
Abstract
The COVID-19 pandemic contributed to an increase in mental health issues; Psychological changes occur in health professionals who are more susceptible to infection. The purpose of this study was to investigate health professionals’ levels of anxiety, rage, and depression in COVID-related special circumstances. A general hospital in Korea experienced a widespread COVID-19 outbreak. There was a total of 149 involved frontline and non-frontline health professionals surveyed. The State-Trait Anger Expression Inventory, General Anxiety Disorder-7, and Korean Screening Tool for Depressive Disorders were utilized in the evaluation of their rage, anxiety, and depression. Anxiety and depression were found to be significantly higher among health professionals by occupation than among non-health professionals. Frontline workers were more depressed than non-frontline workers, according to type of work. These psychological changes can cause PTSD, so it is necessary to check and care for the mental health of health care workers working in medical institutions in the event of mass infections. These issues have been confirmed through studies related to the occurrence of mass infections such as SARS and MERS that the occurrence of mass infections can cause PTSD. The findings proved that the COVID-19 pandemic had a psychological impact on healthcare workers. During the COVID-19 pandemic, it is critical to raise awareness of post-traumatic stress disorder among healthcare professionals.
PTSD has a negative effect on social life.
We find that staff in hospitals, regardless of medical and non-medical staff, all had the stress of mass infection like a pandemic.
Since many studies are focusing on PTSD of medical staff, it is of great significance for extending PTSD care research to non-medical staff.
In the event of a pandemic, it is the basis for preparing measures for mental health care of medical institution workers.
Introduction
The respiratory infection known as the coronavirus disease 2019 (COVID-19), which is brought on by a novel coronavirus (SARS-CoV-2), was first observed in Wuhan, Hubei, China, in December 2019 and has since spread to other parts of the world. There was a total of 27.4869 million confirmed cases and 894 900 deaths worldwide as of September 9, 2020. 1
Numerous changes have been brought about by COVID-19, including social isolation as one of the preventive measures in addition to changes in personal and social life and medical care.
From November 1, 2002, to July 31, 2003, 2 an outbreak of severe acute respiratory syndrome (SARS) affected 8096 patients and killed 774 people worldwide. 2346 of these deaths occurred in Taiwan, with 105 of them being health professionals. Because of stay-at-home policies and school and store closures, the pandemic had a significant impact on people’s daily lives. As a result, it caused mental health issues such as infection anxiety and depression.
Although COVID-19 has a low mortality rate, due to the high infection rate, several anti-COVID-19 measures have been implemented, including foreign travel bans, shortened restaurant operating hours, prohibition of social gatherings of 5 or more people, mandatory use of face masks, social distancing, and 2-week mandatory quarantine for people with confirmed infection. Changes in daily life as a result of these prevention measures may have an impact on mental health. 3 Furthermore, physical and mental suffering from sequelae persists even after recovering from COVID-19, and the pandemic’s persistence may result in serious health problems. 4
Post-traumatic stress disorder (PTSD) can also occur as a result of large-scale infectious diseases; it is a mental or psychological disorder that manifests after direct or indirect exposure to a shocking traumatic event. 5 A 2005 study of 1394 SARS survivors in Hong Kong found that 47.8% of them developed PTSD at some point after contracting SARS. Some of these survivors still had PTSD 30 months after contracting SARS. 6 Furthermore, according to a study on long-term mental disorders in SARS survivors, the majority of survivors were diagnosed with PTSD after contracting SARS, and many of them also developed other mental disorders, such as panic disorder. These findings indicate that the mental health issues caused by PTSD following the SARS infection persisted over a long duration. 7
COVID-19 diagnosis, which either confirms the disease or casts suspicion and social stigma on individuals. 8 Kim and Park 9 reported in a study on PTSD, specifically on symptoms such as avoidance and disruption of sleep among health professionals after an outbreak, that professionals such as doctors, nurses, lab specialists handling virus cases, who work most closely with the infection, suffer from more severe forms of PTSD. Similarly, studies look into the relationship between PTSD and job-related variables. A study has been conducted on the effects of occupational hazards on social workers, 10 and another study has been conducted on the physical and mental health, as well as the quality of life, of firefighters. 11
Vaccines were not available at the start of the pandemic in Korea, and no effective treatment for the globally spreading COVID-19 was discovered. Healthcare workers are inextricably linked to the infection because their jobs entail diagnosing suspected cases and treating confirmed patients. Health professionals are vulnerable to PTSD, including anxiety symptoms, because their infection risk is also high due to the nature of the virus.
In other words, COVID-19 has caused short and long-term health issues for healthcare workers, such as mental stress, anxiety, mental disorder like PTSD 12
The COVID-19 pandemic has had a significant impact on the mental health of the majority of health professionals who have directly encountered SARS survivors and have suffered from stress. 13 According to one study, the prevalence of insomnia among health professionals was significantly higher than in the general population. 14 A previous study found that the prevalence of both depression and PTSD symptoms was higher among health professionals than among the general public in hospitals that treated Middle East respiratory syndrome (MERS) patients. 15 Nonetheless, previous COVID-19 studies primarily focused on mental and job stress in health professionals, with some of them investigating the impact of special COVID-19 circumstances, such as a hospital-wide outbreak and PTSD among health professionals.
In February 2021, there was a mass outbreak of COVID-19 inpatient wards from the seventh to the ninth floors of the main building of a general hospital in Seoul, 16 and meticulous frontline tracing was performed on health professionals, patients, family caregivers, and paid caregivers for more than a month to screen close frontline individuals and confirmed patients. A total of 218 patients were diagnosed with the infection.
Thus, the present study aimed to investigate the effects of this incident on the healthcare and non-healthcare staff. In particular, the healthcare staff was divided into frontline health professionals and non-frontline health professionals to compare their levels of anxiety, anger, and depression. We hypothesized that frontline staff would display a higher level of anxiety, depression, and anger than non-frontline staff.
Methods
Participant Selection
The research site is a government-designated safety hospital where COVID-19 patients are transported and treated. Staff from this hospital were divided into 4 groups for the study: frontline healthcare staff, frontline non-healthcare staff, non-frontline healthcare staff, and non-frontline non-healthcare staff. We conducted a questionnaire-based survey to assess their psychological changes during the COVID-19 period.
A total of 149 people were enrolled, including 85 frontline healthcare workers, 39 frontline non-healthcare workers, 13 non-frontline healthcare workers, and 12 non-frontline non-health care workers.
Frontline healthcare personnel include a COVID-19 face-to-face treatment doctor and a COVID-19 patient face-to-face nurse.
Frontline non-healthcare personnel include staff in charge of COVID-19 patients and a foreign interpreter.
Non-frontline healthcare personnel: Personnel in the diagnostic laboratory medicine department who do not have direct patient contact but are medical personnel. Non-frontline non-healthcare personnel include the PR team, the general affairs team, and so on.
The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. The study was approved by the Soonchunhyang University Hospital Institutional Review Board [No. 2020-05-015]. For all studies related to human subjects, freely given written informed consent was obtained from participants.
Survey Method
Following the selection of participants, questionnaires with survey objectives and instructions were delivered directly to each group. The survey received a 100% response rate. The questionnaire was filled out between March 22 and March 29, 2021.
Survey Contents
The survey measured participants’ levels of frustration, anger, and anxiety, as well as changes in concentration and sensitivity prior to COVID-19. Furthermore, we asked those who had been quarantined or treated for COVID-19 about major symptoms, whether they had talked to their family or friends via video calls or text messages during quarantine or treatment, and whether they had played online games, exercised, or engaged in other activities.
In addition, data on general characteristics, such as cohabiting with family members during the COVID-19 period (minor child or elderly members ≥65 years), psychiatric counseling and treatment history, chronic disease, and loss of income due to COVID-19 were also collected to analyze whether these factors had an impact.
Instruments
State-trait anger expression inventory (STAXI)
We used the Korean version of the STAXI (STAXI-K). As for the anger measurement tool, state anger (10 Questions) from the State-Trait Anger Expression Inventory (STAXI) developed by Spielberger and it was converted into a Korean version (STAXI-K).17,18 It contained 10 items asking about participants’ mood, such as feelings associated with COVID-19, and each item was rated on a 4-point scale consisting of 1 “never,” 2 “sometimes,” 3 “frequently,” and 4 “always.” The total score ranged from 0 to 40, with the range close to 40 meaning higher levels of anger and the range close to 0 meaning lower levels. The cutoff line set for anger was over to 14 in this study.
Generalized anxiety disorder 7-item scale (GAD-7)
The GAD-7 was used to measure anxiety symptoms and severity. 19 The scale comprised 7 items inquiring about participants’ experiences related to becoming agitated, easily frustrated, or afraid due to COVID-19, and each item was rated on a 4-point scale consisting of 1 “never,” 2 “a few days,” 3 “more than half of the time,” and 4 “almost every day.” The total score ranged from 0 to 28, with a higher score indicating greater anxiety due to COVID-19. The cutoff for anxiety was set at 10 in this study.
Korean screening tool for depressive disorders (K-DEP)
The K-DEP was used to measure depression. For evaluating, the K-DEP provided by the National Mental Health Center Mental Health R&D Project Team of the Ministry of Health and Welfare and the KU Mind Health Research Center at Korea University was used. 20 This scale comprises 12 items about the severity of depression-related symptoms, such as depressed mood, reduced concentration, and attachment to life. Each item is rated on a 5-point scale consisting of 1 “not at all true,” 2 “slightly true,” 3 “moderately true,” 4 “considerably true,” and 5 “extremely true.” The total score ranged from 0 to 60, with a higher score indicating greater depression due to COVID-19. The cutoff for depression was set at 15 20 in this study.
Data processing and statistical analysis
Participants’ characteristics were derived as frequencies and percentages. The differences between quarantined and non-quarantined staff were analyzed using the chi-squared test, and the differences in anger, depression, and anxiety among job groups were analyzed using analysis of variance (ANOVA) followed by Bonferroni post-hoc analysis. All statistical analyses were performed using R version 4.0.5, and statistical significance was set at <.05 for a 2-tailed test.
Results
The study population comprised 52 individuals aged 20 to 29 years (34.9%), 56 individuals aged 30 to 39 years (37.6%), 26 individuals aged 40 to 49 years (17.5%), and 15 individuals aged 50 to 59 years (10.1%). Twenty-three patients were men (15.4%), and 126 were women (94.6%) (Table 1).
Demographic and General Characteristics of the Study Population (n = 149).

Values are presented as number (%) Chronic disease divided multiple selection.
There were no differences in anger among the 4 groups of staff (P = .11), but levels of anxiety (P = .01) and depression (P < .05) differed among them. There were no statistically significant differences in anger, anxiety, and depression between the quarantined and non-quarantined groups (P = .7) in Table 2.
ANOVA Results of Participants’ Responses to the Anger, Depression, and Anxiety Surveys by Quarantine Type.

Note. Values are mean ± standard deviation, unless otherwise stated.
STAXI = state-trait anger expression inventory; GAD-7 = 7-item generalized anxiety disorder scale; K-DEP = Korean screening tool for depressive disorder.
To analyze the differences by job group and type of work, we compared frontline and non-frontline staff and healthcare and non-healthcare staff (Table 3, Figure 1).
ANOVA Results of Participants’ Responses to the Anger, Depression, and Anxiety Surveys by Job Type.

Note. Values are mean ± standard deviation, unless otherwise stated.
STAXI = state-trait anger expression inventory; GAD-7 = 7-item generalized anxiety disorder scale; K-DEP = Korean screening Tool for anxiety disorders.
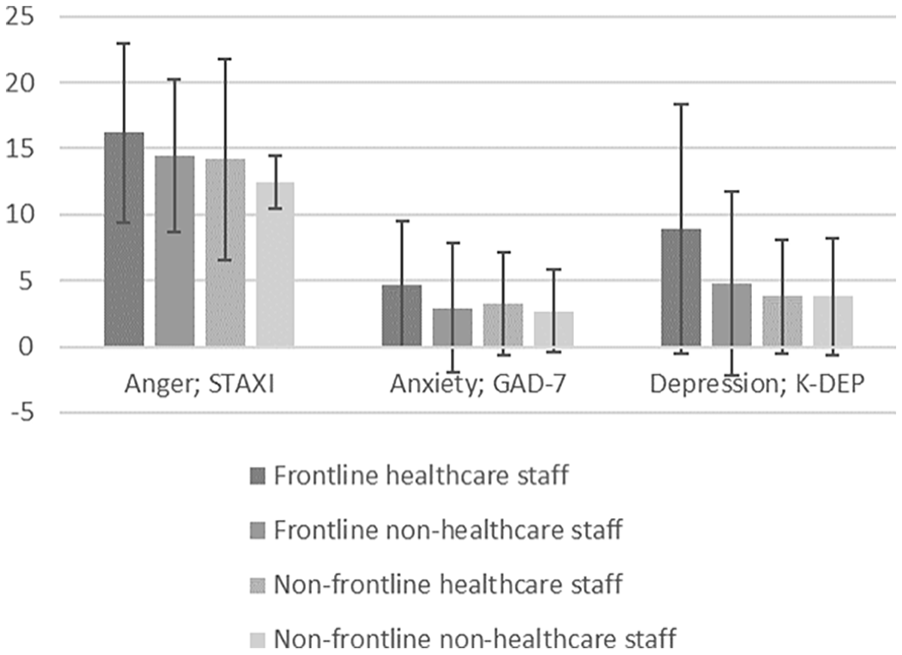
Results of participants’ responses to the anger, depression, and anxiety surveys by position.
Compared by dividing into just healthcare and non-healthcare staff, except for anger (P = .06), anxiety (P = .037) and depression (P = .005) were statistically significantly higher in medical staff than non-medical staff.
In order to compare only the medical personnel, the medical personnel were divided into frontline and non-frontline healthcare staff, and as a result, the level of depression was statistically significantly higher in the face-to-face healthcare staff (P = .006). There were no statistically significant differences in anger, anxiety, and depression between non-frontline healthcare staff (clinical pathologist, etc.) and non-frontline non-healthcare (PR team, general affairs team, etc.) staff who did not have direct contact with patients (P > .05).
However, healthcare staff showed statistically significant higher anxiety (P = .037) and depression (P = .005) than non-healthcare staff. In terms of the type of work, there were no statistically significant differences in anger and anxiety between frontline (healthcare/non-healthcare) and non-frontline (healthcare/non-healthcare) staff (P > .05), but depression (P = .002) was statistically significantly higher among frontline staff who had direct contact with patients in Table 3.
Based on a cutoff of 14 or higher for anger (STAXI-K), 18 (48.6%) in the quarantined group and 48 (42.9%) in the non-quarantined group experienced anger. Based on a cutoff of 10 or higher for anxiety (GAD-7), 3 (8.1%) in the quarantined group and 14 (12.5%) in the non-quarantined group experienced anxiety. Based on a cutoff of 14 for depression (K-DEP), 5 (13.5%) in the quarantined group and 21 (18.8%) in the non-quarantined group experienced depression in Supplement Table.
Discussion
Main Finding of This Study
This study looked at differences in the levels of anger, depression, and anxiety among healthcare professionals working in various capacities during a COVID-19 mass outbreak in a general hospital. The findings revealed that anger did not differ significantly by job group or type of work. Anxiety levels were higher among healthcare workers than among non-healthcare workers. Furthermore, depression was more prevalent among frontline healthcare workers than among non-frontline healthcare workers.
What is Already Known on This Topic
A study of nursing staff who provided direct care with MERS (Middle East respiratory syndrome) patients reported 22.2% of PTSD and 27.8% of partial PTSD. 21 A study on the mental health of COVID-19 healthcare providers reported that approximately 29% of the participants displayed extreme tension, depression, and anxiety, while 2.2% to 14.5% of them developed stress-related mental health problems. 22
Psychological changes among healthcare personnel in a hospital following a mass outbreak should be discussed from a variety of angles. First, because the presence of an index patient within the facility and the subsequent spread of the infection is uncontrollable, with difficulties in halting the spread of the infection even if response measures are implemented immediately after its onset, healthcare personnel may develop a sense of helplessness. Second, while healthcare workers are fully committed to promoting public health by working to treat and prevent the spread of infectious disease, they may experience depression and diminished confidence as a result of the stigma associated with potential COVID-19 exposure. Furthermore, their concerns and fears of contracting the infection and spreading it to their family or those around them must be considered.
What This Study Adds
The study’s findings have significant social implications, indicating that society must pay attention to the possibility of PTSD among healthcare workers during an epidemic or pandemic, such as COVID-19, and that a viable management system to address the condition must be developed. First, psychological changes in medical workers following COVID-19 will be publicized in order to promote a system for early detection, treatment, and management of mental health problems among health care providers.
To eliminate barriers to advancement at work due to prejudice, such as social stigma against mentally ill people or prejudice against family and relatives, PTSD caused by psychological change must be recognized as a social problem, requiring various institutional and policy changes and support.
Second, the government should spearhead efforts and collaborate with healthcare organizations to create a self-evaluation app as well as a care and management system for COVID-19 healthcare staff suffering from PTSD. This would allow for active monitoring, early detection, and treatment of COVID-19-induced PTSD in healthcare workers.
Third, self-evaluation should be further promoted to develop big data according to job group and the type of work and to acquire data of specific cases, based on which professional opinions and treatment modalities should be developed in collaboration with diverse specialists and healthcare providers. These data should be utilized to continually upgrade the system.
The enhancement of public knowledge is also crucial in this regard, in addition to political backing. In order to encourage consideration of disease prevention measures, educational campaigns and awareness activities are crucial. Social support may help to some extent in relieving their despair, anxiety, and rage since it has been shown in research that it is related to stress brought on by social norms as well as depression, anxiety, and tension. 23 Social media, particularly in contactless situations such as COVID-19, has made a significant contribution to assisting the general public in understanding the origin, transmission, and control of disease. 24 Just as specific awareness and education campaigns have informed people about the seriousness of the disease and how to avoid contact with it, health care workers should be informed about the possibility of PTSD and should be protected and respected. One of the study’s limitations is that we were unable to include diverse professionals and types of work, such as medical faculty and nurses who worked in the COVID-19 screening center, due to a variety of factors, such as infection control regulations in hospitals. Subsequent research should aim to create a viable PTSD measurement and management system that is tailored to the job characteristics of healthcare workers in various specialties, such as surgery and internal medicine.
The levels of anxiety, anger, and depression in healthcare staff exposed to a special COVID-19-related situation, namely a mass outbreak of the infection in a general hospital, were surveyed and statistically analyzed in this study. We did not, however, use a questionnaire to assess psychological recovery, such as the Conner-Davidson Resilience Scale (CD-RISC). Furthermore, due to the cross-sectional nature of our study, we were unable to establish a causal relationship between the mass outbreak and the anxiety, anger, and depression of healthcare workers. As a result, we intend to conduct a follow-up survey on the same group.
During epidemics and pandemics such as SARS, MERS, and COVID-19, healthcare providers, particularly frontline healthcare providers who are at an increased risk of PTSD due to the nature of their professional role, should be actively monitored. Furthermore, proactive measures such as providing periodic psychological counseling, rest areas, periodic job training for those at high infection risk, implementing shortened work hours, and establishing a special support team, as needed, may be effective.
Despite these limitations, the results of this study are useful as baseline data for research on the psychological changes that healthcare workers could experience in special situations, such as a mass outbreak of COVID-19 in a single facility.
Policy Recommendations
It is already known that mass infection events like COVID-19 and SARS cause PTSD in healthcare workers. Not only do medical staff who have direct contact with patients face high job demands, but health workers working in hospitals face high job demands simply by responding to infectious diseases, such as fear of coming into contact with positive patients and the possibility of contagion, which can lead to PTSD. It is only natural to safeguard them through policy. Governments, as previously stated, should collaborate with health care providers to manage PTSD in COVID-19 health care providers. The long COVID-19 dispatch period, the stress of forced job demands, the stress caused by unclear COVID-19 national guidelines and policies, and the work environment all contribute to PTSD caused by mass infection. As a result, if a mass infection like COVID-19 occurs, financial or psychological compensation corresponding to job demands should be guaranteed, and adequate rest and a moderate workload should be protected to prevent PTSD. Nationally, it is necessary not only to investigate and report confirmed cases on a regular basis, but also to continuously monitor the mental health of hospital workers and to implement a mental health management program by deploying mental health experts from the beginning of group infection.
Supplemental Material
sj-docx-1-inq-10.1177_00469580231161435 – Supplemental material for A Cross-Sectional Study on the Psychological Changes of Medical Personnel in Hospitals Who Experienced Special COVID-19 Situations
Supplemental material, sj-docx-1-inq-10.1177_00469580231161435 for A Cross-Sectional Study on the Psychological Changes of Medical Personnel in Hospitals Who Experienced Special COVID-19 Situations by Xiao Guang Yan, Hwa Yeon Sun and Byung Wook Yoo in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We appreciate to the all the hospital staffs at Soonchunhyang university Seoul hospital and their carers for their time and contribution to this study. Also appreciate the helpful comments of the editor and reviewers.
Author Contributions
The authors contributed to the manuscript equally.
Data Availability
The datasets generated and/or analyzed during the present study are available from the corresponding author upon reasonable request until May 2024.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.