
Abstract
The primary method for preventing health and health-related problems in diabetic people is glycemic control. Numerous studies have documented the importance of glycemic control and the factors that influence it. However, the results are dispersed. This study sought to identify the prevalence of poor glycemic control and associated factors in Ethiopia. Findings will be crucial to reduce the burden of poor glycemic control. Comprehensive search was performed from databases: PubMed, Global Health, CINAHL, IRIS, and FSTA. Gray literature sources were also explored. This document was prepared based on the PRISMA flowchart. The protocol is registered in PROSPERO (ID: CRD42022296583). STATA software was used for data analyses and I2 test with Cochrane Q statistics, and forest plot were used to verify heterogeneity. When the I2 value was higher than 50% and the p-value was 0.05, heterogeneity was deemed significant. To confirm publication bias, a funnel plot with an Egger’s regression test was performed. The factors related to poor glycemic control were reported using pooled odds ratios (POR) and a 95% confidence interval. In this study, 46 papers totaling 15 457 people were used to calculate the pooled estimates. It was determined that 32.6% (95% CI: 28.3, 36.9) and 61.92% (95% CI: 57.92, 65.92) of the subjects, respectively, had good and poor glycemic control. Being male protected against poor glycemic control, while poor diet adherence, lack of exercise, poor adherence to anti-diabetic medications, and smoking increased the likelihood of poor glycemic control. Lack of formal education, no family history of diabetes, lack of glucometer for blood glucose monitoring, comorbidity, being overweight and prolonged length of stay with diabetes all contributed to poor glycemic control. Ethiopia had a fairly high rate of poor glycemic control. The main determinants are lifestyle factors. Therefore, it is important to focus on behavioral interventions.
We have been looking through various databases to see what other researchers have done. In the meantime, it has been discovered that systematic reviews and meta-analyses on poor glycemic control are scant in African countries like Ethiopia. Additionally, a wide range of factors, such as sociodemographic, health-related factors, organizational factors, and policy-related factors, are found to influence glycemic control.
Multiple factors were discovered to have a significant relationship with glycemic control in this study. The main factors were lifestyle-related factors. As a result, the current study’s findings could be critical in developing diabetes treatment and prevention strategies.
The study’s findings may result in a paradigm shift in the DM management process. As a result, policymakers and program planners could benefit from the study’s findings.
Introduction
Diabetes mellitus (DM) is a chronic multisystem disorder marked by hyperglycemia that affected 422 million people worldwide in 2014. It was responsible for 1.5 million deaths each year. 1 The global prevalence of diabetes continues to rise, with 537 million people expected to have the disease by 2021, with 3 out of every 4 adult patients living in low and middle income countries. It also contributed to the deaths of 6.7 million people worldwide in 2021. In Africa, 24 million (1 in 22 adults) have diabetes, with a projected increase to 55 million by 2045. It resulted in the deaths of 416 thousand Africans by 2021. 2 Similarly, diabetes is expected to affect 693 million people globally by 2045. 3 This is primarily due to an increase in obesity caused by lifestyle changes such as poor feeding practices (nutrition transitions) and insufficient physical activity. 4
There are various types of DM. Type 2 diabetes (due to insulin resistance), type 1 diabetes (due to autoimmune b-cell destruction), gestational DM, and other types of diabetes like neonatal diabetes, maturity-onset DM (MODY), and DM due to diseases of pancreas are all common types of diabetes. 5 However, type 1 diabetes (T1DM) and type 2 diabetes (T2DM) are the 2 most common public health burdens affecting people all over the world.4,6 This is supported by the fact that these types of diabetes are mostly associated with a variety of short and long-term morbidities and deaths. Cardiovascular diseases, neuropathy, nephropathy, retinopathy, skin impairment, hearing impairment, diabetic ketoacidosis (DKA), and premature death are the most common complications of diabetes.7-12
Diabetes-related health-care costs are undoubtedly high. In 2019, global DM expenditure was 760 billion USD, with projections of 825 billion USD and 845 billion USD by 2030 and 2045, respectively. 13 The worst economic consequences of diabetes were seen primarily in low and middle-income countries. 14 All of these unintended consequences of diabetes are linked to poor glycemic control. 15 In addition, precarious people with poor socio-economic status are more likely to have poor glycemic control as a result of excessive consumption of unhealthy foods such starches and sugary drinks, as well as poor adherence to medications and care. 16 The fact that prolonged exposure to social and economic deprivation is linked to poor health outcomes further supports this. 17 Thus, glycemic control (keeping blood glucose levels within normal ranges) is critical for reducing the burdens of diabetes, such as complications, hospitalization rates, and medical costs. It is also vital to improve the functional capacity of patients, the life expectancy and the overall health related quality of life.18,19 Glycemic control is especially important in low-income countries like Ethiopia for improving the quality of life of diabetes patients. A recent study in Ethiopia found that the economic burden of diabetes was significantly higher among the least privileged population. 20
With 1.9 million diabetics, or 3.3% of the population, Ethiopia is one of the top 5 countries in Africa. 21 The results of a meta-analysis in Ethiopia also showed that the overall prevalence of diabetes mellitus is 5.5%. 22 Diabetes mellitus has been a major public health challenge in the health care system with more than 5% of the population have undiagnosed DM. 23 This is associated with poor glycemic control. Several studies in Ethiopia have reported poor glycemic control level and factors associated with poor glycemic control in T1DM or T2DM patients. The primary study results are inconsistent, which can be attributed to a number of factors, including the use of various glycemic control measurements, variations in study setups, and study population. Poor glycemic control, for example, ranges from 29% 24 to 82.2%. 25 A meta-analysis of 16 studies found that only one-third of patients have good glycemic control. 26 As a result, aggregated evidences about the magnitude of poor or good glycemic control, as well as potential factors associated with poor glycemic control, are scarce in Ethiopia. Hence, the purpose of this systematic review and meta-analysis was to provide solid evidence on the prevalence of glycemic control and the determinants of poor glycemic control in Ethiopian diabetes patients. The current study’s findings will be vital for policymakers in developing strategies to reduce the overall burden of diabetes in Ethiopia.
Methods
Data Sources and Searching Strategies
The purpose of this study was to determine the pooled prevalence of glycemic control as well as the determinants of poor glycemic control in Ethiopia. To report the findings, the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guideline was used. 27 This study’s protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO) at the University of York Centre for Reviews and Dissemination (ID: CRD42022296583). Articles were obtained from a variety of databases and gray literature sources. PubMed (including MEDLINE), Global Health, Cumulative Index to Nursing and Allied Health Literature (CINAHL) (EBSCO), WHO’s Institutional Repository for Information Sharing (IRIS), and Food Science and Technology Abstracts (FSTA) were all searched extensively (EBSCO). In addition, gray literature sources such as Google, WorldCat, and Google Scholar were used to find articles. In order to retrieve additional articles, the reference lists of included articles and previous reviews were cross-checked. To manage articles, EndNote X8 software was used. All retrieved articles were exported to this software, which was then used to remove duplicated articles, extract data, and cite references. During the search, Boolean search operators such as “OR” and “AND” were used. Prior to searching, key terms were checked for appropriateness. To find articles in PubMed, the following search string was used (Appendix 1):
Eventually, we followed PICO to search articles:
Inclusion and Exclusion Criteria
Two authors chose the articles included in the current study (ZWB & AA). We evaluated article eligibility based on study region, sample size, type of diabetes, glycemic level measurement, study designs, titles, and abstracts. At the end, 2 authors evaluated the full texts in accordance with the pre-defined eligibility criteria (ZWB & DAJ). The observational studies (cross-sectional, case-control, and cohort) reporting glycemic control and factors associated with it were included in this systematic review and meta-analysis. The studies that reported an association using an odd ratio (OR) were included and the Cruds odd ratios (CORs) were used to calculate the pooled odds ratios (POR). The current study excluded systematic reviews and meta-analyses, non-human studies, qualitative studies, conference proceedings, case reports, case series, double publications using similar data, editorial comments, and studies conducted in languages other than English. Furthermore, because we were unable to identify the original cross tabulated data, we excluded some articles studies that did not report CORs based on a standard 2 by 2 table.
Data Extraction and Quality Assessment
To extract data from the included articles, a standard data extraction tool prepared in Microsoft Excel 2016 was used. Three investigators (ZWB, FBG, and ET) worked independently to extract data. The data was then cleaned and prepared for the final analysis using an Excel spreadsheet. Name of the author (s), publication year, and study region, age of study subjects, type of DM, study design, calculated sample sizes, final sample sizes, and measurements of glycemic control, good glycemic control, poor glycemic control, and factors associated with poor glycemic control were all included in the data extraction format. During the extraction process, disagreements between the authors were resolved through discussion with 2 authors (AS & MW) (see Supplemental S1 Table). For the quality assessment or critical appraisal of the articles, the Joanna Briggs Institute (JBI) Critical Appraisal Checklist for Observational Studies was used. 28 Two authors (ZWB and AA) independently assessed the quality of the work. Yes, No, Unknown, and Not Applicable are the options available in the tools. Yes, is assigned a one, and all other options are assigned a zero. The scores were totaled and converted to percentages. The current systematic review and meta-analysis included studies with a quality score of more than 50% (see Supplemental S2 Table). An inter-rater agreement was calculated using Cohen’s kappa coefficient (κ) prior to the inclusion of articles. The findings revealed significant agreement between the 2 raters (κ = 0.72, P < .001).
Measures of Variables
The primary outcome of the current study was the determinants of poor glycemic control. The other outcomes were the pooled prevalence of good and poor glycemic control among Ethiopian diabetes patients. Odd ratios were used to identify factors associated with poor glycemic control. The individual components of the factors were calculated as follows: a: the number of DM patients with poor glycemic control who were exposed to the possible factor; b: the number of DM patients with good glycemic control who were exposed to the possible factor; c: the number of DM patients with poor glycemic control who were exposed to the possible factor; and d: the number of DM patients with good glycemic control who were exposed to the possible factor. The CORs for the individual studies were then calculated (OR = ad/bc). Finally, the determinants of poor glycemic control were calculated using PORs with 95% confidence interval. Variables with POR that did not have one in the 95% CI were considered independent predictors of poor glycemic control. STATA software was used to compute the pooled estimates using the “metan” command. The effect sizes were log odds ratios indicating the factors associated with poor glycemic control in Ethiopian diabetes patients. The log odds ratios were converted to exponent of log odds (POR = elogOR) to report the factors.
The primary studies used different references for poor glycemic control. As a cut point for poor glycemic control, most studies used FBG > 130 mg/dl or FBG < 70 mg/dl. HbA1C>7% was used as a cut point in some studies, while FBG > 154 mg/dl and FBG ≥ 126 mg/dl were used in others to declare poor glycemic control. The pooled prevalence of poor glycemic control was calculated in this meta-analysis using the cut points for poor glycemic control. This was done to account for potential sources of heterogeneity and to reduce bias caused by differences in the primary studies’ reference points for poor glycemic control.
Analysis and Statistical Methods
STATA Version 16 (STATA Corporation, College Station, Texas) software was used to compute the pooled odds ratios in this study. Pooled estimates were computed using both random and fixed effect models. Due to the high heterogeneity among the included studies, the final pooled estimates were reported using a random-effect model weighted using the inverse variance method. Subgroup and sensitivity analysis, as well as univariate Meta regression, were used to confirm the possible sources of heterogeneity among the included studies. The 95% CIs for the pooled estimates were provided. Meta-analysis results were presented using a forest plot, text, and summary tables. The asymmetry of the funnel plot was used to check for publication bias, which was confirmed by Egger’s regression test at a 5% significant level. 29 To detect heterogeneity among studies, the forest plot, I 2 test, and Cochrane Q statistics were used. 30 I 2 values of 25%, 50%, and 75%, respectively, were interpreted as low, medium, and high heterogeneity. 31 In the current study, heterogeneity was considered significant when the I 2 value was 50% and above with P < .05.
Results
Article Identification
The initial search yielded 606 articles. These articles were discovered from reputable databases and gray literature sources. After removing 225 duplicated articles, a total of 381 articles were screened for titles and abstracts. After reviewing the titles and abstracts, 320 articles were removed. The full texts of 61 articles were examined. In the next phase, 15 articles were excluded due to in consistent results,32-40 incompleteness of records, 41 poor quality of articles,42-45 and duplicated publication. 46 Finally, 46 articles were found eligible to this study. Of these articles, 9 articles were excluded from meta-analyses of different factors due to the fact that some articles did not report factors or did not properly report the factors.25,47-54 The pooled prevalence of good and poor glycemic control in Ethiopia was estimated using all 46 articles (Figure 1).

PRISMA flow chart showing the selection process to compute glycemic control and associated factors of poor glycemic control in Ethiopia.
Description of Articles
The total calculated sample size of 46 articles was 16 135 in the current study, of which 15 457 study population were included to estimate the pooled prevalence glycemic control, yielding a non-response rate of 4.18%. The pooled prevalence of good glycemic control was calculated from 5918 of the 15 457 study population and poor glycemic control was calculated from 9539 of the 15 457 study population. The original articles’ sample sizes ranged from 10024,55 to 2554. 49 Likewise, articles published between 2012 and 2021 were included in this study. In terms of the studies included in estimating the good prevalence of glycemic control, the lowest proportion (17.8%) was reported in a study conducted among T2DM patients in Addis Ababa, whereas the highest prevalence (71%) was reported in a study conducted in SNNP among both diabetic cases. Similarly, the lowest and highest rates of poor glycemic control were 29% 24 and 82%, 25 respectively. In this study, 43 articles were cross sectional studies and 4 (2 each) were cohort48,56 and case control studies.57,58 Besides, 30 articles were conducted among T2DM patients and the study participants of 17 of studies were both T1DM and T2DM patients. Furthermore, 17 of the 46 articles were conducted in the Oromia region, while 11 were conducted in the Amhara region. Seven articles were published in Addis Ababa, and others were published in the SNNP (4 articles), Tigray region (4 articles), Harari region (1 article), and Dire Dawa city administration (2 articles). Finally, the qualities of the articles were evaluated using a JBI checklist. Thus, 22 articles were categorized as high quality, while 19 and 5 articles were categorized as medium and low quality, respectively.
The Pooled Prevalence of Glycemic Control
In the present meta-analysis, the pooled prevalence of good and poor glycemic control in Ethiopia was estimated using 46 articles.19,24,25,47-89 In a random effect model, the pooled prevalence of good glycemic control was found to be 38.08% (95% CI: 34.08, 42.08) with significant heterogeneity among the included articles (I 2 = 96.57%, P < .001) (Figure 2). The potential sources of higher heterogeneity were investigated further. Initially, publication bias was investigated by inspecting the funnel plot, which was discovered to be asymmetric (Figure 3). Begg’s test confirmed the presence of publication bias, with the result indicating publication bias (P = .004). The Egger’s regression test, on the other hand, revealed no publication bias (P = .398). As a result, the DerSimonian-Laird trim fill analysis was carried out. Nine articles were imputed as a result of the 5-step iteration, and the pooled prevalence of good glycemic control was found to be 32.6% (95% CI: 28.3, 36.9). This demonstrates that the pooled prevalence of good glycemic control was calculated using data from 55 articles (Figure 3).

Forest plot (pooled prevalence of good glycemic control in Ethiopia).

Funnel plots: (A) funnel plot of log prevalence of good glycemic control and (B) funnel plot of good glycemic control after trim fill analysis.
A random effect model was also used to calculate the pooled prevalence of poor glycemic control. It was estimated that 61.92% (95% CI: 57.92, 65.92) of diabetes patients had poor glycemic control, with significant heterogeneity among the articles included in this meta-analysis (I 2 = 96.57%, P < .001) (Figure 4). The sources of heterogeneity were further explained. The funnel plot appeared asymmetric (Figure 5), and the Begg’s correlation test was significant (P = .004), indicating the presence of publication bias due to unreported small study effects. Nonetheless, the Egger’s regression test was found to be insignificant (P = .398). As a result, the DerSimonian-Laird trim fill analysis was also run, but the pooled estimate remained unchanged. The sensitivity analysis was then performed to identify specific articles that may have contributed to the higher heterogeneity. However, no single study discovered a significant effect for greater heterogeneity. Rather, the individual prevalence 95% CIs were outside the pooled estimate’s 95% CI in either the lower or upper confidence intervals. Finally, using sample size, univariate meta-regression was executed to identify potential sources of heterogeneity. The sample size, however, was not found to be a significant source of heterogeneity (Table 1).
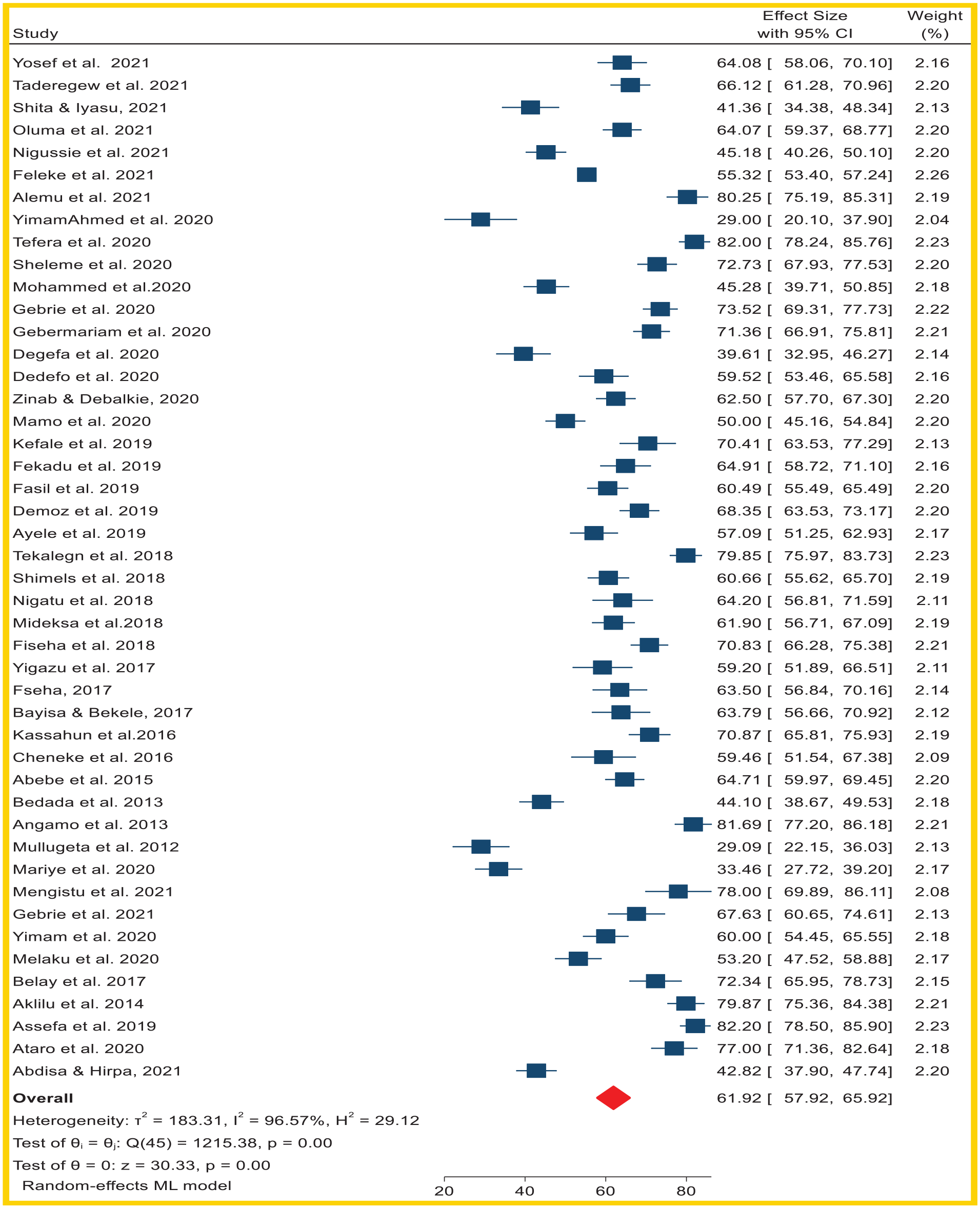
Forest plot (pooled prevalence of poor glycemic control in Ethiopia).
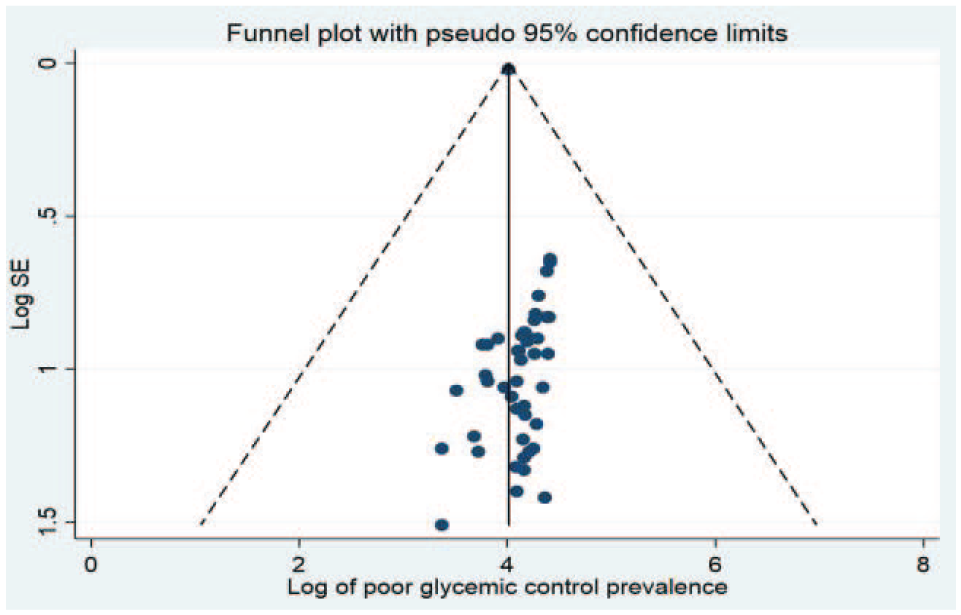
Funnel plot (pooled prevalence of poor glycemic control in Ethiopia).
Meta-Regression Using Sample Size.

Subgroup Analysis (Poor Glycemic Control) in Ethiopia
A meta-analysis of subgroups based on region revealed that Dre Dawa had the highest prevalence, with 54.78% (95% CI: 51.09, 58.46) of patients having poor glycemic control. Similarly, among T2DM patients, the pooled prevalence of poor glycemic control was higher (38.86%, 95% CI: 32.17, 45.54). A subgroup analysis using glycemic control references revealed that 46.66% (40.07, 53.26) of patients had poor glycemic control (Table 2).
Poor Glycemic Control (Subgroup Analysis) in Ethiopia.
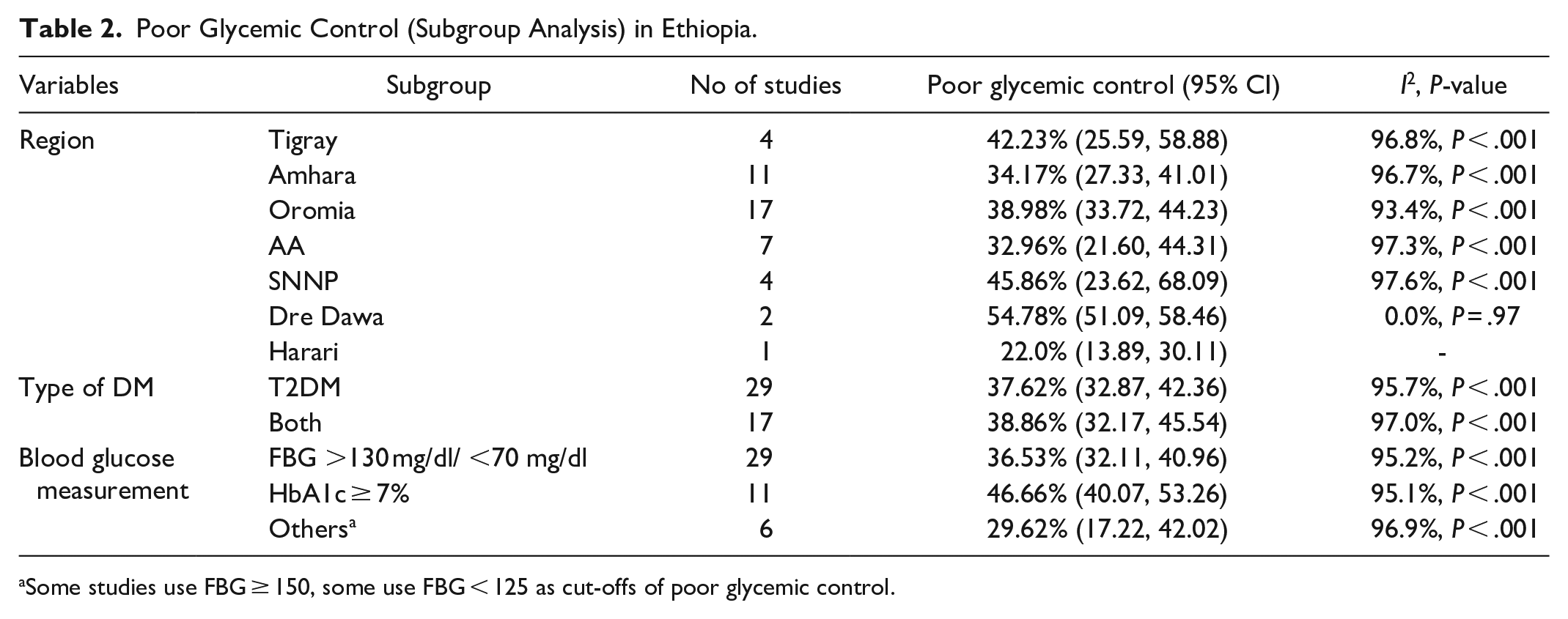
Some studies use FBG ≥ 150, some use FBG < 125 as cut-offs of poor glycemic control.
Factors Associated With Poor Glycemic Control in Ethiopia
A total of 19 variables were found to be meta-analyzable in this systematic review and meta-analysis. Eleven of the 19 factors associated with poor glycemic control were found to be significantly associated with poor glycemic control. Gender, level of education, weight, compliance with dietary and exercise recommendations, compliance with anti-hyperglycemic medication, smoking, comorbidities, length of stay with DM, self-monitoring of glucose level, and family history of DM were all substantially associated with poor glycemic control.
Gender was found to be a significant predictor of poor glycemic control in this study, with males having a 31% lower likelihood of poor glycemic control than females (POR = 0.69, 95% CI: 0.53, 0.88, I 2 = 82%, P < .001). Similarly, the educational level of DM patients was found to be significantly related to glycemic control. Poor glycemic control was 1.54 times more likely in patients with no formal education than in patients with formal education (POR = 1.54, 95% CI: 1.28, 1.87, I 2 = 50.6%, P = .006). When compared to normal weight DM patients, the odds of having poor glycemic control was 1.43 times higher in the overweight groups (POR = 1.43, 95% CI: 1.01, 2.06, I 2 = 74.5%, P < .001). According to the current meta-analysis, lifestyle factors such as adherence to exercise recommendations, dietary recommendations, adherence to antiglycemic drugs, and smoking were significantly associated with poor glycemic control. Diabetes patients who did not follow exercise recommendations were more likely to have poor glycemic control than those who did (POR = 2.14, 95% CI: 1.61, 2.84, I 2 = 74.4%, P < .001). Poor glycemic control was 3.30 times more likely in patients with poor adherence to diabetic diets than in those with good dietary adherence (POR = 3.30, 95% CI: 2.14, 5.08, I 2 = 84.2%, P < .001). Poor glycemic control was more common in patients with poor drug adherence than in their counterparts (POR = 3.77, 95% CI: 2.22, 6.40, I 2 = 87.5%, P < .001). Patients with comorbidities were also more likely to have poor glycemic control (POR = 1.38, 95% CI: 1.05, 1.82, I 2 = 71.4%, P < .001). Smokers were twice as likely as non-smokers to have poor glycemic control (POR = 2.07, 95% CI: 1.25, 3.42, I 2 = 60.8%, P = .037). The length of stay with diabetes since the initial diagnosis was significantly related to glycemic control. Patients with diabetes for 10 years or more were 1.62 times (95% CI: 1.14, 2.31, I 2 = 75.3%, P < .001) more likely to have poor glycemic control than patients with diabetes for less than 10 years. Poor glycemic control was more common in patients who did not regularly monitor their blood glucose levels than in those who did (POR = 2.26, 95% CI: 1.40, 3.66, I 2 = 86%, P < .001). Likewise, patients with no family history of diabetes were 1.63 times more likely to have poor glycemic control (95% CI: 1.11, 2.41, I 2 = 75.7%, P < .001) than patients with family history of DM (see Supplemental S2 Figures, Table 3).
Determinants of Poor Glycemic Control in Ethiopia.
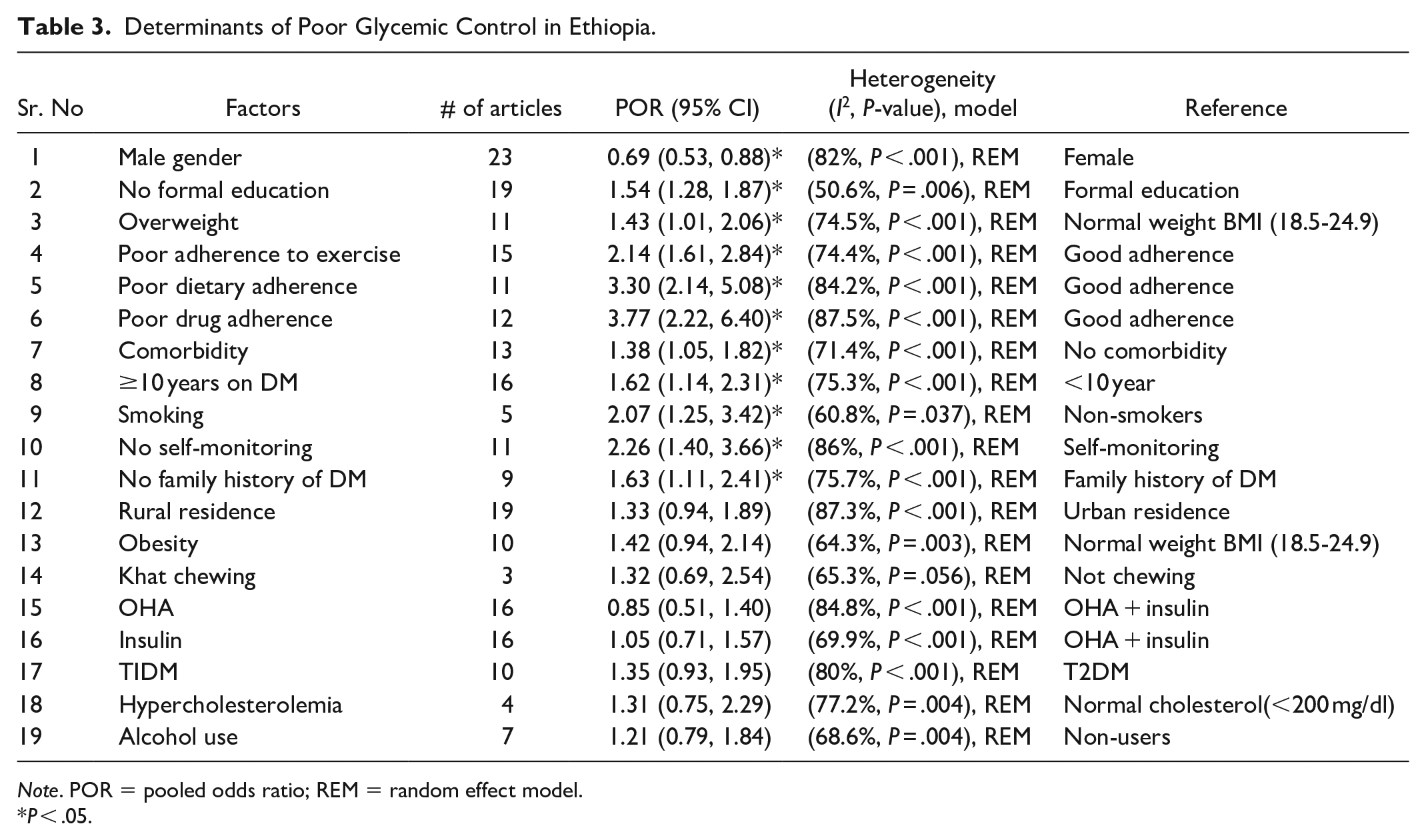
Note. POR = pooled odds ratio; REM = random effect model.
P < .05.
Eight variables, however, did not show a significant association with poor glycemic control. These variables include place of residence, intake of OHAs, insulin intake, obesity, type of diabetes, hypercholesterolemia, khat chewing, and alcohol consumption (see Supplemental S1 Figures, Table 3).
Discussion
The purpose of this systematic review and meta-analysis is to determine the pooled prevalence of poor or good glycemic control in Ethiopia. The current study’s main goal is also to identify the factors associated with poor glycemic control. Using a random effect model, the pooled prevalence of good or poor glycemic control is calculated from 46 articles. Similarly, 19 variables were found to be meta-analyzable for determining the determinants of poor glycemic control, with 11 variables significantly associated with poor glycemic control among Ethiopian diabetes patients.
In this study, only one-third (32.6%) of DM patients in Ethiopia have good glycemic control which is lower than a previous meta-analysis finding in Ethiopia where 34.4% of DM patients had good glycemic control. 26 The discrepancy could be due to a difference in the number of articles used for meta-analysis, as the current study used 46 articles while the previous one used 16 to compute the pooled prevalence. Thus, the pooled estimate in the current meta-analysis is more representative than the previous one. In Ethiopia, however, 62% of DM patients have poor glycemic control, with significant regional variation. Dire Dawa has the highest pooled prevalence of poor glycemic control (54.78%), while Addis Ababa has the lowest (32.96%). Similarly, poor glycemic control is substantially higher (47%) among patients whose glycemic level was determined using HbA1C ≥ 7%. This meta-analysis of poor glycemic control is the first of its type in Ethiopia. The magnitude of pooled poor glycemic control is lower than the findings of individual studies conducted in Saudi Arabia (74.6%, 74.9%),90,91 Kenya (65.1%), 92 Bangladesh (82%), 93 India (78.2%), 15 Morocco 66.3%, 94 and Dares Salaam (69.7%) 95 as well as a recent finding in Ethiopia where 72.5% patients with T2DM have poor glycemic control. 96 However, it is lower than the findings in China and Zimbabwe, where 57.3% 97 and 58.2% 98 of diabetic patients had poor glycemic control, respectively. The differences in the sample size, study population, and reference points indicating glycemic control may be associated with differences in the elucidation of these discrepancies. Individual studies included in this meta-analysis used FBG as a glycemic control measure, whereas the majority of the comparator studies used HbA1C cut points to determine glycemic control. Besides, none of the studies used as a comparator in this meta-analysis were meta-analyses, which could be the source of variation. Furthermore, patients’ low socioeconomic status may be related to Ethiopia’s increased prevalence of poor glycemic control. This is corroborated by the fact that most of the factors determining poor glycemic control are correlated to socio-economic status. This is supported by previous reports that depicted patients with socio-economic disadvantage are liable poor outcome to DM.99,100 This finding was also backed by economic development theories, which state that those with low economic status are more likely to have poor health and health service inequalities. 101 Due to the high costs of DM care and treatment, it is unavoidable that the majority of Ethiopian patients with diabetes will have poor glycemic control. A recent study on the financial impact of diabetes revealed that diabetic care costs US $ 38.23 per month, which is more than a significant portion of the Ethiopian population earns on a monthly basis. 102 Therefore, socio-economic empowerment of patients could be vital to trim the burden of DM in Ethiopia.
Regarding the determinants of poor glycemic control, factors related to life style (self-monitoring, drug adherence, dietary adherence, adherence to exercise, and smoking) and other factors named by gender, educational status, weight, family history of DM, comorbidities, duration of stay with DM have been found to be significantly associated with poor glycemic control. Poor glycemic control is more likely in DM patients who do not measure blood glucose levels or who do not have the HemoCue machine than in patients who practice self-monitoring. This is linked to poor self-monitoring practice among Ethiopian patients, as evidenced by a meta-analysis finding in Ethiopia, where only one-third of patients had good self-monitoring practice. 103 This is because patients who have good self-monitoring practice may adhere to diabetic cares. As a result, the possibility of DM-related complications such as poor glycemic control is lower in these patients. Diabetes patients who do not properly take their anti-hyperglycemic (anti-diabetic) medications are more likely to have poor glycemic control. It is obvious that adhering to anti-diabetic medications is critical for maintaining normal blood glucose levels. However, only one-third (69.5%) of diabetic patients in Ethiopia adhere to anti-diabetic medications. 104 In the current study, poor adherence to dietary recommendations in DM patients is also an important determinant of poor glycemic control. The possible explanation is that DM patients who follow DM-recommended diets, such as high plant-based diets, moderate intake of fish and dairy products, and low red meat intake, are more likely to control and prevent DM-related complications. 105 However, adherence to recommended diets may be ineffective in controlling glycemic levels if not supplemented with physical activity. 105 This is supported by the findings of the current meta-analysis that DM patients who adhere poorly to exercise recommendations are more likely to have poor glycemic control. In Ethiopia, both dietary practices and physical activity adherence are relatively low in DM patients. 103 Furthermore, smoking has been linked to poor glycemic control. This could be because nicotine impairs glucose metabolism, including B-cell function, which leads to insulin resistance.106,107 Thus, smoking increases the likelihood of T2DM and worsens poor glycemic control.
In the present study, males are at lower likelihood of poor glycemic control than females. The possible justification of gender disparity could be associated with lower physical activity level of females,108,109 and feeding practice of women in which females usually consume sweet foods with high glycemic index in Ethiopia. Also, the high calorie food consumed during the puerperal period by females and physiologic difference could be the source of gender disparity. Furthermore, variations in homeostasis, treatment response, and psychological factors may all contribute to variation. 110 The educational level is significantly associated with poor glycemic control, with patients with no formal education being more likely to have poor glycemic control than patients with formal education. This could be because diabetic education is the most effective strategy for glycemic control, and uneducated patients may have difficulty accessing DM related information. 111 Overweight patients are more likely than normal-weight patients to have poor glycemic control. When an individual’s BMI is above the normal range, he or she is more likely to develop insulin resistance. 112 Similarly, family history has been found to have a significant impact on glycemic control. DM patients with no family history of diabetes have a higher risk of poor glycemic control than patients with a family history of diabetes. A lack of awareness about prevention methods and the importance of early diagnosis could be one explanation. Patients with a family history of diabetes, on the other hand, may be more aware of early diagnosis and treatment options, potentially reducing the risk of poor glycemic control. In Ethiopia, most DM patients are aware of their condition only when they experience symptoms. 23 This increases the risk of poor glycemic control. This justification is supported by the current study’s meta-analysis finding that patients with DM for 10 years or more are more likely to have poor glycemic control. Other evidences, however, showed that patients with a family history of diabetes were more likely to have poor glycemic control, which could be linked to genetics, particularly in T2DM patients. 113 Finally, the presence of comorbidities has been found to increase the likelihood of poor glycemic control. Previous evidence suggests that comorbidities impair glycemic control primarily in patients with T2DM, though the mechanism varies depending on the comorbidity.114,115 Comorbidities such as musculoskeletal diseases, for example, may lower HbA1C at diagnosis, but it may then rise and remain stable for several years. 115 The current study found no statistically significant difference in poor glycemic control between T1DM and T2DM patients.
In general, this study attempted to investigate all potential determinants of poor glycemic control. The pooled prevalence of glycemic control is also determined, which provides policymakers, program planners, and researchers with useful information. Another strength of the current study is that multiple sources were used to find articles. The articles included in this meta-analysis, on the other hand, used different reference points (cut points) to estimate glycemic control. Sub-group analysis was performed to handle heterogeneity. However, we were unable to separate glycemic control in T1DM and T2DM patients because all of the articles used in this study were performed on T2DM patients or both. This could conceal the true magnitude glycemic control.
Conclusion
In summary, poor glycemic control is considerably high in Ethiopia. It has been discovered that being male improves glycemic control. However, DM patients who do not adhere to anti-hyperglycemic drugs, exercise, dietary recommendations and smokers are at higher risk of poor glycemic control. Besides, being illiterate, being overweighed, having no family history of DM, not self-monitoring of blood glucose, the presence of comorbidities, and prolonged duration of stay with DM prohibited glycemic control. There is no statistically significant difference in glycemic control between T1DM and T2DM patients. In general, life style related factors or behavioral factors are the main determinants of poor glycemic control in Ethiopia. As a result, treatments for DM patients should be designed considering multitude of factors. Behavioral interventions along with economic empowerment could decrease the burden of poor glycemic control and related complications in Ethiopia. Economic empowerment can help DM patients practice self-care more effectively and might boost their quality of life.
Supplemental Material
sj-doc-2-inq-10.1177_00469580231155716 – Supplemental material for Prevalence of Glycemic Control and Factors Associated With Poor Glycemic Control: A Systematic Review and Meta-analysis
Supplemental material, sj-doc-2-inq-10.1177_00469580231155716 for Prevalence of Glycemic Control and Factors Associated With Poor Glycemic Control: A Systematic Review and Meta-analysis by Zebenay Workneh Bitew, Ayinalem Alemu, Desalegn Abebaw Jember, Erkihun Tadesse, Fekadeselassie Belege Getaneh, Awole Seid and Misrak Weldeyonnes in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-1-inq-10.1177_00469580231155716 – Supplemental material for Prevalence of Glycemic Control and Factors Associated With Poor Glycemic Control: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-inq-10.1177_00469580231155716 for Prevalence of Glycemic Control and Factors Associated With Poor Glycemic Control: A Systematic Review and Meta-analysis by Zebenay Workneh Bitew, Ayinalem Alemu, Desalegn Abebaw Jember, Erkihun Tadesse, Fekadeselassie Belege Getaneh, Awole Seid and Misrak Weldeyonnes in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-3-inq-10.1177_00469580231155716 – Supplemental material for Prevalence of Glycemic Control and Factors Associated With Poor Glycemic Control: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-3-inq-10.1177_00469580231155716 for Prevalence of Glycemic Control and Factors Associated With Poor Glycemic Control: A Systematic Review and Meta-analysis by Zebenay Workneh Bitew, Ayinalem Alemu, Desalegn Abebaw Jember, Erkihun Tadesse, Fekadeselassie Belege Getaneh, Awole Seid and Misrak Weldeyonnes in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-4-inq-10.1177_00469580231155716 – Supplemental material for Prevalence of Glycemic Control and Factors Associated With Poor Glycemic Control: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-4-inq-10.1177_00469580231155716 for Prevalence of Glycemic Control and Factors Associated With Poor Glycemic Control: A Systematic Review and Meta-analysis by Zebenay Workneh Bitew, Ayinalem Alemu, Desalegn Abebaw Jember, Erkihun Tadesse, Fekadeselassie Belege Getaneh, Awole Seid and Misrak Weldeyonnes in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-5-inq-10.1177_00469580231155716 – Supplemental material for Prevalence of Glycemic Control and Factors Associated With Poor Glycemic Control: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-5-inq-10.1177_00469580231155716 for Prevalence of Glycemic Control and Factors Associated With Poor Glycemic Control: A Systematic Review and Meta-analysis by Zebenay Workneh Bitew, Ayinalem Alemu, Desalegn Abebaw Jember, Erkihun Tadesse, Fekadeselassie Belege Getaneh, Awole Seid and Misrak Weldeyonnes in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-6-inq-10.1177_00469580231155716 – Supplemental material for Prevalence of Glycemic Control and Factors Associated With Poor Glycemic Control: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-6-inq-10.1177_00469580231155716 for Prevalence of Glycemic Control and Factors Associated With Poor Glycemic Control: A Systematic Review and Meta-analysis by Zebenay Workneh Bitew, Ayinalem Alemu, Desalegn Abebaw Jember, Erkihun Tadesse, Fekadeselassie Belege Getaneh, Awole Seid and Misrak Weldeyonnes in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-docx-7-inq-10.1177_00469580231155716 – Supplemental material for Prevalence of Glycemic Control and Factors Associated With Poor Glycemic Control: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-7-inq-10.1177_00469580231155716 for Prevalence of Glycemic Control and Factors Associated With Poor Glycemic Control: A Systematic Review and Meta-analysis by Zebenay Workneh Bitew, Ayinalem Alemu, Desalegn Abebaw Jember, Erkihun Tadesse, Fekadeselassie Belege Getaneh, Awole Seid and Misrak Weldeyonnes in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We are grateful to the authors of original studies included to the current study.
Author’s Note
Erkihun Tadesse is also associated with Sydney Medical School, Faculty of Medicine and Health, The University of Sydney, Sydney, NSW, Australia.
Authors’ Contribution
Zebenay Workneh Bitew, Ayinalem Alemu, Dessalegn Abebaw Jember, Erkihun Tadesse, Awole Seid, and Misrak Weldeyonnes contributed equally.
Availability of Data and Materials
The data that support the review findings of this study are included in the manuscript and in the supplementary files.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.