
Abstract
The shortage of healthcare workers is a growing problem across the globe. Nurses and physicians, in particular, are vulnerable as a result of the COVID-19 pandemic. Understanding why they might leave is imperative for improving retention. This systematic review explores both the prevalence of nurses and physicians who are intent on leaving their position at hospitals in European countries and the main determinants influencing job retention among nurses and physicians of their respective position in a hospital setting in both European and non-European countries. A comprehensive search was fulfilled within 3 electronic databases on June 3rd 2021. In total 345 articles met the inclusion criteria. The determinants were categorized into 6 themes: personal characteristics, job demands, employment services, working conditions, work relationships, and organizational culture. The main determinants for job retention were job satisfaction, career development and work-life balance. European and non-European countries showed similarities and differences in determinants influencing retention. Identifying these factors supports the development of multifactorial interventions, which can aid the formulation of medical strategies and help to maximize retention.
Keywords
The shortage of nurses and physicians is a growing and worrying problem across the globe due to the aging population, increasing incidence of chronic diseases and aging healthcare workforce.
This systematic review investigated push and pull factors that determine why nurses and physicians want to stay or leave their position; the main determinants were job satisfaction, career development and work-life balance.
Identifying these factors supports development of multifactorial interventions, which can aid the formulation of human resource strategies and help to maximize retention of nurses and physicians.
Introduction
Healthcare personnel shortages are a problem across the globe. With a lack of 4.3 million doctors in 20161 and 5.9 million nurses in 20202 globally, the shortage was already critical. The World Health Organization (WHO) reports that by 2030, there will be a global shortage of almost 14 million healthcare workers, in terms of nurses, physicians, midwives and other cadres. 3 These challenges constitute a multifaceted phenomenon. Among other things, extant literature shows that personnel shortages in healthcare are primarily driven by demographic changes in the population, increasing demand for healthcare, and a growing number of chronically ill patients. 4 Life expectancy has consistently increased and is expected to continue to increase, which, in turn, increases morbidity because people are experiencing more age-related diseases. 5 At the same time, the workforce is aging. 4 The expected retirement rate of nurses within the next 10 years is 17% in the American and European regions. 2 Regarding physicians, half of them who were practicing in 2021 will be retired by 2030 due to age and early retirement.6,7 The cumulative effect of these trends is that there are insufficient recruits to replace retiring personnel. 8
These high turnover rates are dysfunctional in multiple respects. Firstly, they lead to financial losses related to recruitment. Secondly, high turnover rates have a deleterious impact on the quality of care provided, for example, higher mortality rates9-11 and an increase in medical errors.10,12 loss of care continuity13,14 and patient dissatisfaction, 15 which, in turn, can result in lost revenues and higher patient care costs. Finally, high turnover rates reduce staff productivity for the simple reason that there is less staff to complete the tasks 16 which can be lowering the morale of the remaining staff.17,18 This may lead to additional turnover among the remaining nurses and physicians. 19
EU hospitals, in particular, are suffering from high staff turnover rates, while simultaneously being faced with austerity measures. 4 This has resulted in less recruitment, replacement and retention investment to meet their saving targets. 20 During the COVID-19 crisis, hospitals were under additional pressure due to acute stress, frustration, isolation and the high risk of infection. Many studies show an increasing desire among medical staff to quit their jobs and leave the healthcare sector. In the long term, we can expect additional dropouts as a result of long-term mental health problems among medical staff due to COVID-19. 21 Nashwan et al reported that turnover intentions of nurses were higher during COVID-19 in comparison before the crisis. 22 Overall, the healthcare workforce is vulnerable to the growing job demands in the sector witnessed both during and after the COVID-19 pandemic. 23
Literature shows that turnover intentions are critical predictors when it comes to nurses and physicians leaving the workforce.13,24 The intention to leave is considered to be one of several stages in a complex decision-making process that leads to turnover behavior. 25 The reasons that trigger nurses’ and physicians’ intention to leave are complex and influenced by multiple individual and organizational factors. A recent systematic review of the determinants influencing turnover among nursing staff indicates that job satisfaction, stress and burnout are crucial individual determinants among this working population. 26 Although the determinants influencing medical doctors’ intention to leave have been less systematically studied, the available evidence indicates that psychosocial determinants (eg. job satisfaction, burnout) substantially influence these particular nurses’ and physicians’ intention to leave.26,27 This conclusion is supported by the Job Demands-Resources (JD-R) model. 28 The JD-R model was developed in the context of employee wellbeing and work-related stress. The central idea is that every occupation has its specific job demands and job resources. Job demands comprise all aspects of the job that require continuous physical or mental effort and are associated with a specific cost. On the other hand, job resources stimulate personal growth, lead to the achievement of one’s goals and reduce the costs of job demands. 29 Job satisfaction, burnout and turnover intentions are thus the results of complex interactions between job demands and job resources. The associations between job demands, job resources, job satisfaction, burnout and turnover are illustrated in Figure 1, based on the findings of extant literature. 29
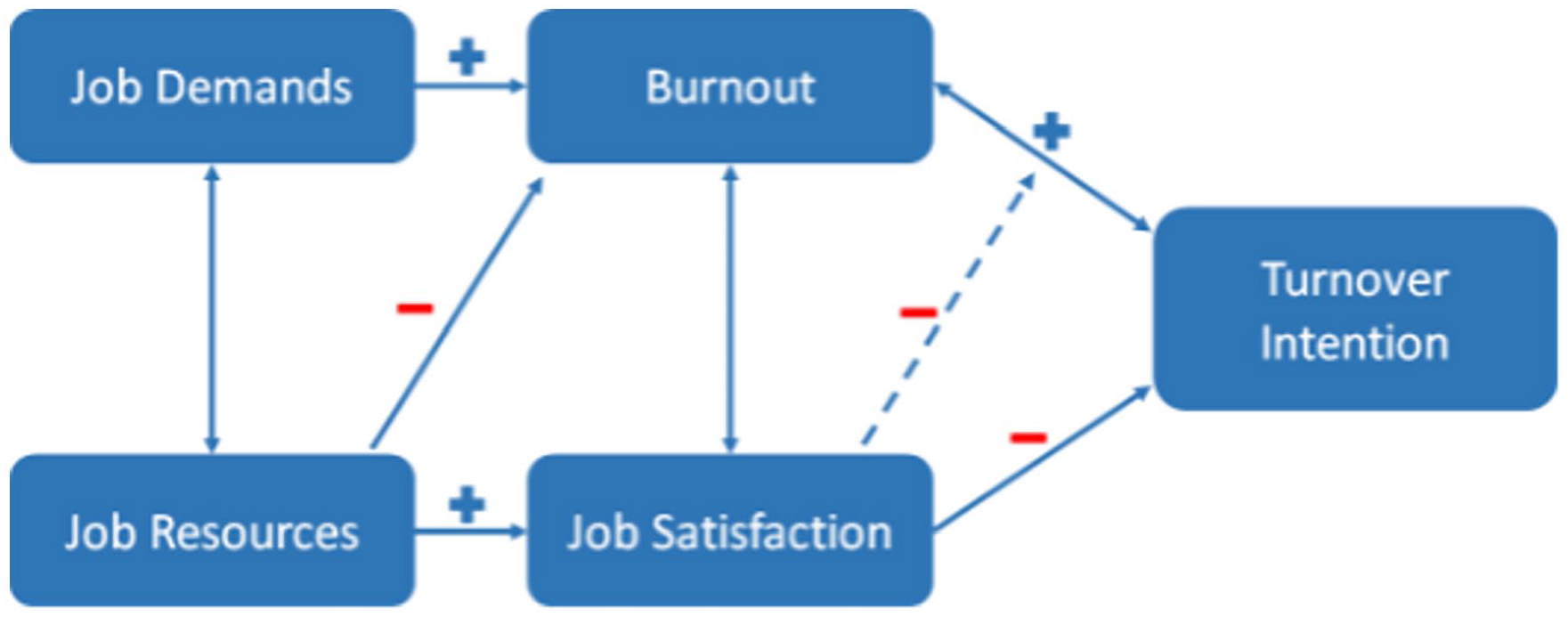
Job Demands-Resources Model adapted to turnover intentions. 29
Hence, focusing on workers’ intention to leave is strongly recommended, whereas, attitudes, subjective norms and perceived behavioral control are what underpin someone’s intentions and actual behaviors. 30 Both policymakers and managers can potentially still influence these intentions in order to prevent workers from actually leaving the workforce. 31 Although a lot of research has been conducted on this topic, multiple research gaps remain. Prior systematic reviews either solely focused on nurses24,32 or physicians, 33 or carried out in a non-EU setting34,35 or primary care setting. 36 In addition, they were conducted prior to the COVID-19 pandemic. As both demographic changes and the COVID-19 pandemic may result in new outcomes, this systematic review is desirable.
To the best of the author’s knowledge, no systematic review is conducted yet examining the nurses’ and physicians’ intentions to leave their position in the hospital. The first aim of this systematic review is to explore the prevalence of nurses and physicians who intend to leave their position in a hospital in EU countries. Second, this systematic review aimed to explore the main determinants influencing job retention among nurses and physicians in their respective position in a hospital setting. The outcomes of this study will enhance our current knowledge of the prevalence and the determinants influencing job retention as well as diversity in magnitude of determinants and potential new determinants. Knowing these determinants of intention to leave, will aid the development of retention interventions in a hospital setting and inform policymakers related to human resources. These interventions may prevent nurses and physicians from actually leaving the workforce, which, among other things, positively impacts the quality of care, financial costs and morale of the remaining staff.
Methods
This systematic review constitutes the starting point of a large European Union-funded project called MenTal hEalth: focus on Retention of healthcare workers (METEOR). Further information about the project can be found on the website. 37
Design and Population
The systematic review was conducted with multiple quantitative and qualitative studies, and was carried out in accordance with the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement. 38
The systematic review is registered at the International prospective register of systematic reviews (PROSPERO), CRD4202159007. The population studied in this review included nurses and physicians, namely nurses and physicians, who either worked or are currently working in a hospital setting.
Data Sources and Searches
We developed an extensive search string to be used in scientific literature databases, namely PubMed, Embase, and CINAHL. The study search was fulfilled on June 3, 2021. The search was framed using the domain (healthcare professionals), determinant (determinants/interventions), and outcome (job retention/turnover) within the last 10 years. The timeframe of the last 10 years was chosen because the healthcare sector is changing a lot in recent years and, this systematic review aimed to include recent articles so outcomes are still sufficiently relevant for today’s healthcare sector. In this study, we used the term turnover to refer to nurses and physicians who no longer work as nurses and physicians in their respective position in a hospital setting, which included former nurses and physicians who either moved to a different unit, different hospital, moved on to work in non-patient roles or left the system entirely. 39
For healthcare professionals, the following synonyms were used: “health personnel [Mesh],” “health personnel,” “healthcare workers,” “healthcare providers,” “healthcare professionals,” “health workforce,” and “health workers.” Because of the population, the domain was extended with “nurses [Mesh],” “nurse,” “nursing personnel,” “physicians [Mesh],” “physician” or “doctor.” The search for determinants contained “determinants,” “factors,” “predictors” and “interventions.” Synonyms for the outcome that were used were: “personnel turnover [Mesh],” “personnel turnover,” “retaining personnel,” “job retention,” “retention rates,” “turnover intention,” “intention to leave,” “intention to quit,” “intention to stay.” Supplemental Appendix 1 can be consulted for the complete search string.
Study Selection
Articles were included in the review if they studied nurses and/or physicians, and contained determinants of job retention or turnover intention. Furthermore, the study needed to have been published between 2011 and August 2021. If a study was not carried out in a hospital setting or if the manuscript was not in English, then the study was excluded. Further exclusion criteria were as follows: systematic review, study protocol and thesis, and full text not available. Moreover, studies that contained interventions seeking to reduce the intention to leave were also excluded from this systematic review. All the participants in the studies also needed to be of working age. There were no restrictions on gender, ethnicity or healthcare status. Data extraction began with evaluating the abstracts of the studies following the formulated inclusion criteria; one reviewer conducted this evaluation. Furthermore, a selection was made of those studies that were conducted in countries of the European continent (EU) or non-European continent (non-EU). This distinction was drawn because of the participating countries in the METEOR project, which led us to focus on EU studies. 37 After the first screening, full texts of EU studies carried out over the last 5-year period were examined by 2 pairs of 2 reviewers (JB, SS, NdV, PdW). The studies carried out during this period give the strongest insight into the determinants in the EU. Furthermore, we did this to create an overview of the information about the pre-COVID period in the EU with a minimal degree of bias.
In order to facilitate the comparison of EU outcomes with non-EU studies, the abstracts of studies conducted in non-EU countries over the last 10-year period, rather than the last 5 years, were analyzed. This global overview of non-EU outcomes can be used to supplement details in the EU outcomes.
A quality assessment of the EU studies in our search was conducted by using the Mixed Methods Appraisal Tool (MMAT) version 2018. This tool was selected because it is applicable for mixed methods studies. To reduce bias, 2 researchers independently carried out the quality assessment (NdV, PdW). Non-EU studies were not included in this quality assessment as the outcomes of the heterogeneous non-EU countries were indicated as a global overview and supplemental in the EU outcomes.
Any disagreements over the eligibility of certain studies were resolved through either engaging in consensus-based decision-making or by including the views of an additional author. The other authors reviewed the validity of the data extraction.
Data Extraction
The data from the EU studies were extracted into multiple characteristics: the author, the country where the study was conducted, the population and push and pull factors influencing job retention. Push factors were defined as those factors which increase the intention of nurses or physicians to leave the hospital setting. Conversely, pull factors were defined as those factors which increase the intention to stay in the hospital setting. Prevalence of nurses and physicians who intend on leaving their position at hospitals in EU studies where described using percentage.
The determinants identified in the EU and non-EU studies were organized into one of the following subthemes: personal characteristics, job demands, employment services, working conditions, work relationships and organizational culture. The determinants identified in the EU studies where described in text. The data from the non-EU studies were extracted into one of the subthemes a table.
Results
The literature search, including determinants and interventions, resulted in 3521 studies over the last 10-year period. After excluding all studies that met the exclusion criteria and removing any duplicates, 345 studies fulfilled the inclusion criteria: 37 EU studies and 308 non-EU studies (Figure 2).
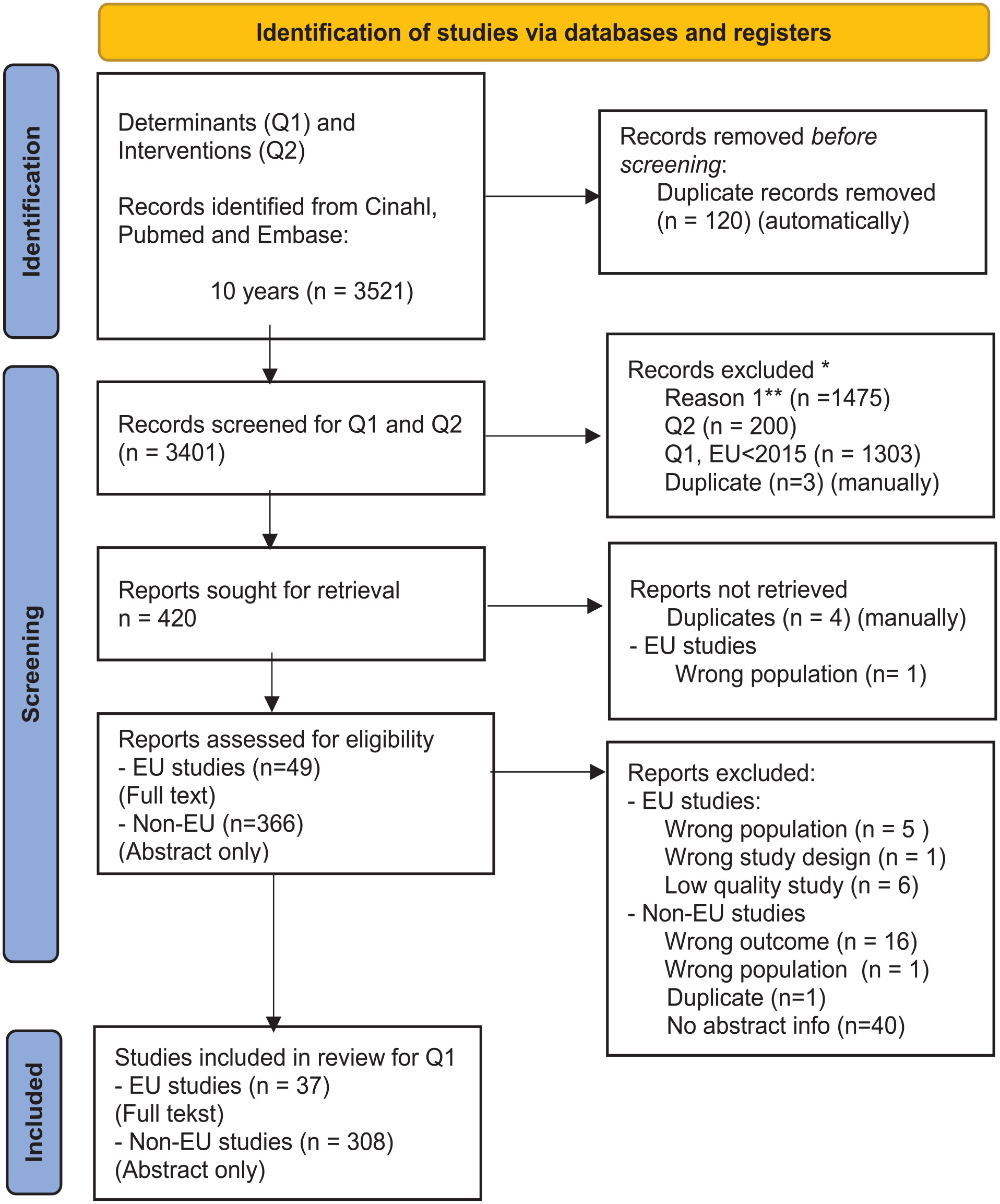
PRISMA flow diagram.
The EU studies comprised 2 qualitative studies and 35 (semi)quantitative studies. Most of the studies were conducted in Turkey (19%), followed by Germany (8%), Norway (8%) and Sweden (8%), respectively (Table 1).
Study Characteristics of the Included EU Studies.

Of the studies included, 78.4% were concerned exclusively with nurses,15,40-67 8.1% only looked at physicians,68-7010.8% included nurses and physicians,71-74 while 2.7% studied healthcare professionals. 75 The studies of healthcare professionals also included nurses and physicians, therefore, these were included.
The literature showed that between 12% and 64% of nurses intend to leave their current job (Figure 3). Turkey in particular has a high number of nurses who intend to leave, with studies finding 60.9% 57 and 64.4%, 42 respectively. The countries with the lowest percentages of nurses intending to leave were Italy (11.7%), 63 Germany (14%), 67 and Switzerland (16.7%). 71
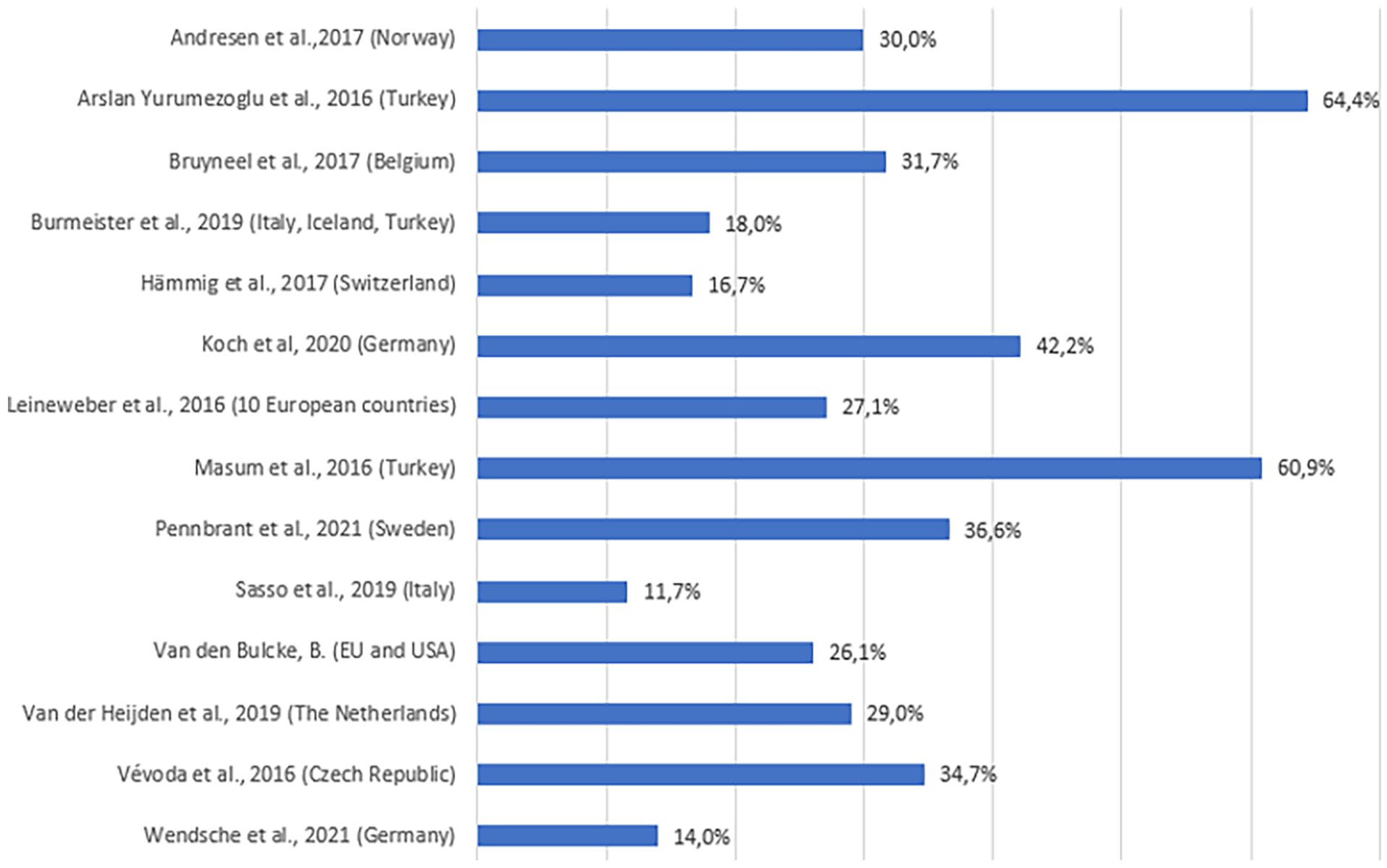
Intention to leave: registered nurses.
With respect to physicians, the percentage of them that intend to leave their current job ranged from 16.7% to 29% (Figure 4). Switzerland had the lowest number of physicians who intend to leave, namely 14.2%, 71 followed by Norway (21%), 70 Poland (22.7%) 68 and Germany (28.2%). 72 Van den Bulcke et al studied multiple countries and revealed that 36.1% of the participating physicians intended to leave their job. 73

Intention to leave: physicians.
Determinants in the EU Studies
The results related to the determinants were categorized into push and pull factors. Table 2 provides an overview of the selected EU studies, along with all the push and pull factors for each study.
Details of Studies With Push and Pull Factors Related to Nurses and Physicians’ Intention to Leave Their Hospital: EU Countries.

Because of the many included EU countries (besides non-EU), this was chosen to be included in the study.
Two reviewers (NdV, PdW) discussed these push and pull factors to categorize them into “personal characteristics,” “job demands,” “employment services,” “working conditions,” “work relations,” and “organizational culture.”
Personal Characteristics
The studies showed that older nurses were more likely to remain in the workplace, 57 while younger nurses were more inclined to leave their hospital.41,44,57,73 The outcome related to the impact of gender was inconsistent. Specifically, the literature revealed male gender was both a pull factor 55 and a push factor. 63 The female gender decreased the intention to stay. 43 Furthermore, one’s household structure (number of children) was also found to impact upon one’s intention to leave. 40
Furthermore, higher educated nurses (Master’s degree) were more likely to leave their current employment. 57 Moreover, a higher Big Mac index in the healthcare worker’s region increased their intention to leave. 73 Good personal health 40 and being single 57 were found to potentially increase retention, moreover, self-efficacy (indicating one’s beliefs about one’s personal ability to implement the necessary actions to achieve specific goals) reduced turnover intention. 15 A lack of passion for patient care 53 and high interpersonal conflict 47 were also found to result in an intention to leave.
Job Demands
Overall, job demands and (adequate) resources were found to play a positive role in the intention to stay.42,48 More specifically, job satisfaction was found to be an important pull factor in multiple studies,15,40,41,43,44,46,49,57,60,63,72 whereas a lack of job satisfaction was found to be a push factor.42,53
Other push factors were burnout symptoms, 65 which can be defined as depersonalization, emotional exhaustion and reduced personal accomplishment. 76 Several studies highlighted symptoms like emotional exhaustion42,43,47,58,63 and depersonalization42,74 as push factors. Similarly, nurses and physicians were found to be more likely to intend to leave when they experienced dissatisfaction, 42 were unsatisfied with individual expectations, 45 had low energy, 47 encountered ethical dilemmas in the workplace, 51 experienced mental job stress 71 or high moral distress. 54
Other studies pointed toward quantitative workload,47,67 high quantitative demands, 67 temporal, physical, emotional and mental workload, 71 rest break disturbances, 67 stressful work 41 and performing non-nursing care activities (for nurses) as push factors. 63 Conversely, performing core nursing activities was found to be a pull factor. 63 Moreover, the work engagement of the staff,15,58 agentic capacity, 15 the meaning that nurses and physicians attached to their work51,65,75 and low job stress 49 were found to be essential. More specifically, high work engagement was found to be a pull factor, while low work engagement was a push factor. 61 Similarly, pull factors were described in terms of having less stressful work and carrying out less monotonous tasks. 41 Finally, the literature showed that autonomy was an essential factor that positively impacted upon nurses’ intention to stay. 41
Employment Services
Financial items like a good salary40,66,68 and positive changes in salary 52 appeared to also positively impact upon the intention to stay. Furthermore, rewards were found to be a pull factor, 75 whereas effort-reward imbalance impacted upon the intention to leave. 71 The absence of social benefits at work, such as, for example, social perks provided by the employer (personal accounts, vitamins, meal tickets, etc.) led nurses to intend to leave their employer. 66
Moreover, development opportunities in nurses’ and physicians’ careers were found to positively impact upon retention in several studies,43,56,75 including opportunities for education, 44 a chance for renewal 52 and positive career experiences. 55 Conversely, it is important to note that a lack of challenge 53 and limited opportunities for career development were found to increase the intention to leave,43,46 along with a lack of perceived competence. 53 In addition, temporary positions were also found to negatively impact upon job retention. 41
The work schedule was also found to impact upon job retention. For example, schedule flexibility was found to positively impact upon retention, 55 whereas irregular working hours 41 and on-call duties 69 can operate as push factors. The effect of the number of contracted working hours was ambiguous in the studies; both part-time 40 and full-time work 55 were found to affect job retention positively.
Finally, both more working years42,43 and high levels of experience44,55,56 were found to increase the chance of retention.
Working Conditions
Several working conditions positively impact upon retention, such as, for example, reducing the administrative burden and improving infrastructure.52,68 Nurses working in hospitals in the countryside were found to have a greater intention to leave than those working in hospitals in large cities. 68 Moreover, patient care impacts upon the intention to stay. Poor patient safety 63 and higher mortality rates contribute to nurses and physicians leaving their hospital. 73 Similarly, both patient satisfaction 15 and perceived high quality of care63,72 were also found to have a positive impact on job retention.
Adequate staffing was found to have a positive impact on retention.42-44 Conversely, inadequate staffing,43,45,63,72 and a high level of job strain (high demands, low control) 69 were found to be push factors.
Finally, moderate work pace 48 and positive unit-level variables were found to positively influence retention, 55 while a low level of job strain (low demand and high control) were identified as being pull factors. 69
Furthermore, social support,48,65 and a good work-life balance were found to play an important role in the intention to stay.56,68 Therefore, work-family conflict47,61 defined as “a form of inter-role conflict in which the general demands of, time devote to, and strain created by the job interfere with performing family-related responsibilities” 77 or family work conflicts,47,65 defined by Netemeyer et al as: “a form of inter-role conflict in which the general demands of, time devoted to, and strain created by the family interfere with performing work-related responsibilities.” 77 Lastly, work-life imbalance71,75 negatively impact the intention to stay.
Work Relationships
Nurses and physicians benefit from social colleagues, 56 good communication on the work floor, 59 affective commitment,46,62 appreciation from their superior 41 and mutual respect. 73 However, nagging colleagues, 41 unfair behavior 75 and many social conflicts on the work floor negatively impact upon leaving an organization. 67
Regarding teamwork, nurses and physicians were found to benefit from open interdisciplinary reflection and not avoiding end of life decisions. 73 Furthermore, a collegial nurse-physician relationship was emphasized in earlier studies.42,63 Conversely, a lack of appreciation for the operational activities 41 and the absence of a feeling of belonging 53 increased the intention to leave.
Organizational Culture
Nurses were found to benefit from positive organizational changes in terms of job retention.56,70 Moreover, with regard to cultivating a workplace culture characterized by respect and reciprocity, humanity is an essential factor to focus on if a healthcare organization is to positively enhance retention. 48 A positive work environment positively affects retention, 59 whereas a negative work environment (lack of professional solidarity, lack of support from management, horizontal violence and inadequacy of preceptorship process) makes nurses leave their organization. 45
The literature also underscored that good leadership, 59 leadership quality,59,75 and leadership styles make a key difference. Productive leadership styles identified in the research were authentic leadership, 60 upbeat leadership 70 and ethical leadership, 58 while, alternatively, paternalistic leadership was found to be a push factor. 64 Moreover, sufficient social support from one’s supervisor43,51,57,62,70 and vertical trust 48 were found to be important determinants of remaining in the workplace. Multiple studies outlined the importance of positive management for successful retention.56,66 Alongside this, exchanges between supervisors and nurses were also shown to impact upon retention positively. 62 Furthermore, decision authority43,58 and nursing leadership 52 were important pull factors in the literature. Conversely, low decision authority 43 and organizational cynicism 64 negatively impact upon the intention to stay and, hence, should be avoided.
Determinants Non-EU Studies
The determinants influencing nurses’ and physicians’ intention to leave outlined in the non-EU studies afford a global overview of similarities and differences between non-EU and EU studies. The determinants identified in the abstracts of the non-EU studies were also categorized into themes by 2 reviewers (NdV, PdW). Table 3 presents an overview of all the determinants identified in the studies in non-EU countries.
Determinants Influencing Nurses and Physicians’ Retention in Hospitals: Non-EU Countries.

The literature of the determinants influencing nurses’ and physicians’ intention to leave in non-EU countries presented some similarities and differences with the studies in EU countries.
One of the similarities was the impact of job satisfaction upon the intention to leave.78-147 A study conducted in Australia by Doleman et al noted that “Job satisfaction was found to have a significant negative inverse relationship with intention to leave.” 97 Similar to the situation in EU countries, education and career development appeared to play an important role in non-EU countries with regard to the retention of nurses and physicians.87,131,135,148-167 A study conducted in the United States found that career development was positively correlated with retention. 135 Moreover, like in the EU studies, work-life balance112,113,115,118,134,143,157,168-181 and organizational commitment78,82,83,87,91,92,100,103,109,116,118,122,123,128,134,140,157,171,172,178,182-203 were also found to be determinants influencing the intention to leave in non-EU studies.
Notable differences highlighted in the non-EU studies pertained to the impact of race/ethnicity204-206 or discrimination183,207-210 upon the intention to leave. For example, Alshareef et al described that in Saudi Arabia, Filipino nurses were more intent to leave their current position due to discrimination. 183 Furthermore, Hispanic204,205 and black 204 nurses and physicians were more inclined to leave compare to white or Asian nurses and physicians, 204 which could be influenced by discrimination. Furthermore, bullying was frequently noted in the non-EU studies.84,120,211-221 Favaro et al found that those who had recently graduated, particularly male graduates, reported significantly higher workplace bullying. 213
Finally, hospitals with a Magnet designation were associated with lower turnover rates in the United States.222,223 The Magnet program “will continually elevate patient care around the work in an environment where nurses, in collaboration with the interprofessional team, flourish by setting the standard for excellence through leadership, scientific discovery and dissemination and implementation of new knowledge”. 224
Multifactorial Determinants
This review has thus far focused on single factor determinants that impact upon the intention to leave or stay. However, these outcomes are multifactorial rather than being based on a single factor. The review began with the JD-R model that was adapted to address turnover intention, which showed the inter-correlation between job demand, job resources, burnout, job satisfaction and intention to leave (Figure 1). Figure 5 provides an overview of the extended JD-R model with more specific inter-correlations from the considered literature on EU countries.15,41,43,49-51,58,59,61,72,74,225

Inter-correlation figure adapted for turnover intention.
As shown in Figure 5, burnout (symptoms) and job satisfaction are correlated with the determinants, which also impact upon the intention to leave by single factor determinants. It should be noted that the direct correlation between the intention to leave and those determinants was dropped in Figure 5, in order to provide a more precise picture. For example, work-family conflict and work engagement impact upon interpersonal conflict, which, in turn, impacts job satisfaction and subsequently the intention to leave. As was the case for simultaneous work-family conflict, work engagement and interpersonal conflict directly impact upon the intention to leave. Furthermore, social support of the supervisor impacts upon job satisfaction. Moreover, social support impacts upon the meaning of work and subsequently burnout (symptoms), which impacts upon the intention to leave. Nevertheless, social support of the supervisor also directly impacts upon the intention to leave.
Discussion
This systematic review aimed to explore both how prevalent the intention to leave is among physicians and nurses in EU countries and the main determinants of job retention among nurses and physicians in their respective position in a hospital setting.
The results showed notable differences with respect to nurses’ and physicians’ intentions to leave their position. The determinants that impact upon job retention varied and were divided into 6 themes: personal characteristics, job demands, employment services, working conditions, work relationships and organizational culture. These outcomes are in line with previous systematic research in different population32,33,226 and setting.34-36
The similar determinants identified in studies in EU and non-EU countries were job satisfaction, education and career development, work-life balance and organizational commitment. Non-EU countries were characterized by different determinants that impact upon the intention, namely ethnicity and discrimination, bullying and whether a hospital had a Magnet designation. Nevertheless, a comparison of these outcomes should be handled with care due to the heterogeneity variation in countries in the non-EU setting and EU setting. Future research is required to fulfill knowledge of these gaps regarding the determinants in non-EU countries.
The JD-R framework (Figure 1) illustrated the association between job demands, job resources, job satisfaction, burnout and turnover. 29 The outcomes of this current systematic review confirmed that these determinants impact upon the intention to leave. Nevertheless, the factors job demands, job resources, job satisfaction and burnout can be further specified by drawing upon the outcomes from this study. Furthermore, the JD-R framework of Demerouti et al illustrated that the determinants were multifactorial. 29 The results of this study confirmed the multifactorial impact of determinants, illustrated in Figure 5.
The percentages of the prevalence of intention to leave displayed wide variance across the studies. The intention to leave in Turkey displayed the highest prevalence of all the EU studies, with 61-64% of the nurses declaring their intention to leave.42,57 This could be explained by how intention to leave was defined in different studies. Prevalence was measured in terms of intention to leave their organization,42,43,66 intention to leave their current position41,44,55,57,61,63,70,73 or intention to leave their profession.65,71,72 Furthermore, there was also variance in the timeline of the prevalence; some studies measured the prevalence in a longitudinal design (eg, within a 12-month period), whereas others applied a cross-sectional design, which may have impacted the prevalence outcomes.
In terms of personal characteristics, the literature is not clear about the effect of gender on job retention. Leineweber et al found that males were more inclined to leave their profession, but not to leave their workplace. 55 Sasso et al also noted that being male influenced the intention to leave their current job, 63 which was confirmed by the systematic review of Chan et al. 227 However, other studies included in the present systematic review showed that females were more likely to leave their current workplace.43,57 This difference is difficult to explain because the outcomes are so varied. It is possible that there are gender differences related to how nurses and physicians perceive their job.
Moreover, self-efficacy seemed to reduce turnover intentions, A systematic review conducted in 2018 showed self-efficacy is positively related to nursing resilience. 228 Both outcomes assume that implementing an intervention enlarging one’s beliefs about one’s personal ability, could positively impact the retention rates. Supervisors should support healthcare workers by identifying their strengths and enlarging their self-efficacy. Recent research showed that job-crafting can positively impact building on strength, self-efficacy and less turnover intention. 229 Self-efficacy is an interesting theme in turnover intention and more research toward the outcomes and impacting this determinant is desirable to reduce turnover.
Furthermore, this review showed more working years42,43, a high level of experience44,55,56 and being older 57 increased the chances of retention. These outcomes related to experience are in accordance with Chan et al’s systematic review, which studied nurses’ intention to leave their employment or profession. 227 However, they noted that the multifactorial impact of age along with the determinant of experience impacted on the intention to leave; that is to say, the younger the nurses and physicians were and the less experience they had, the greater their intention to leave, whereas nurses above the age of 45 who had less experience were found to be more likely to stay, 227 which should be noted in the outcomes of the present systematic review.
Part-time work was a pull factor in terms of job retention for nurses and physicians. 40 Conversely, full-time work was found to be a push factor in terms of leaving the workplace and a pull factor for nurses and physicians intending to remain in the profession. 55 This could be explained by the fact that nurses and physicians who work full-time instead of part-time are more exposed to working conditions that negatively impact upon job satisfaction and result in them leaving the workplace. Similarly, full-time work can create greater difficulties in combining one’s work and private life, due to more working hours, which negatively impacts upon work-life balance, work-family conflicts, job satisfaction and turnover intention.46,56,61,68,71,75
Furthermore, career and learning abilities were found to be important determinants of intention to leave.43,44,56,75 The ability to further develop as a nurse or physician or the chance of renewal may help reduce the turnover of nurses and physicians. For example, the Magnet philosophy focuses additional attention on education and career development across every career stage, which was indeed found to be a pull factor in hospitals in the United States. 222 Annual interviews can be helpful for both evaluating and reviewing future expectations, such as, for example, one’s career development or learning opportunities.
Leadership is a hot topic at the moment. This review has underscored the positive effect of nursing leadership and autonomy on the intention to stay.41,52 An integrative review by Kiwanuka et al noted that nursing leadership influences the productivity and morale of nursing staff, which can have a positive effect on the general mood on the work floor and, in turn, increase the intention to stay. 230
Social support appeared to be an important psychosocial theme in terms of job retention. Indeed, during the COVID pandemic, many front-line nurses and physicians suffered from mental health problems and benefited from social and organizational support. 231 There is mounting evidence indicating that such support can lead to higher job satisfaction and, ultimately, successful job retention.
It is important to note that the current search string employed in this systematic review did not result in articles specifically related to COVID-19, likely because the studies focused on COVID-19 and the dropouts or determinants impacting upon the intention to leave were not published yet at the moment the search string was enrolled. Further systematic research would be advisable to create an evident clarification of the impact of COVID-19 on the intention to leave of nurses and physicians.
Limitations
This systematic review studied extant literature on physicians and nurses which constitutes a key strength of this study. Other systematic reviews on this topic focused on turnover among solely nursing staff or physicians.24,33 To the best of our knowledge, there is no systematic review available exploring both nurses’ and physicians’ intentions to leave the hospital setting, which makes this systematic review unique.
The limitations of this study should also be considered. We conducted a quality assessment and full-text screening of studies carried out in EU countries for this review. However, no quality assessment was conducted for the studies carried out in non-EU countries; rather, only the abstracts were studied for determinants. In light of the simplified screening of non-EU studies, there is the possibility of bias, and, as such, the outcomes should be considered with caution. 232 Nevertheless, the extensive literature search can be seen as a strength of this review. Furthermore, the METEOR project mainly focused on EU outcomes. In this respect, the non-EU determinants were merely supplementary and should be considered as such. Further systematic research is recommended that more closely examines the determinants influencing the intention to leave hospitals in non-EU countries.
The included studies defined intention to leave in various ways; intent to leave their current position,44,46,47,69 intent to leave their organization,15,42,45,46,55,58,66-68 intent to leave their profession,42,46,47,49,53-55,61,64,66,69,71,72 intent to leave the job,40,41,60,69,70,73 intent to leave the workplace,50,57,61 intent to leave (not specified)43,48,49,51,60,62,63,74,75 or intent to stay.52,56 This systematic review aimed to search for determinants impacting the intention to leave their respective position of nurses and physicians in a hospital setting. The multiple definitions of intention to leave in this systematic review are a limitation of this study. Nevertheless, leaving their position in the hospital could also implicate nurses or physicians to change their work organization or even leave their profession. Hence, intent to leave the respective position is the overarching term for intent leaving the organization or intent leaving the profession. Moreover, the inclusion of this broad definition of intent to leave resulted in a complete overview of determinants impacting the retention of nurses and physicians. Therefore, the bias in this systematic review due to the definition of intention to leave is minimal.
Moreover, most of the participants in the studies reviewed were female (nurses). Because there is a lack of research on this subject for male nurses and physicians, it could potentially generate gender bias and the presented results should be handled with care. Nevertheless, research showed in 2019 that only 14% of the proportion of nurses in Europe were male and consequently, consequently the majority of nurses are female. 233 Furthermore, this review only included studies written in English, which may have led to the exclusion of other valuable study findings.
Conclusion
Our findings have shown that the determinants identified in this systematic review, namely personal characteristics, job demands, employment services, working conditions, work relationships and organizational culture, impact, the job retention of nurses and physicians. Assessing the outcomes of this systemic review, management should take job satisfaction, career development and the work-life balance of their personnel seriously into account as 3 crucial factors in terms of job retention. Currently, the determinants identified in this systematic review can be used to design interventions or policies dedicated to increasing job retention and improving healthcare quality. The impact of the determinants could differ per hospital which should be taken into account designing the interventions. Therefore, it is desirable to fulfill future research to check which determinants are crucial in a specific hospital. Finally, an overview of interventions impacting the determinants described in this systematic review would be desirable expanding the adapted knowledge to stabilize the workforce of nursing and physicians in a hospital setting in the future.
Supplemental Material
sj-doc-2-inq-10.1177_00469580231159318 – Supplemental material for The Race to Retain Healthcare Workers: A Systematic Review on Factors that Impact Retention of Nurses and Physicians in Hospitals
Supplemental material, sj-doc-2-inq-10.1177_00469580231159318 for The Race to Retain Healthcare Workers: A Systematic Review on Factors that Impact Retention of Nurses and Physicians in Hospitals by Neeltje de Vries, Anke Boone, Lode Godderis, José Bouman, Szymon Szemik, Domenica Matranga and Peter de Winter in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-1-inq-10.1177_00469580231159318 – Supplemental material for The Race to Retain Healthcare Workers: A Systematic Review on Factors that Impact Retention of Nurses and Physicians in Hospitals
Supplemental material, sj-docx-1-inq-10.1177_00469580231159318 for The Race to Retain Healthcare Workers: A Systematic Review on Factors that Impact Retention of Nurses and Physicians in Hospitals by Neeltje de Vries, Anke Boone, Lode Godderis, José Bouman, Szymon Szemik, Domenica Matranga and Peter de Winter in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Correction (April 2023):
Article updated to remove Table 3 footnote and for few minor changes within text.
Author’s Note
We confirm that the listed authors have authorized the submission of their manuscript via third party and approved any statements or declarations, for example, conflicting interests, funding, etc.
Author Contributions
All authors contributed substantially to the concept and design, acquisition of the data or analysis and interpretation of the data, drafted the article or revised it critically for important intellectual content, and approved the final version to be published.
Disclaimer and Funding Source
The views expressed in the submitted article are those of the authors alone and may not reflect the official position of their respective institutions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: External funding was received for the development of this study: European Union, Chafea – 3rd Health Programme, Multi-beneficiary Project Grant (HP-PJ, HP-JA), Topic: PJ-01-2020-1, Type of action: HP-PJ, SEP-210693712: Project called METEOR (MEnTal hEalth: fOcus on Retention of healthcare workers).
The funding source did not influence the study design, the collection, analysis and interpretation of the data, the manuscript writing or the decision to submit the manuscript for publication. Both the views that are expressed and any errors or omissions are the sole responsibility of the authors.
Presence of Declarations,and Ethics and Consent Statements
For this systematic review no ethical/consent concerns were needed because no humans were involved. We only checked the available literature in three databases.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.