
Abstract
This study evaluates inpatients’ ontological insecurity and daily epidemic prevention behavior during the pandemic and explores the factors influencing daily epidemic prevention behaviors. The outbreak of coronavirus disease (COVID-19) in December 2019 caused a global public health crisis that has affected the very structure of society and the order of daily life. Ontological security is the ability to predict the impact of changes in social environments on personal security, such as during the pandemic. A cross-sectional study was used to collect data from 1185 inpatients of a hospital in Zhejiang, China, from July 11 to August 9, 2021. Our questionnaire recorded information on demographics, ontological insecurity, and daily epidemic prevention behaviors. The Mann-Whitney U test, Kruskal-Wallis H test, Spearman’s correlation analysis, and logistic regression analysis were used to determine the influencing factors of daily epidemic prevention behavior on ontological security. Results showed a negative correlation between inpatients’ ontological insecurity and daily epidemic prevention behavior (r = −.253, P < .001). The logistic regression analysis showed that the independent factors affecting daily epidemic prevention behavior include ontological insecurity (OR: 0.952; 95% CI: 0.937-0.968) (P < .001), sex (OR: 1.292; 95% CI: 1.004-1.663), age (OR: 0.880; 95%: 0.790-0.980), education (OR: 1.307; 95% CI: 1.098-1.556), and occupation [famers vs civil servants, staff or professional (OR: 0.596; 95% CI: 0.374-0.949),other versus civil servants, staff, or professional (OR: 0.693; 95% CI: 0.503-0.953)] (P < .05). Inpatients were shown to have good ontological security during the COVID-19 epidemic, younger patients, female patients, patients with stronger ontological security, patients with a higher educational level, and those who work in a fixed unit or organization showed higher levels of daily epidemic prevention behavior. Hospital managers should strengthen the intervention management of epidemic prevention behavior based on patient characteristics.
What do we already know about this topic?
Studies show that ontological security can predict the impact of changes in the social environment on personal security during a disease pandemic, and that it has a beneficial early warning effect on people’s behavior trends in times of crisis. Against the backdrop of the COVID-19 pandemic, people’s ontological security has been impacted to different degrees.
How does your research contribute to the field?
In this study, most inpatients were shown to have good ontological security and the patients’ ontological insecurity was negatively correlated with their daily epidemic prevention behavior which offers new insights on the ontological security of inpatients, particularly during the current pandemic.
What are your research’s implications toward theory, practice, or policy?
Based on our results, hospitals should formulate corresponding behavior intervention strategies to improve the level of daily epidemic prevention behaviors and boost publicity and education to address weak links and should implement personalized health education that is based on patients’ characteristics, to effectively improve their compliance with daily epidemic prevention behaviors.
Introduction
The outbreak of coronavirus disease (COVID-19) in December 2019 led to a major public health crisis on a global scale. 1 As of August 2021, the number of COVID-19 infections worldwide is still rising, and the activities of 60% of the world’s population are affected by it. 2 Various countries’ governments and public health organizations have worked hard to formulate appropriate control measures, such as travel restrictions, social distancing requirements, and the suggested use of—or even mandated use of—facial masks and frequent hand washing to suppress the spread of COVID-19 and reduce the infection rate.3,4
Research has shown that people’s epidemic prevention behaviors were greatly influenced by their knowledge, physical health status, psychological factors, perceived susceptibility, and perceived severity concerning COVID-19 and mediated by their trust in the healthcare system.5-11 Rad et al 12 found that trust in the healthcare system, fear of COVID-19, and positive attitude toward vaccination were significantly higher in vaccinated participants compared to those who were unvaccinated. Chung et al 13 examined psychological distress and protective behaviors across different populations. They showed that, despite the greater COVID-19 severity and fear of COVID-19 in Hong Kong, the general population in Hong Kong experienced less psychosocial distress with higher compliance to protective behaviors than the other groups in Taiwan. Alijanzadeh et al 14 recently showed that fear of COVID-19, trust in the healthcare system, or both (fear of COVID-19 and trust in the healthcare system) mediated the association between an individual’s risk perception and performing preventive COVID-19 behaviors. These studies further showed that the current pandemic broke the original form of society and affected the order of people’s daily lives—causing not only a series of social and economic problems but also varying degrees of psychological stress responses.
Individuals have an innate desire to maintain a sense of continuity and constancy in their lives and the world around them; however, this ordered state, and one’s very identity, can be threatened by the perceived experience of scarcity. Known as ontological insecurity. 15 Ontological security is usually integrated into daily life and is not conventionally perceived by people. Conversely, when drastic changes threaten their external environment, the concept of ontological security becomes more prominent and perceptible. 16 This change in awareness occurs because the drastic changes in the external environment often disrupt people’s daily life order and the stable interaction between people and the environment; this has a long-lasting negative effect on the state of psychological security formed in the stable environment. This disruption of order and stability can lead to uncertainty and loss of agency, diminished confidence in one’s self-identity, and, subsequently, a heightened motivation to regain a sense of control by reestablishing predictability and order to the world around them. 17 Responses to the experience of ontological insecurity range from increased anxiety, stress, and fear, to feelings of helplessness, loneliness, need for connection, and mortality salience. 15 In turn, ontological insecurity evokes a host of behavioral responses to help alleviate the uncertainty caused by the disruption of order and stability in one’s life.
Against the backdrop of the COVID-19 pandemic, people’s ontological security has been impacted to different degrees. 18 Studies show that ontological security can predict the impact of changes in the social environment on personal security during a disease pandemic and that it has a beneficial early warning effect on people’s behavior trends in times of crisis. Yang et al 19 showed that the pandemic-induced scarcity perception of ontological security could promote migrant workers’ risk-taking tendency, while Leary et al 20 found that it could stimulate people’s consumption. However, there are few reports on inpatients’ level of ontological security and its impact on daily epidemic prevention behavior under the normalization of the current COVID-19 pandemic situation. The current cross-sectional survey, therefore, investigates the ontological insecurity and daily epidemic prevention behavior of 1185 inpatients and analyzes the correlation between these 2 factors to provide a reference basis for hospitals to formulate prevention and control norms for inpatients.
Methods
Participants
We conducted a cross-sectional survey and used a logistic regression analysis model to calculate the effects of predictors on the outcome, assuming an odds ratio of 1.3 and PrH0 of 0.2 with a significance level of 5% and 95% power. The target sample size was 988 participants. We allowed for a 10% participant dropout (reluctance to participate in surveys) and selected 1097 participants as a conservative sample size. The sample size was calculated using G*Power 3.1.9.2 software. In this survey, our target population was hospitalized patients in Taizhou Hospital of Zhejiang Province, a general tertiary hospital with 1100 beds. Patients younger than 18 years old were excluded. In addition, participants who took <2 min to answer the questionnaire were also excluded. Moreover, repeat responses were subject to the first submission. A total of 1223 hospitalized patients volunteered to participate and completed the questionnaire from July 8 to August 11, 2021. Ultimately, of 1223 participants, 1185 responses were valid (96.9% valid response rate). The present study was exempted from the requirement for written informed consent and was approved by the Ethics Committee of Taizhou Hospital of Zhejiang Province (approval number: K20210521) in China. All procedures were performed in accordance with the guidelines of the institutional ethics committee of the authors and adhered to the tenets of the Declaration of Helsinki.
Survey Tools
The questionnaire comprised 3 parts: (1) demographic information, including age, sex, residence, education, and occupation, and (2) an ontological insecurity scale.21,22 The scale consists of 9 items, each answered on a Likert-type scale with “strongly disagree, disagree, neutral, agree, and strongly agree,” counting for 0 to 4 points, respectively. The scores of each item are added to obtain the total score of this category; the total score range is 0 to 36. The higher the total score, the worse the individual’s sense of ontological security. A score below 50% (ie, score <18.0) was set as the upper-middle level of ontological security. The Cronbach’s α of the scale is .950, indicating good reliability. (3) The last section is a daily epidemic prevention behavior questionnaire. This section is divided into 3 dimensions: 13 items for hand washing, 9 items for wearing masks, and 4 items for maintaining social distance, for a total of 26 items. Questions are also answered on a Likert-type scale with “never, occasionally, often, and always” counting 0 to 3 points, respectively. The total score range is 0 to 78, and the higher the total score, the more active the individual’s daily epidemic prevention behavior is. Total scores of 80% (ie, score ≥62.4) and up indicates a high level of epidemic prevention behavior, while a total score of less than 80% (ie, score <62.4) indicates a low level of epidemic prevention behavior. The Cronbach’s α of the questionnaire is .964. More details about the questionnaire could refer to the Supplemental Material.
Data Collection and Quality Control Methods
We conducted an online questionnaire survey using the “Questionnaire Star” platform. Information provided indicated the purpose, completion instructions, precautions, and confidentiality measures relating to the questionnaire. Respondents completed the questionnaire on their mobile devices. After integrated training, the questionnaire collectors explained the purpose, significance, and content of the survey to the patients before filling in the questionnaire. After obtaining informed consent, patients were invited to participate in the survey and sent the Questionnaire Star QR code. Respondents were not allowed to forward the QR code to others to fill in. When completing the questionnaire, you can only move on to the next item after completing the required items to ensure the integrity of each questionnaire. After questionnaires were completed and returned, ID numbers were used as unique identification codes, and any repeated questionnaires were excluded.
Statistical Analysis
We used SPSS software v 24.0 for data analysis. Data that were not normally distributed were tested by nonparametric tests. The measurement data were statistically described using M (P25, P75), and the counting data were statistically described by frequency and percentage. For the univariate analysis, we used the Mann-Whitney U test, Kruskal-Wallis H test, or Spearman’s correlation analysis. For the multivariate analysis, we used logistic regression analysis. The dependent variable was daily epidemic prevention behavior; the independent variables were age, sex, residence, education, occupation, and ontological insecurity. The significance level is a = 0.05.
Results
Characteristics of Inpatients
In this study, a total of 1223 hospitalized patients completed the survey, with 1185 responses being valid, of which 542 were male (45.7%) and 643 were female (54.3%). The median age of patients was 53 (38, 65) years; 253 patients (21.4%) lived in cities, 303 (25.6%) in towns, and 629 (53.1%) lived in rural areas (Table 1).
Single Factor Analysis of Patients’ Daily Epidemic Prevention Behavior (N = 1185).

Z value
χ2 value.
Patients’ Ontological Insecurity and Daily Epidemic Prevention Behavior
The median score for ontological insecurity was 13 (9,18). The median for daily epidemic prevention behavior was 63 (51,76), and the median score per item for daily epidemic prevention behavior, wearing masks, maintaining social distance, and hand washing were 2.42 (1.96,2.90), 2.67 (2,3), 2.00 (1.53,3.00), and 2.381 (1.85,2.92), respectively.
Single-Factor Analysis of Patients’ Daily Epidemic Prevention Behavior
The single-factor analysis results regarding participants’ prevention behaviors are shown in Table 1. There were significant differences in the scores for daily epidemic prevention behaviors in terms of gender, age, residence category, education, and occupation (P < .001)
Correlation Analysis of Patients’ Ontological Insecurity and Daily Epidemic Prevention Behavior
We performed a Spearman’s correlation analysis to determine the correlation between patients’ ontological insecurity and daily epidemic prevention behavior (r = −.253, P < .001). (Table 2) This indicates that the patients’ ontological insecurity was negatively correlated with their daily epidemic prevention behavior; that is, the stronger the patients’ ontological security, the more positive the daily epidemic prevention behavior.
Correlation Analysis of Patients’ Ontological Insecurity and Daily Epidemic Prevention Behavior (N = 1185).

P < .001.
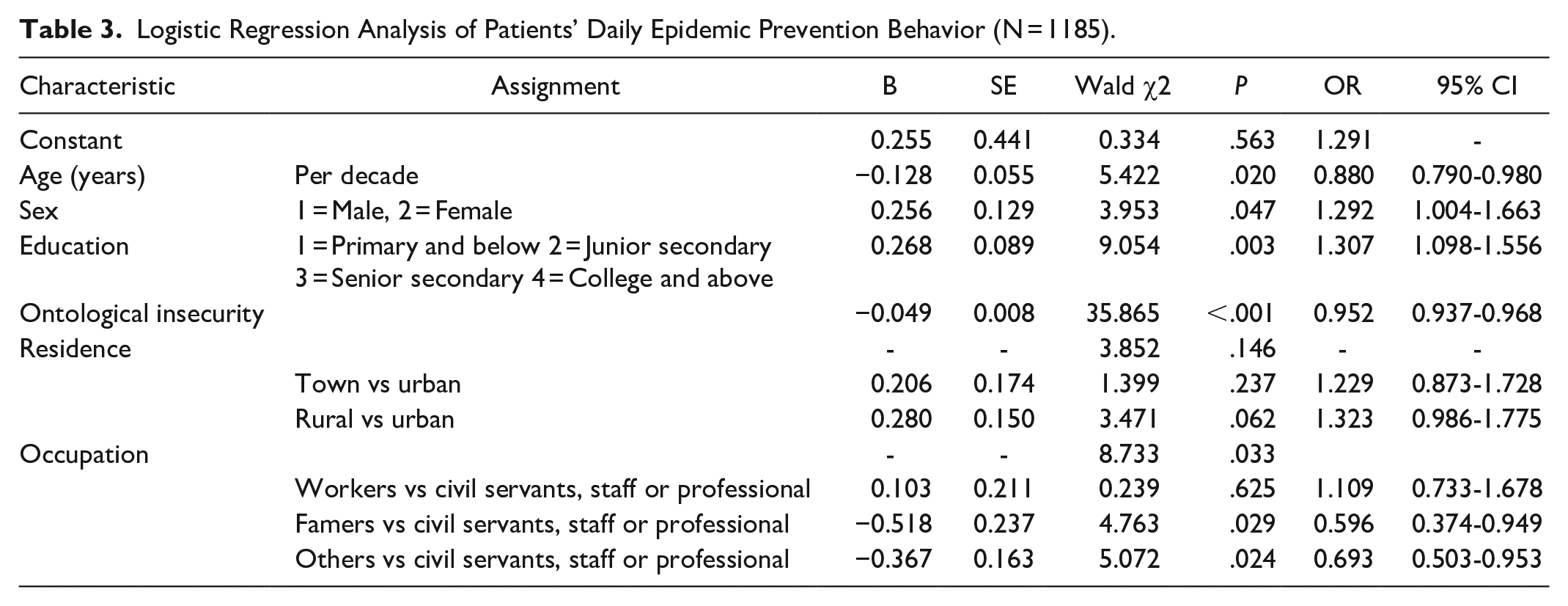
Logistic Regression Analysis of Patients’ Daily Epidemic Prevention Behavior
The logistic regression analysis showed that the independent factors affecting daily epidemic prevention behavior include ontological insecurity (OR: 0.952; 95% CI: 0.937-0.968) (P < .001), sex (OR: 1.292; 95% CI: 1.004-1.663), age (OR: 0.880; 95% CI: 0.790-0.980), education (OR: 1.307; 95% CI: 1.098-1.556), and occupation [famers vs civil servants, staff or professional (OR: 0.596; 95% CI: 0.374-0.949), other vs civil servants, staff, or professional (OR: 0.693; 95% CI: 0.503-0.953)] (P < .05) (Table 3).
Logistic Regression Analysis of Patients’ Daily Epidemic Prevention Behavior (N = 1185).
Discussion
Current Situation of Patients’ Ontological Insecurity and Daily Epidemic Prevention Behavior
Since the start of the COVID-19 pandemic, the Chinese government has actively implemented various public health measures, including urban travel restrictions, self-isolation, maintaining social distance, wearing masks, washing hands frequently, and promoting vaccine acceptance. These measures have been successful in controlling the development of the pandemic.23-25 By June 2021, in the Chinese region where the study was conducted, a total of 149 COVID-19 patients had been cured and discharged with no deaths. 26 In this study, patients came from different wards, such as cardio angiology, gynecology, hematology, neurology, gastroenterology, respirology, and cardiothoracic surgery. No one was hospitalized for COVID-19. According to the National Health Commission requirements, the hospital strictly implemented infection prevention and control measures to be followed by medical institutions during epidemics, such as improving the appointment of diagnosis and treatment, pre inspection and triage, patients wearing masks and successfully performing hand hygiene, restricting the management of accompanying visitors, and successfully performing environmental cleaning and disinfection. 27 The score of patients’ ontological insecurity was 13 (9,18), which is a medium-to-high level. Giesden 28 believes that basic trust is the foundation of establishing ontological security, and the Chinese people trust the government’s ability to control the COVID-19 pandemic and prevent its further development. Studies show that the COVID-19 stress response level decreases with time. 29 At the time of this research, the epidemic situation in China is now under normal management; people have a certain understanding of the disease and have gradually accepted and become accustomed to the changes brought by the epidemic to their daily life and behavior.
Our results also show the score of patients’ daily epidemic prevention behavior to be 63 (51,76). The median score per item for daily epidemic prevention behavior, wearing masks, maintaining social distance, and hand washing were 2.42 (1.96,2.90), 2.67 (2,3), 2.00 (1.53,3.00), and 2.381 (1.85,2.92), respectively. Hospitals should formulate corresponding behavior intervention strategies to improve the level of daily epidemic prevention behaviors and boost publicity and education to address weak links.
Analysis of the Influencing Factors of Patients’ Daily Epidemic Prevention Behaviors
The results of our analysis show that a higher level of education can promote patients’ epidemic prevention behavior (P < .05); the higher an individual’s education level is, the more active their daily epidemic prevention behavior is. This result is consistent with those of Ye et al. 30 Studies show that college-educated individuals have better health habits and higher awareness of self-protection. This tendency may reflect that people with higher education levels are better able to obtain and understand health information, have a firm belief in disease control, and can turn knowledge into practice more readily. 31
Our results also show that age is an obstacle to individual daily epidemic prevention behavior: the older the age, the lower the level of epidemic prevention behavior. This may be related to a lack of epidemic prevention knowledge among older adults. Currently, mobile phone accounts or official WeChat posts, television, and social networking platforms are the main sources of pandemic information. 32 Further, the number of older adults with smartphones and computers or access to social media is far lower than that of young people. The content coverage and information acquisition speed of pandemic prevention and control information obtained through other channels are not as good as when information is obtained through network channels. Moreover, the concepts and thoughts of older adults are set, which means it is much more difficult to change their behaviors than it is to change those of younger people. This suggests that hospitals should strengthen the intervention management related to epidemic prevention behavior among inpatients with low education levels and those who are older.
Research shows that the level of daily epidemic prevention behavior of female patients is higher than that of male patients, while that of civil servants, staff, or professionals is higher than that of farmers and other groups (mainly freelance workers). This may reflect the fact that civil servants, staff, or professionals have relatively fixed work units or organizations and will receive systematic epidemic prevention and control knowledge education and epidemic prevention behavior management. This suggests that the public health administration should strengthen the epidemiological education and behavior warning of ordinary residents. Given all of that, hospitals should implement personalized health education that is based on patients’ characteristics to effectively improve their compliance with daily epidemic prevention behaviors.
The results of this study show that patients with stronger ontological security have a higher level of daily epidemic prevention behavior. Life history theory holds that individuals will show a higher degree of psychological security in a resource-rich living environment and will therefore develop a slow survival strategy; conversely, individuals living in a resource-poor environment will show a low degree of psychological security and develop a fast survival strategy. 33 Individuals with fast survival strategies have been shown to be more likely to violate social norms, be impulsive, and take risks; However, individuals with slow survival strategies are more proficient at following social norms and are often more cautious and conservative. 34 When faced with risk decision-making, individuals who adopt fast survival strategy are relatively short-sighted and aggressive, while individuals who adopt a slow survival strategy pay more attention to long-term impact and behave more cautiously. 35 Risk sensitivity theory states that when facing the gap between reality and the ideal in times of resource shortages, to meet their needs and objectives, individuals choose high-risk projects to narrow this gap. 36 Based on this theory, this study proposes that patients with a weaker sense of ontological security are more likely to suffer from the impact of the pandemic, and their ability to analyze, their judgment, and their logic will be reduced. Their resource shortage mentality will also reduce their cognitive reflection abilities and weaken their impulse control abilities. At this time, patients are more inclined to adopt a fast survival strategy and display risky behavior; that is, patients’ compliance with epidemic prevention behaviors will be reduced, leading to them exposing themselves to a higher-risk environment.
Limitations
This research has certain practical value; however, because of constraints of time and resource factors, there are several limitations. First, this research mainly considered hospitalized patients; nevertheless, the relationship between the ontological insecurity and daily epidemic prevention created by the COVID-19 pandemic might also apply to the public. Further research should consider this selection bias since there might be differences between hospitalized patients and the public. Hence, future research should also consider the public to explore to further investigate the mechanism of the ontological insecurity in people’s infection prevention practices to reduce the spread of the epidemic. Second, patients from different wards, such as cardio angiology, gynecology, hematology, neurology, gastroenterology, respirology, and cardiothoracic surgery, could also affect their perception of COVID-19, and the possible effect of other confounding factors such as income, mental health status, and physical health status, which can also influence pandemic prevention behavior, were also of future consideration. Third, the ontology insecurity scale used in this study was developed by Marlowe et al. In future research, the development of an ontology insecurity scale suitable for local Chinese culture is necessary.
Conclusions
During the current normalization of the COVID-19 pandemic, the ontological security of inpatients is at a medium to a higher level; however, there is still room to improve their daily epidemic prevention behavior. Younger patients, female patients, patients with stronger ontological security, patients with a higher educational level, and those who work in a fixed unit or organization have higher levels of daily epidemic prevention behavior. Hospital managers should strengthen intervention management concerning epidemic prevention behavior based on patients’ characteristics.
Footnotes
Acknowledgements
We would like to thank participants for their cooperation and support.
Author Contributions
Study concept and design: HX Chen, TH Tung
Data collection: WZ Wang, CW Luo, HH Shi
Statistical analysis: HH Shi, MX Zhang, CW Luo
Interpretation of results: HH Shi, WZ Wang
Drafting of manuscript: HH Shi, MX Zhang
Critical revision: HH Shi, WZ Wang, TH Tung
All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper was funded by National Nature Science Foundation of China (Funding ID:72074189).
Ethics Approval
This study was reviewed and approved by the Ethics Committee of Taizhou Hospital of Zhejiang Province (Approval number: K20210521) in China. All procedures were performed in accordance with the guidelines of our institutional ethics committee and adhered to the tenets of the Declaration of Helsinki.
Informed Consent
Informed consent was obtained from all participants.