
Abstract
The outbreak of COVID-19 has had destructive influences on social and economic systems as well as many aspects of human life. In this study, we aimed to estimate the economic effects of COVID-19 at the individual and societal levels during a fiscal year. This cost of illness analysis was used to estimate the economic burden of COVID-19 in Iran. Data of the COVID-19 patients referred to the hospitals affiliated to Bushehr University of Medical Sciences in 2021 were collected through the Hospital Information System (HIS). The study methodology was based upon the human capital approach and bottom-up technique. The COVID-19 pandemic has resulted in 9711 confirmed hospital cases and 717 deaths in Bushehr province during the study period. The direct and indirect costs were estimated to be $1446.06 and $3081.44 per patient. The economic burden for the province and country was estimated to be $43.97 and $2680.88 million. The results showed that the economic burden of this disease particularly premature death costs is remarkably high. Therefore, in order to increase the resiliency of the health system and the stability in service delivery, preventive-oriented strategies have to be more seriously considered by policymakers.
What do we already know about this topic?
The COVID-19 pandemic has quickly affected all economic and social sectors around the world, among which hospitals, as the most crucial pillar of the health system, have been severely influenced by this breathtaking crisis and it seems the continuation of this trend will lead to the severe problems in managing hospitals and other businesses. But the magnitude of this crisis needs to be investigated.
How does your research contribute to the field?
Analysis of the economic burden of the COVID-19 disease could be effective in formulating the required strategies with the aim of increasing the resilience of economic and social sectors, especially hospitals, against such unprecedented crises. In this study, we aimed to estimate the economic effects of COVID-19 at the individual and societal levels during a fiscal year.
What are your research’s implications toward theory, practice, or policy?
Our study findings provide a relatively comprehensive picture of hospitalized COVID-19 patients’ characteristics and also offers valuable insights into hospital and non-hospital cost of COVID-19. Furthermore, considering budget constraints, findings indicate that continuity of this trend would lead to the decreased capacity of the health care system in delivering routine services and in turn higher out-of-pocket payments and even more mortality and finally increased economic burden.in conclusion, to increase the resiliency of the health system against these kinds of unprecedented crises we need to put preventive measures in the priority which are dominantly more cost-effective strategies than therapeutic actions. Otherwise, health systems may face collapse.
Introduction
Corona virus disease or simply COVID-19 is an infectious disease which was firstly found as an epidemic on December 31, 2019, in Wuhan, China.1,2 This disease quickly spread across the world as the World Health Organization (WHO) on March 11, 2020, declared it as a pandemic. 3 The patients catching this virus manifest a various spectrum of symptoms from a mild fever to acute respiratory failure, also thromboembolic diseases, and dysfunction or failure of several organs. 4 People with underlying diseases like cardiovascular disease, diabetes, chronic respiratory disease, and cancer are more likely to develop serious illnesses. 5 In rare cases, cardiac and cerebral problems have been reported in studies as well. 6 By October 29, 2021, this fatal disease has infected more than 245 373 039 million people and nearly 4 979 421 million have died as the result of the disease. 7
In Iran, the first case of the disease was reported on February 19, 2020. 8 Since then, various measures have been implemented to prevent and control the disease. 9 Formulating health protocols for different job groups, insisting on social distancing, wearing a face mask, and temporary and classified closure of jobs with regard to the incidence rate of the disease in the affected geographic areas have been a number of these policy actions. 10 Among the organizations involved with COVID-19, hospitals as the front line of fighting against COVID-19 are considered to be the heart of the organizations that suffered the most from this highly contagious disease. 11 In addition to the direct costs imposed on hospitals due to COVID-19, most of the public hospitals were forced to cancel the routine elective surgeries to effectively cope with the invasion of this virus. 12 The economic burden of COVID-19 exceeds the direct medical costs and extends to the indirect costs, especially premature deaths costs and costs of absenteeism.13-15 Lost productivity arisen from the premature death with regard to the fatality rate of COVID-19 16 and conducted studies about premature deaths rate 17 is estimated to be high.
The calculation of the economic burden of the disease has been regarded in several studies.6,18,19 But given the fact that different settings will have distinguished consequences, determining the economic burden of COVID- 19 in the studied environment is of great importance.
According to the report of Iranian health authorities, there have been 125 223 COVID-19 deaths in Iran with more than 5 860 844 Confirmed cases until October 25, 2021. 20 Bushehr province with 1 465 000 population 21 is located in the southwest of Iran and coincident with the COVID-19 outbreak has been subjected to this disease, but no study has been conducted to determine the economic burden of COVID-19 in the province yet. As a result, this study aimed to demonstrate a relatively comprehensive picture of costs imposed from the societal perspective in the province and finally estimation of its economic burden in Iran.
Materials and Methods
Study Design and Population
This is an applied and cross-sectional research conducted using a partial economic evaluation method on which cost outcomes are described.
The research population included all the patients hospitalized with COVID-19 who had referred to all hospitals affiliated to Bushehr University of Medical Sciences, as referral centers of COVID-19 in Bushehr province, in 2021. No sampling was performed since all patients were included in the study.
Data Source
The required data were collected through the hospital information system (HIS) database. The HIS is a large and comprehensive database at the hospital level in Iran encompassing all services and associated costs of patients admitted in hospitals. The information available in the HIS are qualitatively assured because they have been confirmed by third payers (insurers). Societal perspective was applied to estimate all costs including direct and indirect costs. Data elements included the patient’s demographic information, hospital costs, and discharge status (recovery or death).
Direct Health-Care Costs Per Patient
Data recorded in the HIS database were used to calculate direct medical costs. Data were categorized as follows: hospitalization cost, drugs cost, intensive care unit (ICU) cost, and other (laboratory, imaging, nursing, and visit) costs.
In order to calculate the average direct cost per patient, the total costs incurred hospitals on COVID-19 patients were divided by the number of COVID-19 patients.
Cost per patient = total hospital costs for COVID-19 patients/number of COVID-19 patients
Indirect Costs Per Patient
To estimate indirect costs, human capital approach was used. Indirect costs were put into 2 main categories. The first one included the cost of production lost due to hospitalization and rest at home and finally, absence at work, and the second one was lost productivity as a result of premature death at the ages of 15 to 65. Due to the fact that individuals under 15 and over 65 are not economically productive, their lost productivity was considered zero.
In order to calculate the average cost of hospitalization per patient in the hospital, the Average days of hospitalization was multiplied by the average daily wage of patients at ages 15 to 65. In addition, to calculate the average cost owing to rest at home, days of home rehabilitation were determined based on experts’ opinions (14 days) and then multiplied by the average wage of patients 15 to 65 years old. Considering that access to the average daily wage of patients was not possible, the minimum daily wage determined by Iran’s labor office was replaced. 22 In order to calculate the cost of production lost due to premature death, a growth rate of 3% and a discount rate of 6% was considered. 19
Furthermore, The Forgone Labor Output (FLO) equation was used to estimate the potentially lost productivity due to the premature deaths:

In this equation w is the minimum wage lost per person per year, G is the annual growth rate, r is the discount rate, i is the number of years of life lost, and p is the current value of the predicted future income per workforce. 23
Economic Burden
To estimate total economic burden of COVID-19 in the province, a bottom-up approach was used. Accordingly: firstly, direct cost per patient was multiplied by the number of hospitalized patients. Secondly, the average indirect cost due to hospitalization in hospital and rest at home was multiplied by the number of patients 15 to 65 thirdly, the average indirect cost due to premature death per patient was multiplied by the number of dead patients 15 to 65 and finally, the obtained results were added together. 24
Accordingly, the economic burden will be estimated as follows:
Where ix is the number of affected patients and px is the unit cost at the patient level and C is the overall cost. 24
All costs were calculated in Iran’s Rial at 2020 value and then converted to purchasing power parity (PPP) 2020, adjusted by, equivalent to 31 317 Rials per 1 dollar. 25
Statistical Analyses
Descriptive statistics were utilized to summarize data and in this line demographic and hospitalization attributions such as insurance status, gender, age, place of residence, average length of stay, discharge condition (death/recovery), average direct and indirect costs, and total cost of major costing groups (ICU, drugs, and hospitalization cost) were examined. Frequencies and percentages were reported for categorical variables and continuous variables were summarized using means and standard deviations (SD).
Sensitivity analysis
Since indirect costs estimation was done based on the minimum daily wage, constant discount rate, and also full employment of 15 to 65 age group, a sensitivity analysis was undertaken to elevate the power of the study. In this regard, different discount rates (ranging from −20 to +20) and different wages (minimum and maximum wages paid by the labor department) were determined to get the best and the worst scenarios.
In addition, due to the possibility of changes in direct costs that are mostly influenced by different treatment methods, a positive and negative range of 20% was used to minimize the possible error. As a result, the best and worst economic burden scenarios for Bushehr province and Iran were calculated.
Results
Demographic and Hospitalization Findings of the Study Population
9711 hospitalized COVID-19 patients were identified in 2021 using HIS database. Table 1 presents the demographic and hospitalization characteristics of studied cases.
Demographic Characteristics of COVID-19 Patients Studied in 2021 (N = 9711).
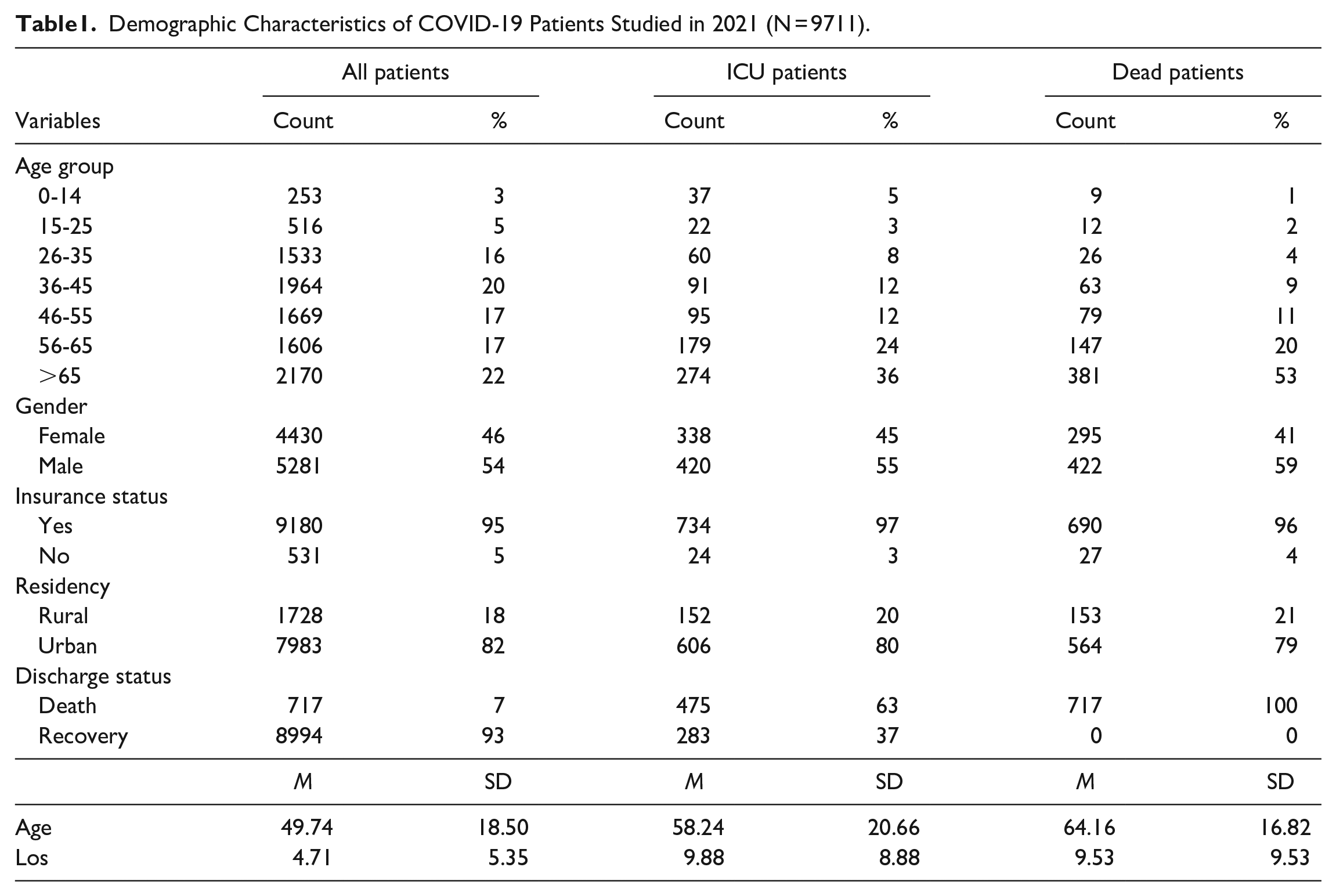
The mean age of the hospitalized COVID-19 patients was 49.7 ± 18.50 years. A 3% of the patients were under 15 years old, 75% were 15 to 65 years old, and 22% were 65 years or higher. On average, the length of stay (LOS) per patient was 4.71 days and the same indicator among the ICU patients was 9.88 days.
A 54% of the hospitalized COVID-19 cases were male and approximately the same percentage of ICU COVID-19 patients were male as such almost three-fifths of dead COVID-19 patients were male. Of hospitalized cases, 95% were insured and 82% of whom were residents of urban areas. Overall, 7% of hospitalized COVID-19 patients died while the death rate of ICU patients was 63%.
Direct Medical Costs
Given the results, the total direct cost was calculated to be $14 042 669 and in turn, the average direct cost was $1446.06 per patient (Table 2).
Major Components of Direct Costs of Hospitalized COVID-19 Patients in 2021.

Findings also showed that the largest share of direct costs belonged to the in-patient beds cost and drugs with 36.44% and 30.80% equivalent to $5 116 984 ($526.93 per patient) and and 4 324 777($445.35 per patient ) respectively.
Fallowing that, ICU costs accounted for 26.88% of total direct costs. all in all, the 3 major cost groups mentioned above constituted approximately 95% of total direct costs (Table 2).
Indirect Costs
Lost Productivity Due to Hospitalization
To estimate indirect costs of hospitalized patients, the average length of stay (LOS) of 15- to 65-year-old patients (4.5 days) was multiplied by the minimum daily wage ($20.34). Consequently, indirect cost per patient was estimated to be $91.50 PPP.
Lost Productivity Due to Convalescence Period
Production loss owing to the recovery period at home was estimated through multiplying with average days of Convalescence period (14 days) in the minimum daily wage of recovered patients 15 to 65 years old and it was calculated $284.68 PPP.
Lost Productivity Due to Premature Death
To calculate average years of lost life (YLL), the average age of dead patients (52 years) was subtracted from the maximum productivity age (65 years) and as a result, YLL calculated 13 years. Given the fact that the salary of dead patients was not available, the minimum salary determined by the Iran Labor Organization (ILO) in 2020 was utilized. It was calculated $7799.32 per year for a dead patient. Finally using the previously mentioned formula in methodology, lost productivity for all dead patients in productive age (327 patients) was estimated as follows (Table 3).
Indirect Cost (Lost Income Due to. . .) of Hospitalized COVID-19 Patients (PPP $) in 2021.

P = 83 410.82 × 327 = $27 275 339.07 PPP
Economic Burden
Economic burden was estimated according to the equation mentioned in the methodology. As a result, economic burden = (direct cost per patient × the number of hospitalized COVID-19 patients) + (the number of patients 15-65 × average indirect cost due to absence at work) + (the number of dead patients 15-65 × average indirect cost due to premature death).
C = (1446.06 × 9711) + (91.50 × 7288) + (284.68 × 6961) + (83 410.82 × 327) = $43.97 million PPP.
The results also indicate that direct costs account for 32% of total economic burden. In other words, more than two-third of total economic burden belonged to the indirect costs (Figure 1).

Percentage of direct and indirect costs based on each age group in 2021.
In line with the proportion of Bushehr to Iran population (1.64%), the Economic burden imposed by COVID 19 on the country during the studied period would be $2680.88 million PPP.
Sensitivity Analysis
Since the estimated indirect burden is sensitive to the average daily wage and discount rate, a sensitivity analysis considering different w and r was performed to increase the robustness of the results (Table 4). Furthermore, with regard to the probability of some changes in direct costs that are mostly affected by treatment protocols, they were calculated in a certain range from + 20% to − 20%. Accordingly, the total economic burden for Bushehr province and Iran would fluctuate between ($39.47 and $205.20 million) and ($2406.71 and $12 512.20 million) respectively.
Sensitivity Analyses for Indirect Costs of COVID-19 Patients (PPP $) in 2021.

Discussion
This is the first study dealing with the economic burden of COVID-19 in Bushehr province. Calculation of economic burden is of considerable importance especially when the outbreak of disease is high and countries severely face financial resources constraints and could help formulate appropriate strategies adopted by policymakers.
In this retrospective study, 9711 hospitalized COVID-19 patients were identified in 2021 of whom 54% were male and 22.3% were X ≥ 65 which is approximately consistent with those described by Ghaffari Darab et al 18 Yet the percentage of affected females in Maltezou et al 19 study was higher (71%) compared to that obtained in the current study which is probably dependent on the studied setting where only health care workers were examined. The mean age was 49.7±18.5 which is lower than Jeck et al 26 as well as Di Fusco et al 6 studies and higher than that mentioned in Maltezou et al 18 study. One of the main reasons attributed to this difference is the high proportion of the young population in the researched province. 21 But since the examined sample in the Maltezou et al 18 study were health workers; the average age was naturally lower. The current study highlighted 95% of patients were insured which is nearly close to the reported percentage (4.5% in Di in Fusco et al 6 study) but from the perspective of the hospital population served, the result was different as the proportion of the rural population in our study was higher (18 against 10.5%).
In-hospital mortality in the current study was 7%. This proportion among the admitted patients in ICU increased to 63%. The in-hospital mortality rate observed in this study to some extent was higher than what was reported in the Jin et al 27 study, but in comparison to Di Fusco et al 6 study, the mortality rate in our study was roughly 50% lower (13.6% against 7%). Observed lower mortality rate could be attributed to the different treatment protocols and ease of access to treatments and also other appropriate strategies adopted by health ministry such as Equipping hospitals with oxygen generators and increased the hospital beds and canceling non-emergency surgeries.
Examining average LOS showed that this indicator for the whole patients was 4.71 days which is lower than the figures reported in Ghaffari Darab et al, 19 Di Fusco et al, 6 Maltezou et al, 18 and Jeck et al 26 studies (7, 8.3, 7.3, and 16.4 days) respectively and nearly doubled (9.88 days) for the hospitalized patients in ICU ward Which is slightly different from the figure reported in Di Fusco et al 6 study. Discretion of physicians and also customized clinical guidelines could be the main drivers of this difference.
The average direct medical cost per patient in hospitals affiliated to Bushehr University of Medical Sciences was estimated to be $1446.06. While reported direct medical cost per patient in another study conducted in Iran was $3755. 19 In addition, 2 conducted studies by Di Fusco et al 6 and Bartsch et al 28 in the United States revealed that on average, the direct cost of COVID-19 per patient has been $3045 and $24 571, respectively. The average longer length of stay, as well as different treatment processes in these studies, are the main drivers attributed to the higher cost.
Results highlighted that although 7% of COVID-19 patients received ICU services, however, the share of these patients from the total cost imposed on hospitals was 26%. Indeed, on average, the cost of ICU patients was 3.4 times that of other patients ($4979.83 against $1446.06), meanwhile, the average cost of ICU patients in the study conducted by Ghaffari Darab et al 19 and also Di Fusco et al 6 was estimated to be $13 267 and $25 688, respectively. This difference in costs could have resulted from underlying conditions of hospitalized patients, different clinical guidelines, physicians’ discretion, and in turn the volume of delivered services, and finally, some differences in service unit cost. Drug cost groups along with hospitalization and ICU cost groups were 3 main components of hospital direct costs as almost 90% of hospital costs belonged to these 3 groups.
In addition to direct medical costs which are a proxy of the costs incurred by hospitals, the economic burden of the COVID-19 outbreak exceeds it and the societal cost of COVID-19 greatly outweighs the medical costs. Findings showed that only productivity losses due to premature death per patient were $83 410.82 that in comparison with average direct medical costs is 58 times. The average indirect cost owing to premature death is nearly close to the estimated amount in another study conducted in Iran. 19 Societal costs will exceed this amount when the lost productivity due to hospitalization and recovery course is considered as well. These figures for hospitalization as well as recovery course are $91.50 and $284.68 per patient, respectively.
According to the findings of the study, economic burden of COVID-19 in Bushehr province is estimated to be $43.97 million ($39.47 and $205.20 million) that 32% out of this constitute direct medical costs. In another word, the share of societal or indirect costs is more than twofold. Considering that Busher’s population is 1.64% of country one, 21 the economic burden of COVID-19 for Iran is estimated to be $2680.88 million ($2406.71 and $12 512.20 million) during the study period which is equivalent to 0.20% Iran’s Gross Domestic Product (GDP) in 2020 29 which in comparison with the results of another study undertaken in Iran is higher. 19
Since the estimated economic burden is influenced by minimum daily wage and also the discount rate, therefore a sensitivity analysis was undertaken to enhance the power of the study. Accordingly, findings indicate that economic consequences of COVID-19 disease at the least estimation are considerably high and increased prevalence will definitely lead to the rise of a tremendous economic burden. Consequently, the health care system and society will be undergone more challenges.
Conclusions
Our study findings provide a relatively comprehensive picture of hospitalized COVID-19 patients’ characteristics and also offers valuable insights into hospital and non-hospital cost of COVID-19. Furthermore, considering budget constraints, findings indicate that continuity of this trend would lead to the decreased capacity of the health care system in delivering routine services and in turn higher out-of-pocket payments and even more mortality and finally increased economic burden.in conclusion, to increase the resiliency of the health system against these kinds of unprecedented crises we need to put preventive measures in the priority which are dominantly more cost-effective strategies than therapeutic actions. Otherwise, health systems may face collapse.
Limitations
The findings of this study should be interpreted in the contexts of several limitations. In the present study, due to the lack of access to patients’ income, the minimum wage was used to calculate indirect costs. Therefore, the economic burden may be underestimated. In addition, in this study only hospitals affiliated to Bushehr University of Medical Sciences were included therefore, generalizability should be done with caution.
Footnotes
Acknowledgements
We hereby thank all the staff of Bushehr University of Medical Sciences for their generous help in conducting this study.
Authors Contributions
Ma.R: Conceptualization, Data curation, Supervision, Validation, Writing—review & editing, Methodology, Software, Roles/Writing—original draft. Me.R.: Conceptualization, Data curation, Supervision, Validation, Writing—review & editing. H.O.: Conceptualization, Data curation, Methodology, Software, Project administration, Investigation, Supervision, Validation, Writing—review & editing, Roles/Writing—original draft. A.Kh.: Conceptualization, Data curation, Methodology, Methodology Supervision, Validation, Writing—review & editing.
S.K.: Conceptualization, Data curation, Methodology, Methodology Supervision, Validation, Writing—review & editing. H.Gh.: Data curation, Methodology, Software, Validation, Writing—review & editing. A.P.: Conceptualization, Data curation, Methodology, Methodology Supervision, Validation, Writing—review & editing.
Availability of Data and Materials
The datasets generated and analyzed during the current study are not publicly available because they contain information that could compromise the privacy of research participants, but are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Consent to Participate
All data are collected and handled in accordance with the relevant privacy protection guidelines. According to Iran law, the study did not fall under the remit of the Medical Research Involving Human Subjects because the design of the study was secondary data analysis, written consent was not necessary but the ethics code was received from Bushehr University of Medical Sciences.
Consent for Publication
All participants completed a consent form, stating that they were well-informed about the content of questionnaires and that they agreed upon the publication of anonymized data.