Rep. | IRN | Philippines | PHL |
| Belgium | BEL | Iraq | IRQ | Poland | POL |
| Benin | BEN | Ireland | IRL | Portugal | PRT |
| Bolivia | BOL | Israel | ISR | Romania | ROU |
| Botswana | BWA | Italy | ITA | Russian Federation | RUS |
| Brazil | BRA | Jamaica | JAM | Rwanda | RWA |
| Bulgaria | BGR | Japan | JPN | Saudi Arabia | SAU |
| Burkina Faso | BFA | Jordan | JOR | Senegal | SEN |
| Burundi | BDI | Kazakhstan | KAZ | Serbia | SRB |
| Cameroon | CMR | Kenya | KEN | Sierra Leone | SLE |
| Canada | CAN | Korea, Rep. | KOR | Singapore | SGP |
| Central African | CAF | Kuwait | KWT | Slovak Republic | SVK |
| Chile | CHL | Kyrgyz Republic | KGZ | Slovenia | SVN |
| China | CHN | Lao PDR | LAO | South Africa | ZAF |
| Colombia | COL | Latvia | LVA | Spain | ESP |
| Costa Rica | CRI | Lesotho | LSO | Sri Lanka | LKA |
| Croatia | HRV | Lithuania | LTU | Sudan | SDN |
| Cyprus | CYP | Luxembourg | LUX | Sweden | SWE |
| Czech Republic | CZE | Malaysia | MYS | Switzerland | CHE |
| Denmark | DNK | Malta | MLT | Tajikistan | TJK |
| Dominican Republic | DOM | Mauritania | MRT | Tanzania | TZA |
| Ecuador | ECU | Mauritius | MUS | Thailand | THA |
| Egypt, Arab Rep. | EGY | Mexico | MEX | Togo | TGO |
| Estonia | EST | Moldova | MDA | Tunisia | TUN |
| Eswatini | SWZ | Mongolia | MNG | Turkey | TUR |
| Fiji | FJI | Morocco | MAR | Ukraine | UKR |
| Finland | FIN | Mozambique | MOZ | United Kingdom | GBR |
| France | FRA | Namibia | NAM | United States | USA |
| Gabon | GAB | Netherlands | NLD | Uruguay | URY |
| Germany | DEU | New Zealand | NZL | Zambia | ZMB |
| Greece | GRC | Nicaragua | NIC | Zimbabwe | ZWE |
Data Accessibility
The data are publicly available from the official website of the database involved in this study and are attainable from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.