
Abstract
The 29-item CareGiver Oncology Quality of Life (CarGOQoL) scale measures quality of life (QoL) based on the specific characteristics of informal caregivers of patients with cancer. The 29-item CarGOQoL has been translated to numerous other languages and validated, thus confirming its validation. This study aimed to evaluate the reliability and validity of the Korean version of the 29-item CarGOQoL. We recruited 316 informal caregivers of patients with cancer. Data were collected using structured questionnaires between January 23, 2019 and November 30, 2019, and analyzed using SPSS 27.0 and Amos 23.0. Internal consistency, construct validity, convergent and discriminant validity of the items, criterion validity, and known-group validity were tested. The 10-factor model was validated by a confirmatory factor analysis (χ2 = 687.633; P < .001; normed χ2 = 2.084; comparative fit index = .922; Tucker–Lewis index = .904; standardized root mean square residual = .050; root mean square error of approximation = .059). Criterion validity was demonstrated using the World Health Organization Quality of Life instrument-short version (r = .495-607), visual analog scale (VAS) for QoL (r = .509), and VAS for burden (r = −.457). The 29-item Korean version of the CarGOQoL had known-group validity according to the Eastern Cooperative Oncology Group performance status of the patients. Cronbach’s alpha coefficient for the total scale was .90. The 29-item Korean version of the CarGOQoL demonstrated acceptable validity and reliability for measuring QoL among Korean informal caregivers of patients with cancer. The 29-item Korean version of the CarGOQoL scale can be useful in Korean oncology clinical practice and research when assessing the quality of life of informal caregivers of patients with cancer.
Physical and psychosocial problems experienced by informal caregivers of patients with cancer reduce their quality of life.
The 29-item CareGiver Oncology Quality of Life scale assesses specific characteristics of informal caregivers of patients with cancer. The 29-item Korean version of the CareGiver Oncology Quality of Life has acceptable validity and reliability.
The 29-item Korean version of the CareGiver Oncology Quality of Life scale can be useful in Korean oncology clinical practice and research when assessing the quality of life of informal caregivers of patients with cancer.
Introduction
Advances in modern medicine have enabled the early detection and treatment of cancer, thereby increasing the cure rate and prolonging life. However, cancer remains the leading cause of death worldwide. 1 The 5-year survival rate of patients with cancer in Korea is 70.4%, which is higher than that of other countries comprising the Organization for Economic Co-operation and Development. 2 Patients diagnosed with cancer receive various treatments for active or palliative purposes, such as surgery, radiation therapy, and systemic treatments including chemotherapy, hormonal therapy, and immunotherapy. 3 During this process, patients with cancer experience various types of psychosocial distress, such as depression, anxiety, fear of recurrence, anger, and social inhibition, as well as physical problems, such as pain, nausea, vomiting, fatigue, and constipation.4-6 Recently, the treatment method for patients with cancer has shifted from hospitalization-oriented treatment to outpatient and day ward treatment, or even if hospitalized, the length of stay is getting shorter. Many people with cancer get most of their care at home rather than in a hospital. Therefore, patients with cancer experience various side effects caused by treatment at home.7,8 This means that spouses, partners, family members, friends, or neighbors who live with or near them may need to take on several day-to-day medical and non-medical responsibilities. 9
Informal caregivers, also called family caregivers, are people who give care to family, friends, or neighbors usually without payment. 9 In a literature review study on the quality of life (QoL) of informal caregivers for patients with cancer, it was reported that approximately 67% of caregivers were women, and the average age was 54.2 years. Also, as for family bonds, most caregivers were spouses or daughters or sons of the patients with cancer, usually sharing the same home. 10 These caregivers of patients with cancer endure an array of physical and psychosocial changes experienced by these patient during treatment; consequently, these caregivers encounter various physical and psychosocial problems, including physical fatigue, 11 depression, 12 lower self-esteem, 13 loneliness, and social isolation. 14 These problems are intensified by the burdens associated with care, such as physical burdens, inadequate cooperation from family, changes in lifestyle patterns, and financial burdens.15,16 Ultimately, the QoL and well-being of these caregivers are impaired.16,17
A previous study of informal caregivers of patients with cancer reported that the prevalence of anxiety symptoms among this population reached 38.1%, and that the prevalence of depression symptoms ranged from 20.0% to 82.2%. 18 Furthermore, a study that compared the psychological burden of patients with cancer and that of their primary caregivers demonstrated that caregivers experience a degree of pain comparable to that of patients with cancer and an even higher levels of mental stress.19,20 Therefore, the QoL of informal caregivers of patients with cancer and that of patients with cancer during treatment warrant the same attention as the population of patients with cancer grows. Well-being and QoL of informal caregivers have both direct and indirect implications on quality of cancer care, including the care given by the medical staff, by the caregivers themselves, and in relation to patients’ own self-management. Supporting caregivers impacts patient outcomes directly, including daily treatment regimens, symptom management, self-care practices, and patient’s QoL. 21 Therefore, a multifaceted strategy is required to enhance the QoL and well-being of informal caregivers for patients with cancer.
Recently, several studies have assessed the QoL of informal caregivers of patients with cancer and highlighted the need to focus more attention on them. The most widely used instruments for measuring the QoL of caregivers include the Caregiver Quality of Life Index-Cancer Scale, 22 the Caregiver Quality of Life Index, 23 and the CareGiver Oncology Quality of Life (CarGOQoL). 24 The Caregiver Quality of Life Index-Cancer Scale was developed based on a mixed-methods design; patients and family caregivers were interviewed together and analyzed by experts. This tool has been validated by only the spouses of patients. In addition, this tool consisted of 35 items measuring physical, emotional, family and social functioning. However, at the time of development, there is a limitation in that factor analysis that can determine the sub-dimension of the measurement tool was not conducted. Another measurement tool, the Caregiver Quality of Life Index, is a simple tool that has been validated among only 5 individuals, who were asked to indicate the relevance of predefined items. Thus, it has limitations in comprehensively measuring QoL of informal caregivers of patients with cancer.
The 29-item CarGOQoL, which was developed by Minaya et al, 24 was developed based on a face-to-face, semi-structured interview with 77 individuals. Such instruments developed based on a clear conceptual framework are currently accepted as the best. Moreover, this tool has been validated among 837 informal caregivers comprising children, spouses, and parents. Therefore, during the item development phase, CarGOQoL was established using caregiver feedback.24,25 It is believed that the participation of the target population throughout the creation of the instrument is necessary to establish its content validity. As mentioned above, the QoL of informal caregivers for patients with cancer has multidimensional aspects such as psychological, physical, and social well-being and burden, coping strategies, finances, relationships with medical professionals, and changes in lifestyle patterns. The 29-item CarGOQoL has 10 subdomains, including psychological well-being, burden, relationships with healthcare, administration and finances, coping, physical well-being, self-esteem, leisure time, social support, and private life. 24 Therefore, it has the advantage of being able to measure the QoL that can encompass the multidimensional attributes of informal caregivers of patients with cancer.
The 29-item CarGOQoL was originally developed in French, 24 and the English 26 and Portuguese 27 versions have been validated. The CarGOQoL is currently undergoing linguistic validation among various cultures, including Greek and Mandarin. The English version of this tool was also extracted into the same 10 subdomains of the 29 items as the original French version at the time of tool development; however, the Portuguese version for caregivers of only multiple myeloma was extracted into 5 subdomains (well-being, relationship with health care, administration and finances, coping, and leisure) of the 17 items. The QoL is a concept that encompasses an individual’s subjective experience of physical, social, and emotional health and is a sense of well-being that is subjectively evaluated in the context of the culture in which an individual lives and its value. 28 In Asian sociocultural contexts, family relationships and family unit are more emphasized than in the West, which may have an impact on expectations regarding family caregiving obligations and arrangements. 29 In order to apply a tool developed abroad, its reliability and validity must be verified in the relevant cultural context and become a reliable tool.
The 29-item CarGOQoL has completed the Korean translation and back-translation process, content validity verification, and pilot test 30 using cultural adaptation guidelines 31 ; however, the applicability and final version of the CarGOQoL require confirmation through cross-cultural validation among Korean informal caregivers of patients with cancer. Therefore, this study aimed to evaluate the validity and reliability of the 29-item Korean version of the CarGOQoL (K-CarGOQoL) so that it can be useful in Korean oncology clinical practice and research for assessing the QoL of informal caregivers of patients with cancer.
Materials and Methods
Study Design
This cross-sectional study was conducted in 2019.
Participants and Setting
The target research population comprised informal caregivers of patients with cancer who were currently undergoing treatment at outpatient hematology and oncology clinics at Chonnam National University Hwasun Hospital located in the Jeollanamdo province of South Korea. The inclusion criteria were as follows: adults 19 years of age or older; being an “informal caregiver” (parents, spouses, or other family members, friends who cares for a patient with cancer and does not receive payment for care) designated by a patient9,24; has been caring for more than 4 weeks 24 ; ability to read and write Korean; free from cancer comorbidity; and voluntarily signed an informed written consent to participate in the study. The exclusion criteria were occupational and formal caregivers of patients with cancer and a history of or undergoing current treatment for mental disorders (eg, depression and anxiety).
Among the 380 participants recruited, 316 (83.2%) provided written informed consent. Therefore, 316 participants were included in the data analysis. The minimum sample size required to test the construct validity of a measurement tool using the confirmatory factor analysis (CFA) is 200 or 5-times the number of items. 32 The sample size of the present study was 316 for 29 items; therefore, the required sample size was achieved.
Data Collection
Data were collected using structured self-reported questionnaires from January 2019 to November 2019. Two research assistants were fully informed of the purposes and procedures of the study; as an initial screening, they asked caregivers some questions (eg, “Do you recognize yourself as a caregiver?” “Do you get paid to take care of them?” etc.) and confirmed their willingness to participate in the study. Data collection was conducted in the education room, a quiet place in the outpatient clinic. Informal caregivers were asked about QoL (CarGOQoL, World Health Organization Quality of Life Instrument-short version [WHOQOL BREF], and visual analog scale [VAS]), burden (VAS), and the general characteristics of informal caregivers and patients with cancer.
Measures
CareGiver Oncology Quality of Life questionnaire
The CarGOQoL assesses the QoL of informal caregivers of patients with cancer using 29 items in the following 10 subdomains: psychological well-being (4 items); burden (4 items); relationship with health care (3 items); administration and finances (3 items); coping (3 items); physical well-being (4 items); self-esteem (2 items); leisure (2 items); social support (2 items); and private life (2 items). Each item is measured using a 5-point Likert scale. The psychological well-being (4 items), burden (4 items), self-esteem (3 items), coping (3 items), physical well-being (4 items), and private life (one item) were reverse-coded. Scores for each domain were obtained by calculating the average item score for that domain. The index was calculated as the average of the domain scores. All domain scores and the index were linearly transformed and normalized using a scale of 0 to 100. The higher the score, the better the QoL. For each individual, a domain score was calculated when more than half of the questions were answered. During tool development, Cronbach’s α values for each subdomain ranged from .72 to .89. 24 The CarGOQoL was developed using a linguistic validation process 31 that included translation, back translation, a first panel discussion, a pilot test, and a second panel discussion. 30 The tool developers evaluated the appropriateness of each step.
World Health Organization Quality of Life Instrument-short version
Criterion validity was evaluated using the Korean version of the WHOQOL-BREF, 33 which was originally developed by the WHOQOL Group. 28 The Korean version of the WHOQOL-BREF comprises 26 items (general health, one item; overall QoL, one item; physical health dimension, 7 items; psychological dimension, 6 items; social relationship dimension, 3 items; environment dimension, 8 items). Each item was scored using a 5-point Likert scale, and the subdomain scores were computed by multiplying the mean score of each subdomain by 4. The subdomain scores ranged from 4 to 20. The higher the score, the better the QoL. The internal consistency reliability (Cronbach’s α) of the entire tool was .90, and that of each domain at the time of the development of the Korean version ranged from .58 to .73. 34 In the present study, Cronbach’s α was .91 for the overall QoL, and that for each domain ranged from .71 to .85.
Subjective QoL
To assess the criterion validity, the perceived QoL of the participants was assessed using one item and the VAS. The VAS consists of a 100 mm linear scale ranging from 0 to 10, with a higher score indicating a better QoL.
Burden
To assess the criterion validity, the perceived care burden of the participants was assessed using one item and the VAS. The VAS consists of a 100 mm linear scale from 0 to 10, with a higher score indicating a worse care burden.
Eastern Cooperative Oncology Group performance status
We used the Eastern Cooperative Oncology Group (ECOG) performance status (PS), 34 which rates the physical activity status of patients with cancer using a scale from 0 to 5, to confirm the known-group validity of the K-CarGOQoL. The ECOG PS categorizes the physical activity status into 5 groups (group 0: no signs, fully active; group 1: some signs but ambulatory and does not require bed rest while awake; group 2: bed rest for less than 50% of the awake time; group 3: bed rest for more than 50% of the awake time; group 4: totally confined to the bed). The ECOG PS scores were obtained from the electronic medical records and evaluated by the physicians at the time when the CarGOQoL questionnaire was administered.
General characteristics
The age, gender, relationship with the patients, and caregiving duration of the caregivers were collected. Additionally, the age, gender, cancer location, cancer stage, metastasis, and disease duration of the patients with cancer were collected.
Ethical Considerations
The institutional review board of Chonnam National University Hwasun Hospital approved this study (IRB No. CNUHH-2019-023). The study was conducted in accordance with the ethical standards of the institution’s Committee on Human Experimentation and the Helsinki Declaration of 1975. All participants submitted written informed consent prior to participating in the study and were informed of the advantages, risks, research protocol, and option to voluntarily withdraw at any time.
Statistical Analysis
Data analysis was performed using SPSS version 27.0 (IBM Corp., Armonk, NY, USA) and AMOS 23.0 (IBM Corp.). The general characteristics of the participants were analyzed using the frequency, mean, standard deviation, range, median, and interquartile range. The items were analyzed using the mean, standard deviation, missing percentage, floor effect, ceiling effect, skewness, kurtosis, and internal consistency of each item. The CFA to verify the model was performed using the normed χ2 (χ2/degrees of freedom), Tucker–Lewis index, comparative fit index (CFI), root mean square error of approximation (RMSEA), and standardized root mean square residual. When validating the goodness of fit, normed χ2 values ≤3.0 indicated acceptable fit, and CFI and Tucker–Lewis index values ≥.90 indicated good fit. 35 Standardized root mean square residual and RMSEA values between .05 and .08 indicated good fit. 36 Convergent validity and discriminant validity of the items were verified using the CFA model. To determine the convergent validity of each item, standardized regression weights, the average variance extracted (AVE), and composite reliability were evaluated. Standardized regression weights ≥.5, AVE ≥.5, and composite reliability ≥.7 were the reference values. 36 To determine the discriminant validity of each item, the AVE values were compared with the square values of the correlation coefficients for each subdomain of the K-CarGOQoL. Criterion validity was verified by identifying Pearson correlation coefficients of the relationships between the subdomain of the K-CarGOQoL and the subdimension of the WHOQOL-BREF, QoL (VAS), and burden (VAS). Sufficient correlations between similar scales (r = .40-.80) supported the criterion validity. Internal consistency was analyzed using Cronbach’s alpha. Cronbach’s alpha of .7 was regarded as sufficient; P < .05 was considered statistically significant.
Results
Participant Characteristics
Table 1 presents the descriptive statistics of the caregivers and patients. The mean age of the caregivers was 49.5 years (standard deviation, 11.56 years; range, 25-84 years); 59.5% were women and 75.6% (239 caregivers) had a partner. Regarding their relationship with the patient, 53.2% were children of the patient and 32.2% were spouses of the patient. The mean duration of caregiving was 9 months (range, 4-25 months). The mean age of the patients was 67.1 years (standard deviation, 10.86 years; range, 35-88 years), and 57.9% were men. The cancer types were gastric cancer (20.6%), hepatobiliary cancer (19.9%), pancreatic cancer (18.0%), and colorectal cancer (17.4%). Most cancer stages were stage 3 (26.9%) and stage 4 (36.2%). The mean illness duration was 12 months (range, 7-29 months), and about 66% of the patients had an ECOG PS grade of 0 or 1.
Participant Characteristics in the Baseline (N = 316).
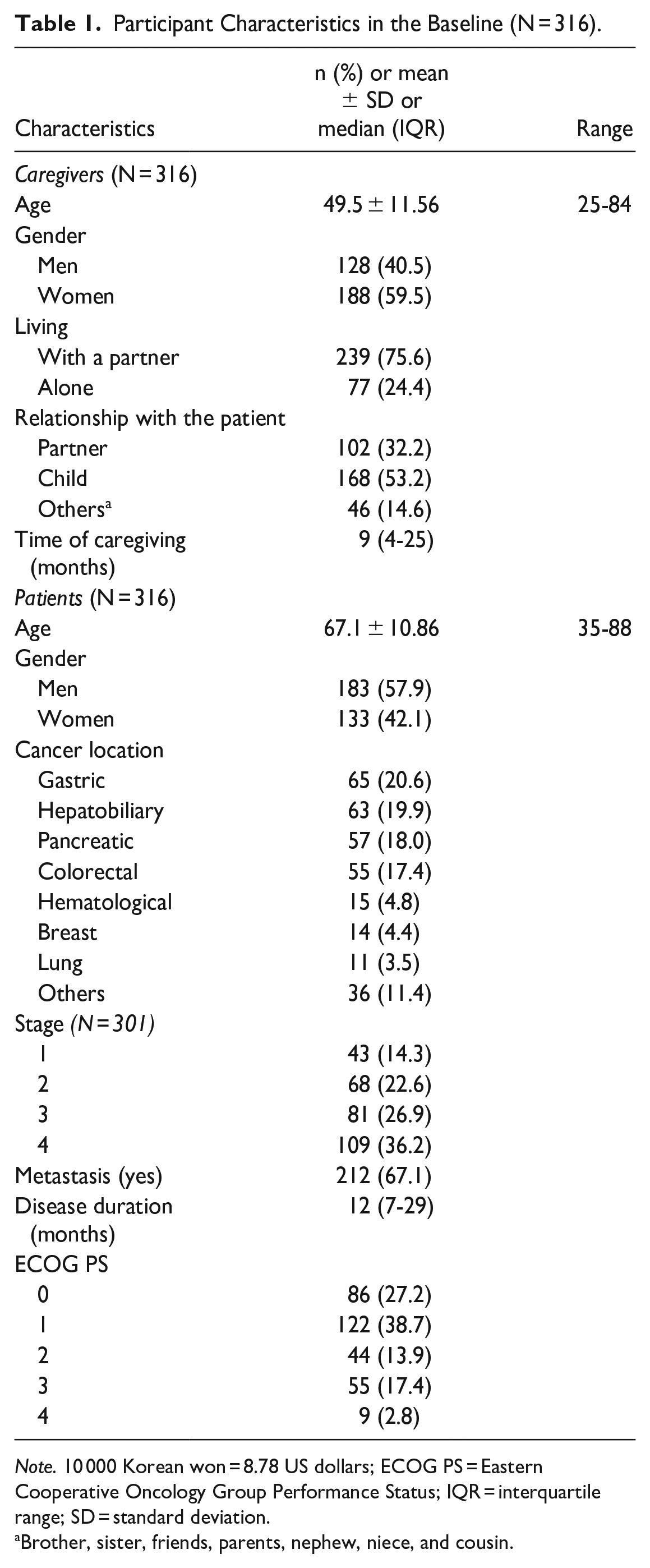
Note. 10 000 Korean won = 8.78 US dollars; ECOG PS = Eastern Cooperative Oncology Group Performance Status; IQR = interquartile range; SD = standard deviation.
Brother, sister, friends, parents, nephew, niece, and cousin.
Item Analysis
The skewness of each item of the 29-item K-CarGOQoL ranged from −5.03 to 0.24. The kurtosis ranged from −2.30 to 2.83. The data were normally distributed. The floor effect for each subscale of the 29-item K-CarGOQoL ranged from 0.6% to 3.5%, and the ceiling effect ranged from 1.6% to 13.3% and was less than 15.0%, which was considered acceptable for all subdimensions. 37 The amount of missing data for each item of the 29-item K-CarGOQoL ranged from 0.0% to 0.5% and was less than 10.0%, which was acceptable for all subdimensions. 35 The mean 29-item K-CarGOQoL index score was 69.34 (standard deviation, 9.85) (Table 2).
Dimension of Characteristics of the 29-Item K-CarGOQoL (N = 316).
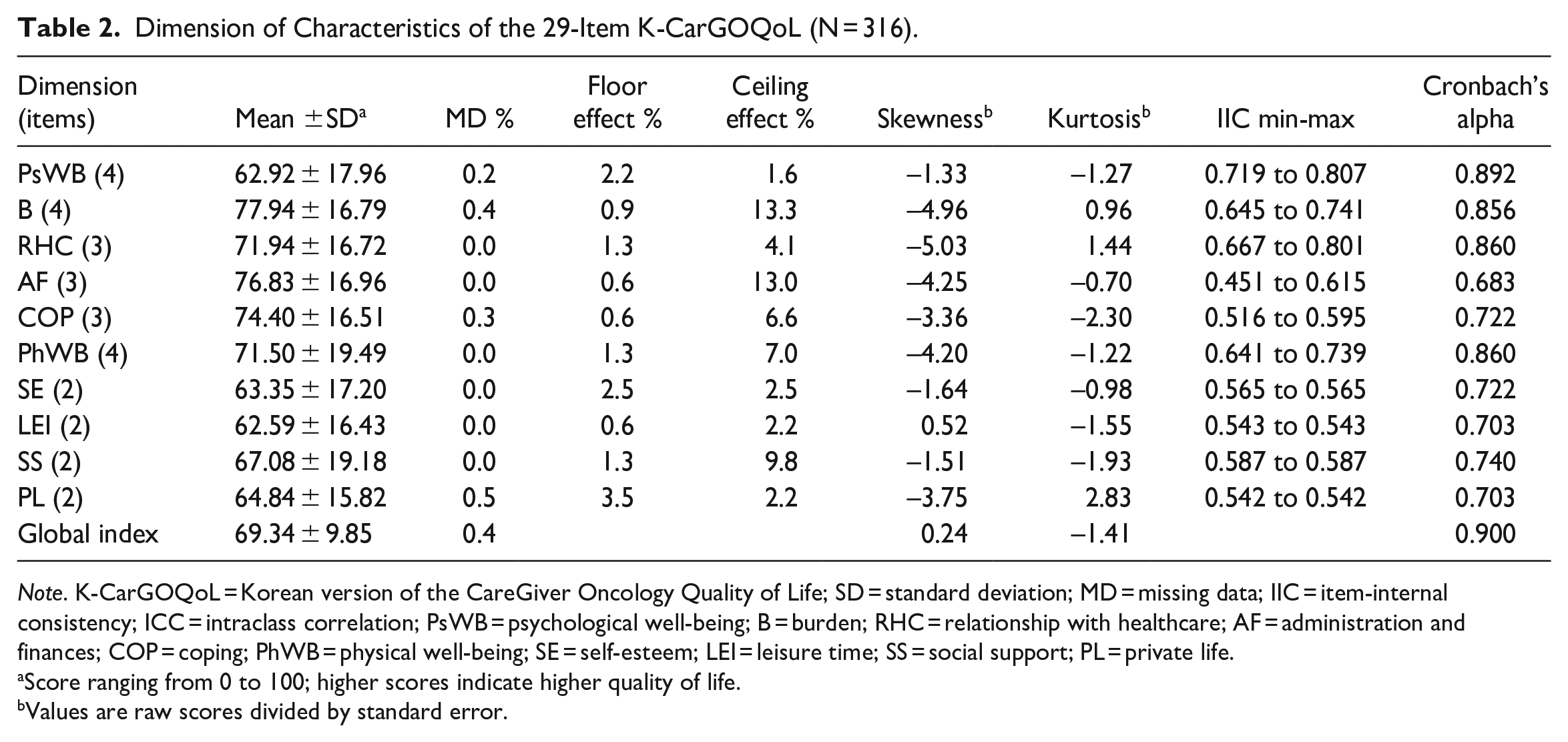
Note. K-CarGOQoL = Korean version of the CareGiver Oncology Quality of Life; SD = standard deviation; MD = missing data; IIC = item-internal consistency; ICC = intraclass correlation; PsWB = psychological well-being; B = burden; RHC = relationship with healthcare; AF = administration and finances; COP = coping; PhWB = physical well-being; SE = self-esteem; LEI = leisure time; SS = social support; PL = private life.
Score ranging from 0 to 100; higher scores indicate higher quality of life.
Values are raw scores divided by standard error.
Validity
Construct validity
The CFA model of the measurement was fitted to the data. The results of the CFA were as follows: χ2 = 687.633 (P < .001); degrees of freedom = 329.958; normed χ2 (χ2/degrees of freedom) = 2.084; Tucker–Lewis index = .904; CFI = .922; RMSEA = .059; and standardized root mean square residual = .050. The standardized regression weights of all items ranged from .558 to .926. The AVE of the subdomain ranged from .519 to .724. The composite reliability of the subdomain ranged from .721 to .886. Therefore, the convergent validity of each item of the 29-item K-CarGOQoL was confirmed, and the discriminant validity of each item confirmed that AVE values were greater than those of the square values of the correlation coefficients for each subdomain (Table 3).
Results of Confirmatory Factor Analysis for the 29-Item K-CarGOQoL.

Note. K-CarGOQoL = Korean version of the CareGiver Oncology Quality of Life; SE = standardized estimate; SRW = standardized regression weights; CR = composite reliability; AVE = average variance extracted; PsWB = psychological well-being; B = burden; RHC = relationship with healthcare; AF = administration and finances; COP = coping; PhWB = physical well-being; SE = self-esteem; LEI = leisure time; SS = social support; PL = private life.
P value <.05 (Pearson’s correlation).
P value <.01 (Pearson’s correlation).
Criterion validity
The global index of the 29-item K-CarGOQoL had statistically significant positive correlations with the physical health, psychological, social relations, and environmental domains of the WHOQOL-BREF (r = .495-.607) (Table 4). The 29-item K-CarGOQoL had a statistically significant positive correlation with QoL (VAS) (r = .509) and a statistically significant negative correlation with burden (VAS) (r = −.457) (Table 4).
Correlations Between of the 29-item K-CarGOQoL and WHOQOL-BREF, QoL, and Burden (N = 316).

Note. K-CarGOQoL = Korean version of the CareGiver Oncology Quality of Life; PsWB = psychological well-being; B = burden; RHC = relationship with healthcare; AF = administration and finances; COP = coping; PhWB = physical well-being; SE = self-esteem; LEI = leisure time; SS = social support; PL = private life; range [0-100]; higher scores indicate higher quality of life.
WHOQOL-BREF = The World Health Organization Quality of Life Scale – Short Form; range [4‒20]; higher scores indicate higher quality of life; QoL (VAS), range [0‒10]; higher scores indicate higher quality of life; Burden (VAS), range [0‒10]; higher scores indicate higher burden.
P value <.05 (Pearson’s correlation), **P value <.01 (Pearson’s correlation).
Known-group validity
The known-group validity of the 29-item K-CarGOQoL was verified using the ECOG PS of the patients. Patients had higher QoL scores for all dimensions and global indices except for the self-esteem, leisure, social support, and private life dimensions, which had decreasing ECOG PS grades (Table 5).
Comparisons of the 29-Item K-CarGOQoL Scores According to Patients’ ECOG-PS.
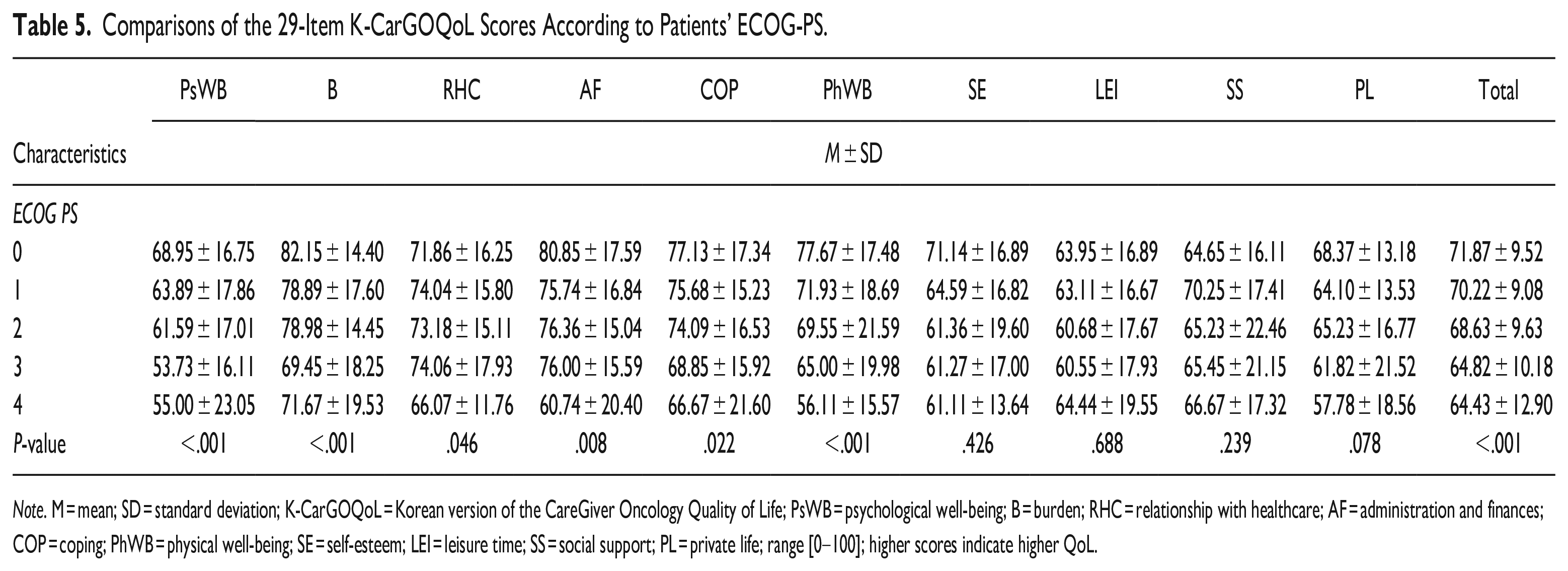
Note. M = mean; SD = standard deviation; K-CarGOQoL = Korean version of the CareGiver Oncology Quality of Life; PsWB = psychological well-being; B = burden; RHC = relationship with healthcare; AF = administration and finances; COP = coping; PhWB = physical well-being; SE = self-esteem; LEI = leisure time; SS = social support; PL = private life; range [0‒100]; higher scores indicate higher QoL.
Reliability
Cronbach’s alpha value of the global index was .900 for the 29-item K-CarGOQoL. The values for the 10 subdimensions ranged from .683 to .892. Table 2 shows the reliability verification results for the 10 subdimensions.
Discussion
Informal caregivers of patients with cancer encounter a variety of physical and psychosocial changes caused by the disease and treatment, as well as physical and psychological issues that subsequently occur. Therefore, continuous attention to the QoL of not only cancer patients undergoing treatment but also caregivers taking care of them is required. The current study verified the validity and reliability of the 29-item K-CarGOQoL, which is a specific scale that was developed to assess the QoL of informal caregivers of patients with cancer.
Cronbach’s alpha values of 9 subdimensions (range, .703-.892) and the global index (Cronbach’s alpha = .900) were ≥.70, which indicates good reliability; however, that of the administration and finances subdimension was not (Cronbach’s alpha = .683). 38 The results of this study are similar to those of the original French (Cronbach’s alpha = .55-.89) and English versions (Cronbach’s alpha = .26-.87). Overall, relatively high alpha values indicated strong reliability. However, test-retest reliability was not verified during this study. It is necessary to verify the consistency of the tool by conducting a test-retest in the future.
During the construct validity analysis, the CFA results for the 10-factor model were acceptable and similar to the results of the original French (non-normed fit index = .90; CFI = .92; RMSEA = .04) and American (RMSEA = .08) versions. Additionally, the K-CarGOQoL confirmed the convergent validity and discriminant validity of the items. In this study, 10 subdomains in the Korean cultural context were extracted the same as the original tool developed in the West, which means that CarGOQoL includes all multidimensional attributes to measure the QoL of Eastern and Western caregivers. The QoL scores of French, 24 American, 26 and Korean caregivers measured by CarGOQoL were relatively similar at 65.0, 67.6, and 69.3, respectively, and were the lowest in the Psychological well-being, Private life, and Leisure time domains in all cultural contexts. However, in the case of the Self-efficacy domain, American 26 and French 24 caregivers scored 74.1 and 73.3 points, respectively, which were relatively high compared to other domains, but Koreans showed the lowest Self-efficacy score of 63.4 points. The Self-efficacy domain, which could not be measured in the existing questionnaires, could be measured through this tool. Considering Korean Confucianism, it is considered immoral for a family caregiver to express resentment and entrust the care of a patient to someone else. In addition, most Korean caregivers were middle-aged; the average age of caregivers was 49 years old, and they were not yet old enough to retire. Therefore, if they lack social support, their caring experience can be overloaded. The lower the social support perceived by caregivers, the lower their self-esteem tends to be. 13 In the case of Korean caregivers, it is thought that their Self-esteem domain scores were low because the scores in the Social support domain were relatively low compared to the scores in other domains.
To assess the criterion validity of the 29-item K-CarGOQoL, we analyzed the correlations between the Korean version of the WHOQOL-BREF, QoL (VAS), and burden (VAS). During this study, burden (VAS) was used to evaluate the variables for “stress which is perceived by caregivers due to the home care situation,” which has been suggested by previous studies to be closely related to the QoL of informal caregivers of patients with cancer.39-41 Additionally, the WHOQOL-BREF evaluates attributes that are similar to those evaluated by the CarGOQoL because it measures the physical, psychological, and social relationship QoL, 28 whereas the CarGOQoL measures the degrees of psychological and physical well-being and social support. 24 Therefore, this work suggests that the WHOQOL-BREF and burden (VAS) can adequately verify the criterion validity of the CarGOQoL. Significant correlations were found between the CarGOQoL and WHOQOL-BREF (r = .495-.607), QoL (VAS) (r = .509), and burden (VAS) (r = −.457), which, based on the recommended correlation coefficient range (r = .40-.80), 42 satisfactorily established the criterion validity.
Finally, this study was the first to evaluate the known-group validity of the 29-item K-CarGOQoL instrument. In particular, the QoL scales captured the influence of the health status by producing ratings that varied between groups in ways that were predicted by a prior study. 43 Previous research has shown a strong relationship between the physical performance level of patients with cancer and the QoL of informal caregivers. In other words, informal caregivers report better QoL when the physical performance level of patients with cancer is lower.44,45 Therefore, a significant difference in the QoL between groups with various physical PS would suggest the known-group validity of the CarGOQoL. This study analyzed the variations in the mean QoL scores for each group according to the ECOG PS classification. The known-group validity of the CarGOQoL instrument was considered proven because groups with a poor physical PS had better QoL.
This study verified the validity and reliability of the 29-item K-CarGOQoL, which was created exactly like the original instrument and did not exclude any items. Additionally, by examining the score for each subcategory, the QoL degree may be comprehended in greater detail because the reliability and validity between each substructure were confirmed (Psychological well-being, Burden, Relationship with health care, Administration and finances, Coping, Physical well-being, Self-esteem, Leisure time, Social Support, and Private Life). This is advantageous because the QoL among informal caregivers of patients with cancer can be compared with that of informal caregivers of patients with cancer from other countries and cultures.
However, this study had some limitations. First, it was conducted using a convenience sample from a single tertiary university hospital. Therefore, generalization of the research results may be limited. Multicenter studies with larger sample sizes should be performed in the future. Second, caregivers can be divided into formal caregivers, who are paid for their services, and informal caregivers, also called family caregivers. 20 In this study, the cultural suitability and validity of the tool for informal caregivers were verified. We suggest further studies verifying the validity and reliability of the tool for general caregiver population, including formal caregivers. And, third, the original French version analyzed the infit (inlier-sensitive or information-weighted fit) using the Rasch model. Therefore, an item response theory analysis of the Korean version of the tool should be performed.
Conclusion
The validity and reliability of the scale were verified for the first time in Korea. This study demonstrated that the 29-item K-CarGOQoL is appropriate for measuring the QoL of Korean informal caregivers of patients with cancer. The 29-item CarGOQoL assesses specific characteristics of informal caregivers of patients with cancer, such as self-esteem and private life, that are not measured by existing questionnaires; therefore, it can be used to effectively evaluate the QoL of this population. In addition, the 29-item K-CarGOQoL scale can be useful in Korean oncology clinical practice and research when assessing the QoL of informal caregivers of patients with cancer. We suggest conducting further research to generalize to the general caregiver population, including formal caregivers.
Footnotes
Acknowledgements
None
Authorship Statement
Conceptualization, EK, HYK, WKB, and JEH; methodology, EK, HYK, WKB, and JEH; formal analysis, HYK; investigation and data curation, WKB and JEH; writing—original draft, EK and HYK; writing—review and editing, EK, HYK, WKB, and JEH. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Institutional Review Board Statement
The study design was approved by the Institutional Review Board of Chonnam National University Hwasun Hospital (IRB) prior to data collection (IRB file no. CNUHH-2019-023).