
Abstract
Determinants of mask-wearing during a pandemic range from the personal to the political. Using a repeated measures design, we examined psychosocial predictors of self-reported mask-wearing 3 times during the early stage of the COVID-19 pandemic. Participants completed surveys at baseline (summer 2020), 3 months (fall 2020), and 6 months (winter 2020-2021). The survey assessed the frequency of mask-wearing and psychosocial predictors from various theories, including fear of COVID-19, perceived severity, perceived susceptibility, attitude, health locus of control, and self-efficacy. Results indicated that the strongest predictors of mask-wearing varied as a function of the stage in the pandemic. In the earliest phase, fear of COVID-19 and perceived severity were the strongest predictors. Three months later, attitude was the strongest predictor. Finally, another 3 months later, self-efficacy became the strongest predictor. Overall, the results suggest that the primary determinants of a novel protective behavior shift over time and with increased familiarity.
Studies have shown both the benefits of mask-wearing for COVID-19 prevention and that mask-wearing varies as a function of multiple legal, societal, interpersonal, and intrapersonal levels.
This longitudinal study has advanced our understanding of preventive health behaviors; specifically, the study has demonstrated how individuals adopt preventive behaviors in pandemic situations and how predictors of such adaptation (ie, decision-making) change over time.
Longitudinal approaches to studying associations among psychosocial variables and behaviors can further enhance our knowledge of how people adapt to new health threats and challenges.
Since the outbreak of the coronavirus disease (COVID-19) in late 2019, the COVID-19 pandemic has spread to 6 continents, causing millions of deaths worldwide. 1 The lack of a vaccine and effective treatments during the early phases of the pandemic enhanced the need for behavioral prevention strategies such as mask-wearing, social distancing, hand-washing, and isolation at home.2,3 Like all preventive measures, people’s willingness and ability to engage in these behaviors varied based on factors ranging from personal beliefs to nationality.4-8 For example, Latkin et al 7 found that COVID-19 skepticism reduced engagement in COVID-19 prevention behaviors, whereas Anaki and Sergay 6 (described below) found variation in prevention behaviors by country.
The present paper focuses on traditional psychosocial predictors (eg, fear, attitudes, and self-efficacy) in relation to mask-wearing to prevent the spread of COVID-19 in a sample of Americans residing in the desert southwest. We first review the rapidly evolving research on psychosocial predictors of COVID-19 prevention behaviors before turning to the rationale for the present study.
Psychosocial Predictors of COVID-19 Prevention Behaviors
Several studies have examined psychosocial predictors of COVID-19 prevention measures. The psychosocial factors examined in these studies included constructs such as attitudes, perceived severity and susceptibility, self-efficacy, and fear. Many of these concepts reflect traditional health promotion theories, such as the Theory of Planned Behavior, 9 the Health Belief Model, 10 and Social Cognitive Theory. 11
To varying degrees, masks have limited the spread of the coronavirus and offered effective protection from contracting the virus to both the wearer and others. 12 Moreover, when combined with social distancing, masks have proven to be even more effective. 12 Mask-wearing was common; at the peak of the pandemic (eg, September 2020), 85% of US adults reported wearing a mask “all or most of the time” when they were inside stores or businesses. Of them, 74% reported “always wearing a face mask” when they were outside of their homes. 13 Mask-wearing was also effective; COVID-19 mortality rates were higher in regions that were slow to adopt mask-wearing mandates compared with regions quicker to adopt them.13-19
The strongest predictor of mask-wearing included legal mandates and possession of a college degree. Women, adults over 65, non-white racial groups, and those identifying as democrats were also more likely to wear masks. 13 Psychological factors such as perceptions of risk, the observed behavior of others, concern for self-protection and protection of others, and perceptions of the judgment of others when wearing a mask were also found to be significant predictors of mask-wearing.6,20-22
Anaki and Sergay, 6 for example, examined predictors of preventative health behaviors among 953 participants who completed an online survey that assessed perceived severity, perceived vulnerability, feelings of anxiety, attitudes toward COVID-19 (proactive, overestimation, passivity, and avoidance), intentions to take preventive measures, and protective behaviors already implemented by the participants. The most common proactive measures included washing hands (62.5%), followed by avoiding crowded places (54.4%), and distancing oneself from people with symptoms such as coughing and sneezing (48.5%); less than a third (30.3%) reported wearing face masks. Mask-wearing related positively to age, education, marital status (married > single), full-time employment, and location (Asia > N. America > Europe). Regarding the prediction of preventive behaviors, the authors examined proactive behavior as an aggregate construct rather than examining each behavior individually. Predictors of aggregate behavior included emotions such as worry, threat over-estimation by the government (negatively), media (negatively), and avoidance (ie, social distancing). Unfortunately, this study did not report predictors of individual health behaviors such as mask-wearing.
Courtice et al 20 examined the adoption of mask-wearing and attitudes toward mask-wearing mandates using a daily diary methodology. A total of 1712 Canadians participated in a 28-day study that tracked their COVID-19 Experiences in May 2020. The results showed increased mask-wearing behavior and attitudes toward mandates over the 28 days. Furthermore, those who perceived the pandemic as more serious showed higher levels of mask-wearing and attitudes toward mask mandates. Finally, political affiliation proved to be a strong predictor of attitudes toward mask mandates, with liberal-leaning participants having had more positive attitudes toward mask mandates than conservative-leaning participants. The authors recommended cohesive, non-partisan messaging during public health crises.
Oliver et al 21 also examined predictors of attitudes toward mask-wearing. Specifically, they investigated whether uplifting media messages could create universal orientation and prosocial behavior and how the latter related to mask-wearing attitudes. They also examined political affiliation (Republican vs Democrat) as a potential moderator. Participants viewed 1 of 3 video messages, one featuring an uplifting message, one featuring an uplifting message with patriotic messages, and a control video. Regardless of political affiliation, participants found the uplifting messages more inspiring and resulted in higher universal orientation and prosocial motivation. Among Republicans, a universal orientation was associated with more positive attitudes toward mask-wearing, whereas among democrats, prosocial motivations led to more favorable attitudes.
In summary, studies have shown both the benefits of mask-wearing for COVID-19 prevention and that mask-wearing varies as a function of multiple legal, societal, interpersonal, and intrapersonal levels. Also, most studies have been cross-sectional, thereby providing only brief snapshots at a specific point in time. Most individuals in the US have never had to respond and cope with the uncertainties and implications of a global pandemic, particularly one with such deadly force. As such, we would expect not only significant changes in psychosocial factors across time but also expect the association of these factors to preventive behaviors such as mask-wearing to change over time and as people learned more about the virus and how to prevent it.
Accordingly, the present study investigated several psychosocial predictors of mask-wearing at 3 different times early in the pandemic: The summer of 2020, the fall of 2020, and the winter of 2020/2021. Participants in the present study completed surveys 3 times during this period. We hypothesized that variables related to fear and threat would positively relate to mask-wearing in the early phases as an immediate response to stress, but that the effect of these variables would wane as time progressed and people learned to cope with the virus. As time marched on, we predicted that fear of COVID-19 would wane and that other variables, such as attitudes toward the behavior and self-efficacy to perform, would emerge as positive predictors of mask-wearing behavior.
Method
Participants
Participants in this study were 95 individuals from a university in the Southwestern United States, including faculty (n = 26), staff (n = 29), students (n = 27), and administrators (n = 11), with n = 2 “others.” Participants were included in the study if they were 18 years of age or older and having faculty, student, or staff status at the university. There were no explicit exclusion criteria. The sample had a mean age of 46.5 (SD = 15.0), was 52% female, 78% White/Caucasian, and 26.3% Hispanic. The sample was highly educated; 83.2% had a college degree or higher. Most participants were married or cohabitating (74%), and the median income range was $75 000 to $90 000. Since this study involved symptom monitoring and reporting in collaboration with a healthcare technology company, enrollment was limited to 100 participants.
Measures
Demographics
Demographics included age, sex, ethnicity, marital status, level of education, and household income.
Engagement in COVID-19 prevention behaviors
We assessed engagement in COVID-19 prevention behaviors (eg, quarantining, mask-wearing, hand-washing, social distancing, etc.) using a 5-item self-report instrument. The specific behavior assessed in this study was, “In the past 30 days, how often have you worn a face covering or mask when you were around others,” and respondents rated it from 1 to 7 as never to every day.
Attitudes toward COVID-19 prevention behaviors
We assessed attitudes toward mask-wearing using a 3-dimension semantic differential scale. Specifically, the question read, “For me, wearing a face covering or mask when I am around others is,” and respondents rated it from 1 to 7 as harmful versus beneficial, pleasant versus unpleasant (recoded), and good versus bad. Table 1 shows that the 3-item scale displayed acceptable reliability at all 3-time points.
Means, SDs, Alpha, and Correlations for Demographics and Main Study Variables at 3 Study Points.
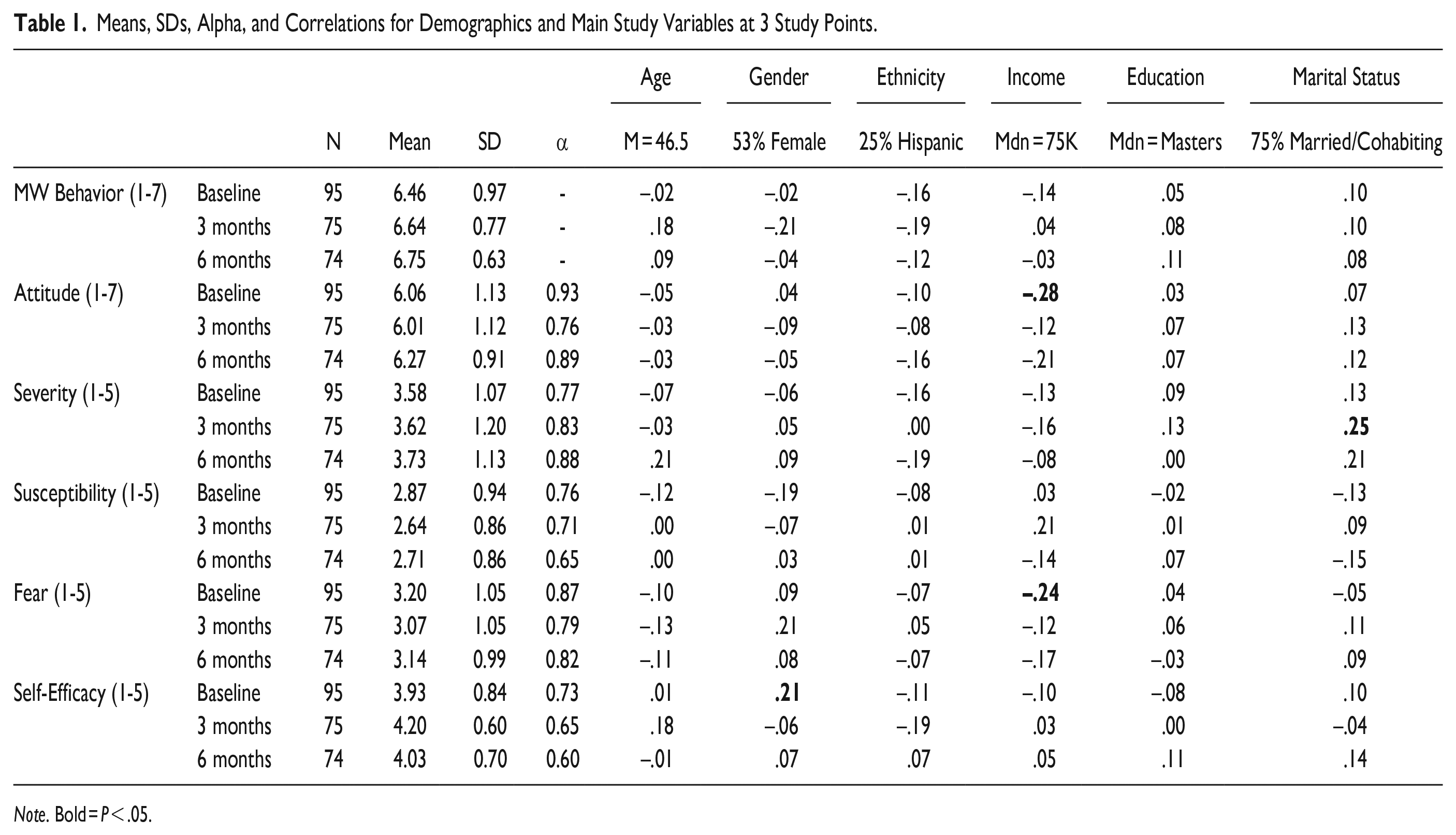
Note. Bold = P < .05.
Perceived susceptibility and severity to COVID-19
We assessed perceived susceptibility and severity of COVID-19 using 4 items based on Rubin et al 23 For severity, participants responded to 2 items assessing, “Do you think that COVID-19 is a matter of life and death?” and “I think that if I contract COVID-19, it will have major consequences on my life.” For susceptibility, the items included, “I believe I am at high risk of catching COVID-19,” and “How likely do you think it is that you will contract COVID-19 over the next month?” All 4 items were rated on 5-point scales ranging from extremely unlikely to extremely likely. Table 1 shows that both scales displayed acceptable reliability at all 3 time points.
The fear of COVID-19
We assessed fear of COVID-19 using 3 items based on Ahorsu et al 24 The items included, “I am afraid of the coronavirus,” “It makes me uncomfortable to think about the coronavirus,” and “When I watch news and stories about the coronavirus, I become nervous or anxious.” All 3 items were rated on 5-point scales ranging from strongly disagree to strongly agree. Table 1 shows that the scale displayed acceptable levels of reliability at all 3 time points.
Self-efficacy to avoid COVID-19 infection
We assessed self-efficacy beliefs using items based on Cho and Lee. 25 The items included, “I am confident in my ability to protect myself from COVID-19,” I am unable to protect myself from COVID-19″ (recoded), and “I am confident that I can carry-out COVID-19 precautionary actions.” Respondents rated each item on 5-point scales ranging from strongly disagree to strongly agree. Table 1 shows that the scale displayed acceptable levels of reliability at all 3 time points.
Procedure
During the early stages of the pandemic, we recruited individuals from the university setting to participate in a COVID-19 longitudinal symptom monitoring study. Each participant took their own temperature and pulse oxygen readings each day for 6 months. They also completed several health and psychosocial measures, including those described above, at study intake, after 3 months of symptom monitoring, and a final time at 6 months. All self-report scales were validated in various disease contexts, but not specifically in the context of COVID-19 (As such, the instruments used in this study should not be seen as duplicates of their originals). We used Qualtrics surveys for the assessment of all psychosocial variables. Active participation in the study began in June 2020 and ended in January 2021. This report focuses on psychosocial variables. A university in the Southwestern United States served as the setting for the study. The University IRB (Institutional Review Board) reviewed and approved the study and all participants provided written informed consent before participation. The authors had no conflict of interest to conduct and report the results of this study.
Results
Descriptive Statistics and Zero-Order Associations
Table 1 shows means, standard deviations, reliability estimates, and intercorrelations for the main study variables at all 3 assessment points. As shown, the sample had a mean age of 46.5 years, was 53% female, 35% Hispanic, and had a median income in the 75-100K range. Over half reported a median education level of a master’s degree or higher, and about 75% were currently married or cohabitating. Coefficient α’s were acceptable, particularly given the small number of items on each scale. Mask-wearing behavior was high at all 3 time points, as were attitudes toward it. Average severity ratings were above the scale midpoint, whereas susceptibility ratings were lower. Fear scores were also near the scale midpoint. Interestingly, the means for most variables remained stable over time.
Table 1 also shows correlations between the demographics and behavioral and psychosocial variables. As shown, age and income showed modest correlations with some of the psychosocial variables but, overall, the demographic variables were not strongly associated with most variables. Given these results, we kept age and income as covariates in further analyses.
Table 2 shows the intercorrelations among measures. Mask-wearing behavior correlated positively with attitudes toward mask-wearing, perceived severity, and susceptibility (except for the 6-month assessment). In general, attitudes, severity, susceptibility, and fear correlated positively and substantially suggesting considerable shared variance among these constructs at all 3 time points. In contrast, self-efficacy correlated minimally with the psychosocial variables and mask-wearing at baseline and 3 months. However, self-efficacy correlated strongly with mask-wearing behavior at 6 months.
Intercorrelations of Psychosocial Variables and Mask-Wearing Behavior at 3 Points in The Pandemic.
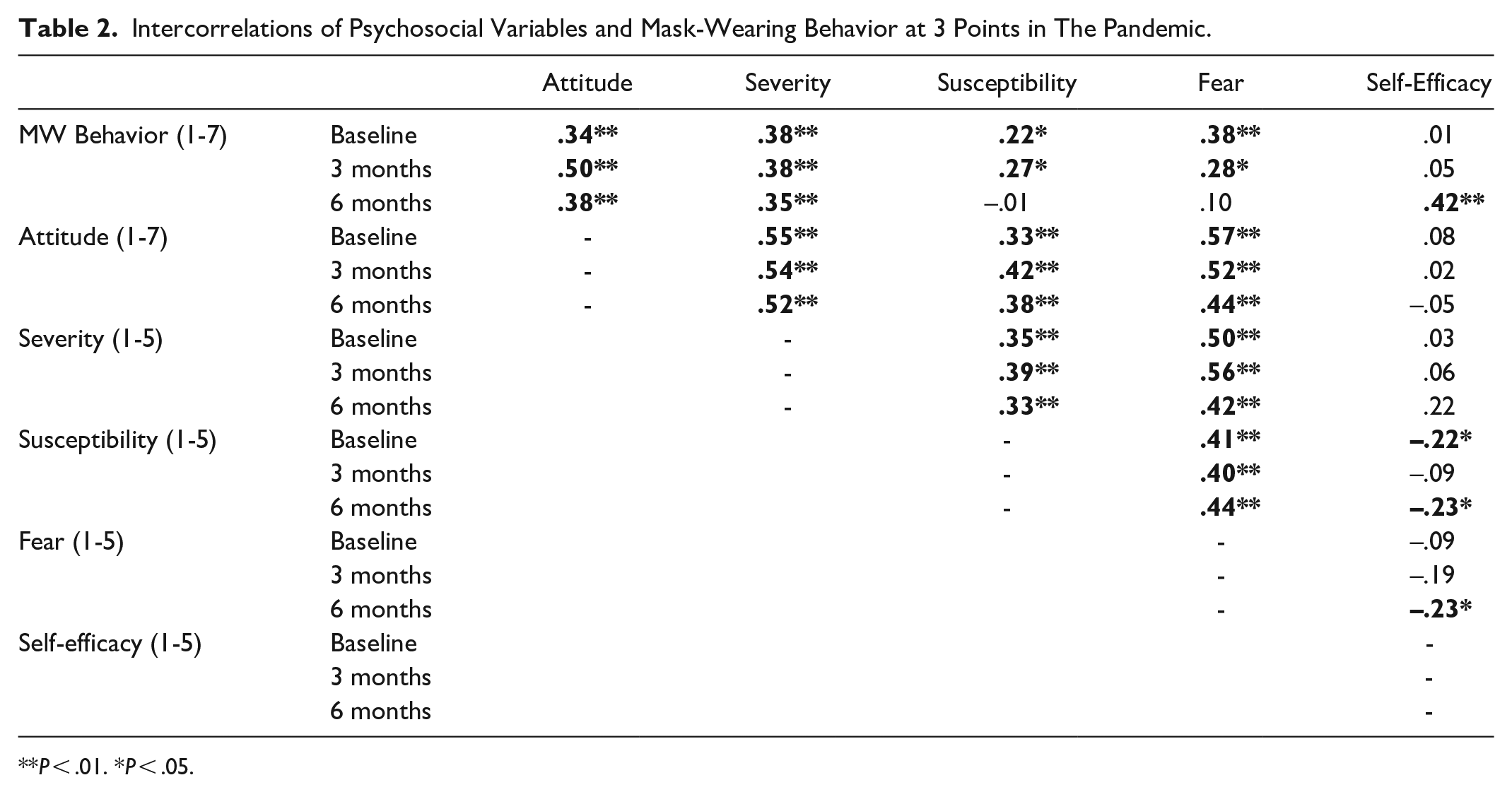
P < .01. *P < .05.
Multivariate Prediction of Mask-Wearing Behavior
Table 3 summarizes the results of standard regression analyses examining the multivariate associations between the psychosocial predictors and mask-wearing behavior. All 3 analyses controlled for age and income. Overall, R 2 effect sizes increased from baseline, R 2 = .17, to 3 months, R 2 = .21, to 6 months, R 2 = .28, suggesting greater prediction over time. At baseline, none of the psychosocial variables predicted independent variance in mask-wearing behavior. At 3 months, only attitude predicted independent variance in behavior. Finally, at time 3, self-efficacy emerged as the only variable to predict independent variance in behavior. It is important to note that the lack of significant regression coefficients, particularly at baseline, does not mean that the variables were unrelated to mask-wearing per se, but that none or one predictor, depending on the time frame, contributed uniquely to such prediction.
Psychosocial Predictors of Mask-Wearing Behavior at 3 Points in the Pandemic Controlling for Age and Income.

Note. Bold = significant coefficients.
Discussion
This study examined psychosocial variables as predictors of self-reported mask-wearing behavior in response to the COVID-19 pandemic. Moreover, the study assessed such associations at 3 time points as the pandemic emerged in the US, including the summer of 2020, the fall of 2020, and the winter of 2020/2021.
Overall, the results showed that the psychosocial variables predicted significant variance at all 3 time points and that the overall percentage of variance predicted increased over time. The nature of such prediction also changed over time. Early in the pandemic, fear and perceived severity showed the strongest associations with mask-wearing behavior, along with perceived susceptibility and attitudes. Three months later, attitudes emerged as the strongest and only independent predictor of mask-wearing behavior. An additional 3 months later, the prediction of mask-wearing shifted again such that self-efficacy emerged as the strongest and only independent predictor of mask-wearing behavior.
This pattern of shifting prediction suggests that the factors most responsible for mask-wearing behavior changed over time and with familiarity with prevention behaviors in the pandemic, which supports our hypothesis. Early on, when the threat was immediate, strong emotional responses prevailed and may have dominated behavioral reactions. Three months later, the emotional responses may have crystallized into the formation of a coherent attitude toward the virus and mask-wearing behavior. Finally, another 3 months later, it is perceptions of behavioral efficacy that prevailed. This later shift suggests that emotional reactions may have cooled over time and/or people had become accustomed to a routine of mask-wearing. These results suggest that public health practitioners might employ fear appeals early in a public health crisis and transition later to self-efficacy-based messaging as the crisis progresses.
The results have some parallels with transactional stress theory as outlined by Lazarus and Folkman.26,27 According to transactional stress theory, coping with stress is a process that changes over time and with the nature of the stressor and the demands of the situation. Folkman and Lazarus’s 28 classic demonstration of this showed how coping behaviors changed depending on the stage (anticipation, waiting, and resolution) of the stressful encounter, specifically midterm exams. Problem-focused coping was prominent during the anticipation stage, whereas distancing was elevated during the latter stages. Coping, whether it be with final exams or a worldwide pandemic, is a process that unfolds and changes over time and with increased familiarity.
Strengths and Limitations
The present study had notable strengths and limitations. One strength of this study was that it capitalized on an emerging situation, one that was unfamiliar to most at the start. As such, it served as a natural experiment and showed the interplay of emotional and regulatory beliefs in the prediction of a sole behavior and how that prediction changes over time and with familiarity. The changing prediction of mask-wearing over time reinforces a cautionary tale for cross-sectional studies of health behaviors, specifically that they really are snapshots in time and may not reflect changing conditions or cognitions. The fact that self-efficacy is often the strongest or most consistent predictor of many behaviors suggests that we may be quite familiar with those behaviors.
The study shares the limitations of other studies that rely on self-report methods. Specifically, such reports may have questionable reliability and validity. Also, participants may be dishonest or inaccurate in their reporting of assessed behaviors. The study also relied on a convenience sample of university-associated individuals willing to volunteer for a larger behavioral monitoring study that was quite labor intensive. As such, the results may not generalize particularly well to other populations and locations—a more diverse sample may have allowed us to better identify traits that drive attitudes and behaviors associated with wearing masks across nations.
Summary and Conclusion
This longitudinal study has advanced our understanding of preventive health behaviors. Specifically, the study has demonstrated how individuals adopt preventive behaviors in pandemic situations and how predictors of such adaptation (ie, decision-making) change over time. The primary implication of this study is that cross-sectional studies of health behaviors are snapshots in time and may not reflect changing conditions or cognitions. Additional longitudinal approaches to studying associations among psychosocial variables and behaviors will even further enhance our knowledge of how people adapt to new health threats and challenges.
Footnotes
Author Note
The data collection procedures for this study were reviewed and approved by the New Mexico State University Institutional Review Board prior to any data collection. The protocol was classified as Expedited Review, Category 7.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The data collection and preliminary analysis were sponsored by the Office of the Vice President for Research.