
Abstract
Theoretical models to explain health service utilization are numerous and there is no known literature that has synthesized existing models for health service utilization. Systematic searches were conducted in PubMed, MEDLINE, PsychINFO, Scopus, and CINAHL databases from 1960 through May 2021. Literature theorizing models/frameworks for health service utilization were included. Multiple investigators screened citations and full texts. Data extracted included: (1) citation information, (2) purpose of models, and (3) major constructs of models. The search retrieved 6639 citations. A total of 34 articles were eligible for this review. Theoretical models were categorized into 4 thematic domains based on the purpose of the model: (1) generalized health service utilization, (2) health service utilization with respect to specific sociodemographic determinants of health, (3) health service utilization specific to illness or health disciplines, and (4) preventive health services/screenings. There was an increase in models developed over time with a trend toward model development specific to sociodemographic determinants of health, illness, and/or health disciplines. This review cataloged theoretical models for health service utilization by thematic domain to enhance the identification and critical review of existing models. Findings support the notion that theoretical pluralism has been adopted in the field of health service utilization.
Several theoretical models exist in attempt to describe health service utilization.
This scoping review synthesized the literature on theoretical models to explain health services utilization and demonstrates theoretical pluralism across available models.
This research aids future researchers and policymakers by cataloging available theoretical models to describe health service utilization that may be adopted and applied to specific contexts.
Introduction
Health service utilization has been described as the product of interactions between healthcare professionals, the generation of health services, and patients. 1 At the most basic level, health service utilization is determined by the need and supply of health services. 2 However, health service utilization is significantly more complex and multidimensional with many underlying factors potentially playing a role in the health service utilization process. 1
The delivery of healthcare contributes toward individual, community, and population level health outcomes. 3 Therefore, research efforts to understand the health service utilization process are important to equitably deliver high-quality health services to all individuals, communities, and populations. To guide health services research, theoretical models to explain health service utilization are necessary. Use of theoretical models in empirical designs and concepts can act to substantially improve empirical design and outcomes for researchers. According to Mechanic, use of theoretical models that represent the realities of the provisions of health service utilization is essential to performing high-quality health services research. 4
Theoretical models to explain health service utilization are numerous and there is no known literature that has synthesized existing models for health service utilization. Therefore, the purpose of this study was to: (1) synthesize the peer-reviewed literature on theoretical models used to explain health service utilization, and (2) describe the characteristics of existing models. This study demonstrates the span of available theoretical models in this field, describes themes and major constructs of existing models, and aids the development of future research and decision making related to various contexts of health service utilization.
Methods
In accordance with recommendations by Munn et al a scoping review methodology was selected. 5 We aimed to clarify concepts and identify key characteristics related to concepts in order to inform future research. 5 This review was conducted in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews (PRISMA-ScR). As outlined by Arskey and O’Malley, 6 and Levac et al, 7 this review was performed in 5-stages. This review was not registered prior to undertaking it as protocols do not require registration of scoping reviews.
Stage 1—Identifying the Research Question
This review addressed the following research questions:
What theoretical models have been used to explain health service utilization in peer-reviewed scientific literature?
What are the key characteristics that define existing theoretical models for health service utilization?
Stage 2—Identifying Relevant Studies
A literature search was performed on May 19, 2021 of the following databases from 1960 through May 19, 2021: PubMed, MEDLINE, PsychINFO, Scopus, and Cumulative Index of Nursing and Allied Health Literature (CINAHL). A variety of terms related to health service utilization, conceptual and theoretical models, and frameworks were combined for the database search (Table 1). Investigators were asked to identify additional studies in which they were familiar, but which were missing from the formal search. Grey literature was not included in this study. Literature identified in this search was downloaded to Zotero and duplicates were removed.
Database Search Example.

Stage 3—Study Selection
Eligibility criteria
English-language literature discussing theoretical models for health service utilization were included in this review. Consistent with a prior literature review that assessed theoretical models in a specific field, this review focused on literature that had a primary objective to: (1) describe a theoretical model to explain health service utilization, or (2) describe a modification of a previously identified theoretical model used to explain health service utilization. 8 We narrowed our eligibility to only include papers which theorized health service utilization models/frameworks. Studies which described the application of existing theoretical models to a specific health condition or setting were ineligible for this review. Experimental, observational, and cross-sectional study designs that included the testing or development of theoretical models were ineligible for this review. Lastly, literature reviews comparing theoretical models were ineligible for this review.
Article selection
De-duplicated citations were uploaded from Zotero to Rayyan 9 for screening of title/abstracts. One investigator independently screened titles and abstracts for evaluation against the eligibility criteria. For quality assurance a second investigator independently screened a random 10% sample of titles and abstracts for evaluation against the eligibility criteria, with a 97.8% agreement seen between investigators. Titles and abstracts that met eligibility criteria were saved and underwent independent full text screening for eligibility. Two investigators independently screened full texts for evaluation against eligibility criteria. Disagreement on eligibility was resolved by discussion and refereed by a third investigator when necessary.
Stage 4—Charting the Data
Data items & data extraction
One investigator independently analyzed the attributes of theoretical models identified in eligible literature. With consideration from a prior review which analyzed theoretical models in a specific field, the following items were extracted: (1) information of eligible literature (citation, first author, and year of publication), (2) purposes of models, and (3) major constructs of models. 8
Methodological quality (risk-of-bias) assessment
The aim of this review was to catalog and describe theoretical models which have been used to conceptualize health service utilization. Therefore, methodological quality (risk-of-bias) evaluations were not necessary to answer the research questions and were not performed in this study.
Stage 5—Collating, Summarizing, and Reporting Results
Descriptive numeric summary
Characteristics of eligible literature were described in a brief numeric summary, including number of identified models and associated citation information.
Qualitative thematic narrative
A qualitative thematic narrative was organized by key thematic characteristics of theoretical models. Key characteristics for each of the individual theoretical models were recorded. Key characteristics were identified as described and depicted by the authors from each of theoretical models identified in eligible literature in this review. One investigator applied codes to the key characteristics for each theoretical model. Potential themes were identified from codes and sorted according to potential themes. Individual theoretical models were not restricted to a single theme and could be sorted into multiple themes. Themes were iteratively reviewed and refined until themes were named and defined.
Results
A comprehensive database search identified 6639 citations. No articles were identified through a hand search. A total of 1913 duplicates were removed. After removal of duplicates, 4726 citations were screened and 4607 were excluded based on title/abstract irrelevance. A full-text review of the remaining 119 citations resulted in 85 articles excluded due to: wrong outcome (n = 62), wrong study design (n = 15), unavailability of full text (n = 7), and wrong publication type (n = 1). A total of 34 articles met inclusion criteria and were eligible for this review. The study selection process is illustrated in Figure 1.

PRISMA flow diagram.
Review of the 34 theoretical models in this review revealed 4 major thematic domains, based on the purpose of the models: (1) models to explain generalized health service utilization, (2) models to explain health service utilization in respect to consideration of specific sociodemographic determinants of health, (3) models to explain health service utilization in respect to illness or specific health disciplines, and (4) models to explain health service utilization for preventive health services/screenings.
Several theoretical models were categorized under multiple thematic domains. A total of 4 theoretical models were classified under the thematic domain to explain generalized health service utilization.10-13 A total of 24 theoretical models were classified under the thematic domain to explain health service utilization with consideration of specific sociodemographic determinants of health.14-37 Eighteen theoretical models were categorized under the thematic domain to explain health service utilization in respect to illness or specific health disciplines.15,17,18,22-27,31,34,37-43 Lastly, 2 theoretical models were categorized under the thematic domain to explain health service utilization for preventive health services/screenings.18,25 The distribution and major constructs of the theoretical models within each of the 4 thematic domains were summarized in Tables 2 to 5.
Theoretical Models to Explain Generalized Health Service Utilization.

Major constructs of theoretical models as depicted by the authors.
Theoretical Models to Explain Health Service Utilization in Respect to Consideration of Specific Social Determinant(s) of Health.

Major constructs of theoretical models as depicted by the authors.
Theoretical Models to Explain Health Service Utilization in Respect to Illness or Specific Health Discipline(s).
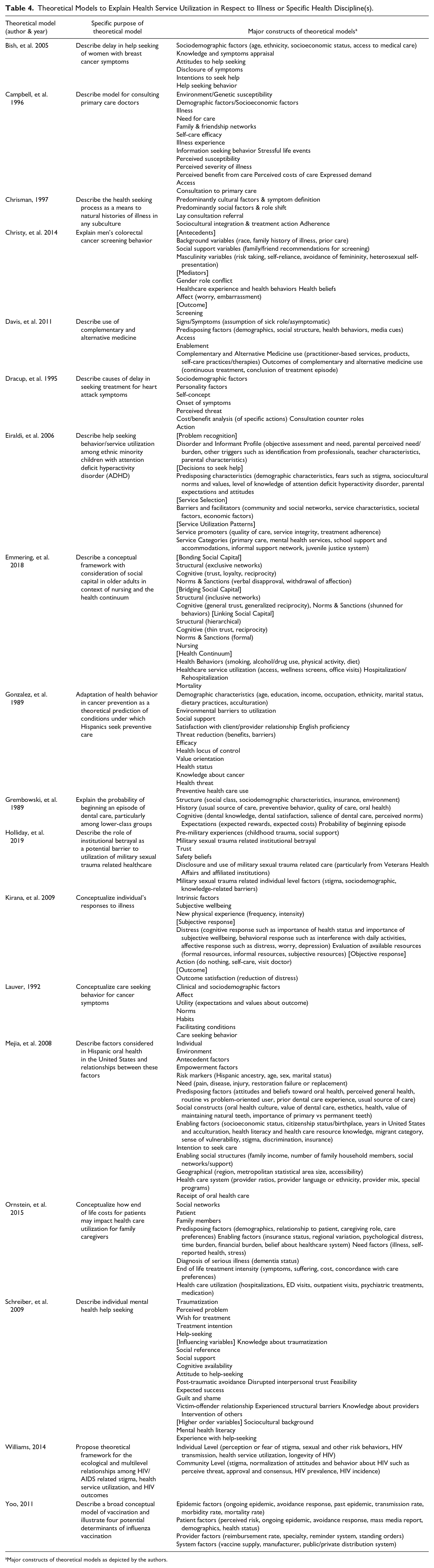
Major constructs of theoretical models as depicted by the authors.
Theoretical Models to Explain Health Service Utilization for Preventive Health Service(s)/Screening(s).

Major constructs of theoretical models as depicted by the authors.
There was an increasing trend of theoretical models published between 1981 and 2019 that conceptualized health service utilization in context of specific sociodemographic determinants of health, illness and/or health disciplines (Figure 2). Each of the 4 theoretical models explaining generalized health service utilization were published before the year 2010.

Thematic distribution of theoretical models for health service utilization by year of publication.
Thematic Domain 1: Models to Explain Generalized Health Service Utilization
Theoretical models under this thematic domain explained health service utilization which can be applied to a variety of contexts.10-13 Models described by Andersen included major constructs of environmental factors (ie, health system factors), population/contextual factors (ie, sociodemographics), and individual health behavior factors and outcomes.10,11 Magi and Allander described a theoretical model that includes consideration of both patient and physician perspectives. 12 Kufafka, et al. presented a cognitive model that considers patient decision making contributing toward the explanation of health service utilization. 13 It is noteworthy that although diverse lexicon is used for core sociodemographic, health behavior, and health system factor constructs in models classified under thematic domains 2, 3, and 4, these core constructs are similar, if not derived, from early models categorized in thematic domain 1.
Thematic Domain 2: Models to Explain Health Service Utilization With Respect to Specific Sociodemographic Determinants of Health
Theoretical models in this thematic domain described health service utilization in context of specific sociodemographic determinants of health.14-37 Common sociodemographic determinants of health that were considered in these models included (sub)cultural factors, gender groups, age groups, race/ethnicity populations, access to healthcare, health disparities, geography, low-income/low-literacy populations, socioeconomic factors, and family/caregiver groups. Arnault described cultural determinants of health seeking. 14 Carillo, et al. described a model of health care access barriers that are associated with health care disparities. 16 Many of these models included core constructs such as demographic, health behavior, and health system factors. However, most models diverged from each other with the inclusion of model constructs that are specific to the sociodemograhpic determinants of health consideration for each model.
Thematic Domain 3: Models to Explain Health Service Utilization Specific to Illness or Health Disciplines
Theoretical models categorized under thematic domain 3 explained health service utilization in context of illness or specific health disciplines.15,17,18,22-27,31,34,37-43 Similar to models under thematic domain 2, several of the models in this thematic domain included core constructs of sociodemographic, health behavior, and health system factors; however, most models differed from each other with the inclusion of model constructs that are specific to the illness and/or health discipline consideration.
Illness considerations included cancers, oral health, end of life considerations, mental health, heart attack, attention deficit hyperactivity disorder, and HIV/AIDS. Bish et al, proposed a theoretical model to describe the delay in help seeking of women with breast cancer. 15 Christy et al proposed a theoretical model to explain men’s colorectal cancer screening behavior. 18 Dracup et al proposed a theoretical model to describe causes of delay in seeking treatment for heart attack symptoms. 22
Health discipline considerations included primary care, complementary and alternative medicine, mental healthcare, dental care, nursing, military sexual trauma related care, and vaccinations. Campbell and Roland described a model for consulting primary care doctors. 38 Davis et al proposed a model to explain the use of complementary and alternative medicine. 39
Thematic Domain 4: Models to Explain Health Service Utilization for Preventive Health Services/Screenings
Theoretical models under this thematic domain intended to explain health service utilization specific to preventive health services and health screenings.18,25 Christy et al proposed a theoretical model to explain men’s colorectal cancer screening behavior. 18 Major constructs of this model included background (ie, demographics), social support, masculinity, and mediating (ie, health behaviors, health beliefs, healthcare experience) variables. 18 Gonzalez, et al proposed an adaptation of the health behavior in cancer prevention model to explain conditions in which Hispanics seek preventive care. 25 Similarly, this model included demographic, social support, and patient-provider relationship experience variables to explain preventive health service utilization. 25
Discussion and Implications
This review of the peer-reviewed literature, the most comprehensive we are aware of, identified 34 theoretical models for health service utilization. Twenty-three of the 34 models have been published since the year 2004. Theoretical models were categorized by model purpose into 4 thematic domains: (1) generalized health service utilization models, (2) models adapted for specific sociodemographic determinants of health, (3) models adapted for specific illness or health disciplines, and (4) models adapted for preventive health services and screenings. Most models were proposed in context of specific sociodemographic determinants of health, illness, and/or health discipline considerations, with an increasing trend of these types of contextually focused models. Though a wide array of terminology was used across models, many of the models in this review were comprised of core constructs related to sociodemographic, health behavior, and health system factors.
This review suggests the seminal work toward theoretical model development by Andersen has contributed to lasting core constructs (sociodemographics, health behaviors, health system factors) in existing theoretical models to explain health service utilization.10,11 Iterations of theoretical models for health service utilization have routinely incorporated these core constructs with additional adaptations to account for contextualization of the specific model’s purpose. These additional contextual adaptations include sociodemographic determinants of health, illness, and/or health disciplines. Though not necessarily theoretical models intended to describe health service utilization, other core concepts from seminal papers on access and quality of care have also been widely incorporated into theoretical models for health service utilization.44,45
The increasing quantity of adapted iterations of models may be influenced by the evolution toward theoretical pluralism in the social sciences and systemic action research, such as implementation science.8,46 Theoretical pluralism has been described as a widely accepted and preferred pragmatic approach to systemic action research by allowing one to view multiple theoretical “lenses” involving differing assumptions. 46 A pluralistic theoretical approach is argued to support actionable decision-making for multiple stakeholders, such as policy makers and health administrators. 8 Accordingly, a pluralistic approach to theory development is argued to be an essential skill for researchers. 8 It has been contended that in order to provide an easily interpretable theory which can provide explicit justification for implementation strategies, detailed attention to theory development is essential.8,47-49
Health services research, particularly that which concentrates on implementation science to address differences in health service utilization across populations, inherently demands a pluralistic approach to the application of theoretical models. Implementation science is fundamentally an applied field that is employed in and across dynamically changing and diverse environments. 50 Thus, the significant increase in iterations of theoretical models for health service utilization that are adapted for specific contextual factors likely goes hand in hand with the adoption of theoretical pluralism within social science and systemic action research.
Conversely, as the health services research field has adopted a pluralistic approach to theory, there could be risk of hindering meaningful theoretical iterations and reducing clarity.8,49 Healy suggests there is an anti-theoretical nature of nuance in sociological theory development and warns against falling into “nuance traps.” 49 Healy asserts that employing iterative nuance to theory actually inhibits the process of abstraction—which theory is contingent upon—and impedes creativity as a useful theoretical process. 49 Not only could a nuance-driven approach to theory development potentially hinder creativity and distract from theoretical problem solving, it may foster the perpetuation of nuanced theoretical models which could attenuate conceptual clarity over time.8,47,48 Findings from this review illustrate the potential for confusion caused by the existence of a vast quantity of models and the varying terminology representing similar constructs across models. As the collection of theoretical models for health service utilization continues to expand, it is important for researchers to critically assess existing models and develop clear and consistent language that can be used in incipient models.
Limitations
This review has notable limitations. Non-English language articles in this review were excluded which may have resulted in missing relevant theoretical models. While an extensive and robust search methodology was performed, this review did not include a search of “grey literature.” This may have resulted in relevant theoretical models being missed. We acknowledge this review did not include theoretical models that are not explicitly conceptualized as models to describe health services utilization, though can be applied to explain health service utilization. For example, the health belief model and other ecological models can be used to explain health service utilization, particularly in respect to specific sociodemographic determinants of health, illness, and health discipline considerations. In addition, this review did not include articles of experimental, observational, and cross-sectional study designs that tested the development of theoretical models. Inclusion of these models would likely have yielded a significantly greater number of theoretical models. This would likely have further strengthened our argument of the increasing dilution of clarity in this field from an expanding number of proposed models with varying terminologies.
Conclusions
This scoping review of the peer-reviewed literature cataloged and described models for health service utilization. Findings of this review were organized into thematic domains to allow for easy identification and comparison of models to be selected to guide research, policy, and decision making. Findings from this review reaffirm an evolution toward theoretical pluralism with increasing quantity of model iterations that consider specific sociodemographic determinants of health, illness, and/or health disciplines.
Footnotes
Acknowledgements
The authors acknowledge health services librarian Elizabeth Suelzer, MLIS, AHIP (Medical College of Wisconsin Libraries, Medical College of Wisconsin, Milwaukee, Wisconsin, USA) in executing the searches and uploading citations to Zotero and Rayyan for this scoping review.
Authors’ Contributions
JAG, ALS, MJS, JW, and SY contributed to concept development and study design. JAG and SY contributed to the literature search in conjunction with a health services librarian. JAG, ALS, and SY contributed to abstract, title, and full text screening for eligibility. JAG contributed to data extraction and data charting. JAG, ALS, JW, MJS, and SY contributed to data analysis. JAG drafted the manuscript. JAG, ALS, JW, MJS, and SY critically revised the manuscript for intellectual content and contributed to manuscript revisions. All authors approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Availability of Data and Material
All data collected are included and described in this manuscript.
Ethical Approval
No portion of this paper has been presented or published elsewhere. Our study did not require ethical board approval because it is a scoping review design.