
Abstract
Gaps between medical needs and health services accessibility are defined as unmet medical needs (UMN). Previous studies assessing UMNs during the coronavirus disease 2019 (COVID-19) pandemic did not account for factors such as the type of medical insurance or chronic disease. Therefore, this study investigated various factors, including medical insurance and chronic diseases, affecting self-reported UMN during the pandemic in Daejeon Metropolitan City, South Korea. This cross-sectional study was conducted using Daejeon Metropolitan City Health Surveys data from 2020. The weighted prevalence of UMN was estimated among participants (n = 1494) aged ≥18 years, while chi-squared and logistic models were used to assess the association between UMN and participant characteristics. The prevalence of UMN was 6.4% (n = 97). Female sex and low education levels were significantly associated with reporting UMN. Medical aid beneficiaries were less likely to report UMN than adults with National Health Programs coverage. Participants with chronic diseases, such as hypertension and arthritis, and those with depression, were more likely to report UMN than adults without these conditions. The findings highlight the need for targeted efforts to decrease UMN in the COVID-19 pandemic, especially for women and individuals with low education levels. The results also indicate that high-risk disease groups should be targeted with additional enabling services to support the management of chronic conditions.
A previous study showed sex, age, education level, occupational cluster, chronic diseases, and mental health to be significantly associated with unmet medical needs during the COVID-19 pandemic.
To our knowledge, there is no evidence that various factors including medical insurance and chronic disease types are associated with a high risk of unmet medical needs during the pandemic.
The research highlights the necessity of efforts aimed at reducing unmet medical needs among high-risk groups.
Introduction
Coronavirus disease 2019 (COVID-19) is an infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).1,2 It rapidly spread worldwide, and on March 11, 2020, the World Health Organization declared it a pandemic. 3 The virus has continued to spread, and as of November 5, 2021, the total number of confirmed cases worldwide was 249.58 million while the number of deaths caused by COVID-19 was 5.04 million. 4 SARS-CoV-2 is transmitted via droplets, 5 and many countries have developed strategies to try and reduce this. 6 Social distancing measures aim to prevent droplet spread and policies regulating social activities were widely implemented, such as avoiding or reducing physical interactions and wearing masks.7-9 However, these policies can isolate people and may lead to additional negative social consequences. 10 In the context of healthcare-seeking behavior, people adhering to social distancing policies are not motivated to visit crowded places, which may discourage them from visiting medical services even when they are sick.
In Korea, the initial outbreak of SARS-CoV-2 led to a significant reduction in the number of hospitalizations and outpatient visits. 11 Thus, the pandemic and social distancing policies appeared to limit access to medical services. Gaps between medical needs and access to care are defined as unmet medical needs (UMN). 12 Before the pandemic, the common causes of UMN were the burden of treatment costs, absence of medical institutions nearby, mild symptoms, no time to visit, and difficulties in getting an appointment. Therefore, many surveys followed these standards and used them as an index to evaluate the effectiveness of a country’s healthcare delivery system. 13 However, the pandemic has emerged as a new and major cause of UMN. Therefore, UMN require further characterization in the era of COVID-19. A recent study identified sex, age, education level, occupational cluster, chronic diseases, and mental health to be significantly associated with UMN during the early stage of the COVID-19 pandemic in Seoul, South Korea. 9 However, this study had limitations, since it did not consider the types of medical insurance, a key determinant of UMN, and the types of chronic diseases. 9
Daejeon metropolitan city (hereafter, Daejeon) is a provincial city in Korea with a population of 1.48 million as of 2020, 14 with 15.2% of residents being elderly. 15 An aging population is associated with a higher prevalence of chronic conditions, and in 2020, the prevalence of hypertension and diabetes in Daejeon were 18.6% 16 and 7.1%, 17 respectively. As these conditions require continuous treatment and management, the Korean government launched chronic disease management projects before the pandemic. 18 Community primary medical institutions and public health centers in Daejeon were in charge of continuous health monitoring, health education, exercise, and dietary management for the residents. However, the Korean government reorganized the functions of the community’s primary medical institutions and public health centers to respond to the pandemic by serving as COVID-19 screening clinics and managing COVID-19 patients. These changes, inevitably, resulted in UMN in residents with chronic conditions. This study aimed to determine the prevalence of self-reported UMN among adults during the COVID-19 pandemic in Daejeon, South Korea, and investigate the relationships of UMN with individual demographic characteristics, financial resources, and health-related factors.
Methods
Data Source and Study Population
We used data from the Daejeon Metropolitan City Health Survey, a cross-sectional survey conducted by the Daejeon Metropolitan City Public Health Policy Institute from 19 August to 29 September 2020, when the second wave of COVID-19 commenced and the government enforced strict social distancing. To represent the entire population of Daejeon, the survey used proportionate quota random sampling accounting for sex and age across 5 districts in Daejeon and selected participants. A total of 2013 people were invited, and 1500 completed the survey. The questionnaire was completed using face-to-face interviews conducted by trained interviewers. The survey had a margin of error of ±2.2%, and a P-value of .05 at 95% confidence level. Questions included physical, mental, and social health status, medical service usage, the impact of COVID-19 on health and daily life, and socioeconomic factors. Of the 1500 participants, we excluded 6 whose responses to the socioeconomic factors were missing, leaving 1494 for analysis. This study was granted an exemption by the Institutional Review Board of the National Bioethics Committee, Seoul, Korea (P01-202203-01-015). All participants provided written informed consent before completing the questionnaire.
Measurements
Our primary outcome variable was a binary variable indicating self-reported UMN due to COVID-19. In the Daejeon Metropolitan City Health Survey, participants were asked the question, “Since the outbreak of COVID-19, have you ever experienced unmet medical needs caused by COVID-19?” Answers were coded as yes/no and scored as 1/0. We selected independent variables based on the conceptual framework of Andersen and Newman’s 19 Behavioral Model for Health Services Use, which is intended to explain contextual and individual factors (including predisposing characteristics such as sex, age, education level, employment status, and enabling resources, such as income and health insurance type). To measure the need for health services, we included self-reported chronic diseases and general health status. Specifically, we used variables for sex (1: male, 2: female), age group (1: <65 years, 2: ≥65 years), and the highest level of education (1: college or above, 2: high school, 3: below middle school). Monthly income was classified as ≥5000 USD, 3340-4999 USD, 1670-3339 USD, and <1670 USD, and the type of health insurance was classified as National Health Insurance (NHI) or Medical Aid (MA). We specifically selected 5 chronic diseases associated with health service use: hypertension, diabetes, dyslipidemia, cerebrovascular disease, and arthritis. To analyze the participants’ chronic diseases, we used the following question: “Are you currently receiving treatment for chronic diseases?” Answers to this were coded as yes/no, and scored as 1/0. Health status indicators included self-rated health status (coded as 1: good, 2: moderate, and 3: poor), and depression over the past 2 weeks (coded as 1: no and 2: yes).
Statistical Analysis
Weighted descriptive statistics of participant characteristics were reported. The prevalence of UMN for the entire sample and in each district in Daejeon were estimated. Next, we determined bivariate relationships between the binary indicator of UMN and each independent variable (participants’ predisposing factors, enabling resources, and need for health services) by using chi-squared tests. We further calculated the odds ratios (OR) and 95% confidence intervals (CI) of the effects of each independent variable included in the multivariate logistic regression model. All data were analyzed using Stata SE, Version 17 (StataCorp LP, College Station, Texas). We considered P-values <.05 to be statistically significant.
Results
A total of 1494 adults (aged ≥18 years) were included, of whom 50.3% were female, 85.2% were aged <65 years, 46.6% had a college or higher degree, 38% were permanent workers, >70% reported monthly incomes between 1670 and 4999 USD, and 95.7% were NHI beneficiaries (Table 1). In addition, 72.3% of the participants had good health status while 65.0% experienced depression during the previous 2 weeks. In the assessment of chronic diseases, 13.3% of the participants had hypertension, 6.3% diabetes, 5.7% dyslipidemia, 1.9% arthritis, and 1.2% cerebrovascular diseases.
Characteristics of Adult Participants in Daejeon Metropolitan City, South Korea (n = 1494).

Note. $1 USD = ₩1180 won in 2020.
Overall, 6.4% of the participants (n = 97) had UMN due to COVID-19 in Daejeon. The highest rate of UMN (10.7%) was reported in the district of Seo-gu, followed by Jung-gu (7.6%), Yuseong-gu (4.3%), Daedeok-gu (3.0%), and Dong-gu (2.4%) (Figure 1).
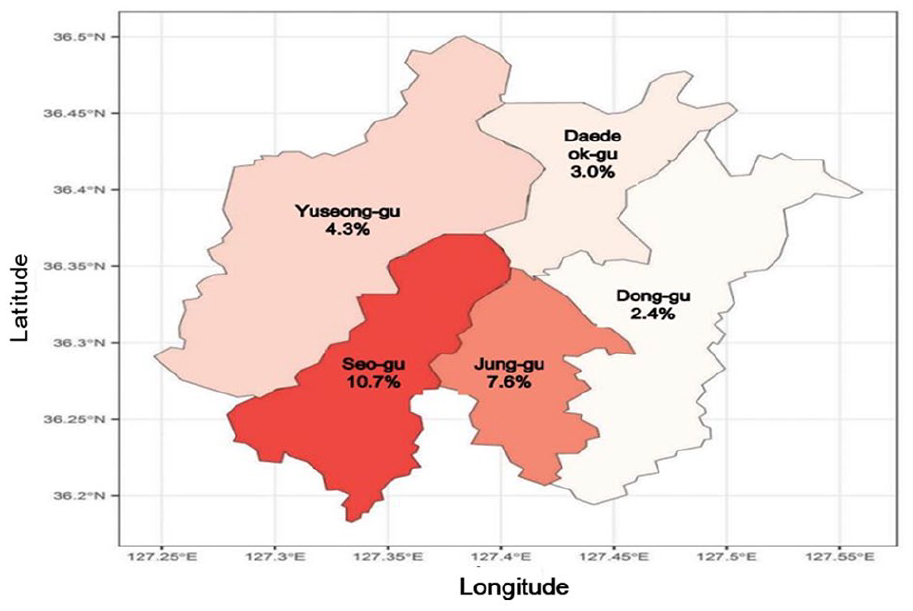
Unmet Medical Needs Due to COVID-19 by Districts in Daejeon Metropolitan City.
Table 2 shows bivariate relationships between self-reported UMN due to COVID-19 and individual-level predisposing factors, enabling resources, and needs. Participants aged ≥65 years, females, those with low educational attainment and low incomes, and economically inactive participants reported high rates of UMN caused by COVID-19 (P < .01). Participants with poor health conditions, depression, dyslipidemia, and arthritis also had high rates of UMN (P < .01).
Unmet Medical Needs Due to COVID-19 in Relation to Participant Characteristics.

Note. $1 USD = ₩1180 won in 2020.
Table 3 shows the estimation of the effects of each independent variable on UMN due to COVID-19. Female participants were 1.60 times (95% CI = 1.01-2.55) more likely to report UMN than males. Participants with only middle school education were 2.29 times (95% CI = 1.02-5.14) more likely to report UMN than adults with high education. MA beneficiaries were 0.24 times (95% CI = 0.03-0.87) less likely to report UMN than NHI beneficiaries. Adults who reported experiencing depression were 2.24 times (95% CI = 1.22-4.11) more likely to report UMN than adults who did not experience depression. Adults with hypertension (OR = 1.94; 95% CI = 1.02-3.68) and arthritis (OR = 6.22; 95% CI = 2.35-16.48) also showed a significantly greater likelihood of experiencing UMN than the participants who did not report these diseases.
Factors Associated With Unmet Medical Needs Due to COVID-19.

Note. $1 USD = ₩1180 won in 2020.
CI = confidence interval.
Discussion
This is the first study to identify the prevalence of UMN and associated factors during the pandemic in Daejeon, South Korea. We sought to determine the factors associated with UMN caused by COVID-19 and applied them to the Andersen and Newman framework. 19 The findings indicated significant associations of predisposing factors (female sex and low educational attainment), enabling resources (MA), and needs (presence of depression, hypertension, and arthritis) with UMN as a result of the pandemic.
Women were more vulnerable to UMN. Previous studies have shown that women report higher rates of UMN than men,20,21 as they experience biological events, such as menstruation and pregnancy, and also subjectively have greater medical needs because they are more sensitive to, and interested in, health than men. 21 Our findings suggest a similar response among women to UMN during the COVID-19 pandemic in Daejeon. Kim et al 9 argued that women are more likely to avoid hospital visits or react sensitively to infection concerns because they are vulnerable to stress.
A lower level of educational attainment was associated with an increased likelihood of experiencing UMN, similar to a recent study. 9 This may be because adults with low educational attainment show negative attitudes toward health and treatment, or are less likely to be aware of the avenues for getting essential or recommended care. 22 In addition, a low educational level is related to low health literacy, which increases UMN. 23 Individuals with low levels of health literacy may experience greater fears while attempting to access care when they need it. In addition, media platforms continuously report on COVID-19 cases and deaths, fueling fear, and preventing patients from seeking health care.
An unexpected finding was that MA recipients were less likely to report UMN during the pandemic than those using health insurance. These results are inconsistent with previous studies that reported economic hardship to be the primary concern among adults, particularly MA recipients.24,25 MA is a government-funded system for providing healthcare benefits for low-income families who cannot pay the premium to NHI but desperately need medical care. Consequently, the UMNs of certain economically vulnerable groups are significantly more affected by finances such as income; therefore, there is a high probability of high rates of UMN before the pandemic but not during the pandemic.
Depression is known to be an essential risk factor for the development of UMN even before COVID-19.20,26 Cho et al 27 argue that self-perception of health status is overwhelmingly negative when individuals suffer from depression or anxiety. They also suggest that depression causes somatization, making diagnosis and treatment difficult. Therefore, we hypothesized that these factors could result in UMN. More recently, the emergence of social anxiety related to COVID-19, and the government’s control of social activities in senior citizens’ centers, schools, places of religion, restaurants, cafes, and sports facilities has increased the symptoms of depression, a phenomenon that has become known as the “corona blues.”28,29
Individuals with hypertension showed a significantly greater likelihood of UMN due to COVID-19. Hypertension is considered milder than other diseases, such as cancer, cardiovascular disease, and cerebrovascular disease, and can be prevented and reversed. 30 However, hypertension requires access to medications, exercise, and diet control, all of which were limited by COVID-19-related restrictions. Exercise opportunities were limited by restrictions on gym and swimming pool usage as a part of the social distancing campaigns. Similarly, getting prescriptions for treatments or medications became difficult due to the restrictions on visits to crowded places, including healthcare institutions, which led to greater UMN. In response to COVID-19, the Korean government differentiated access to medical care according to the patient’s disease, securing accessibility for those with severe illnesses, and allowing telemedical consultations as well as prescriptions for those with mild chronic diseases, such as hypertension and diabetes.31,32 Therefore, UMN could be reduced among patients with hypertension through the continued use of telemedicine.
Interestingly, individuals with arthritis showed the greatest likelihood of UMN. Arthritis is defined as the presence of swelling of the joint, or 2 or more of the following conditions: limitation of motion, tenderness, pain with motion, or joint warmth. 33 In the report by Jung 34 describing the UMN experience rate among chronic patients before COVID-19, arthritis patients showed the highest UMN experience rate (25.2%) in comparison with patients reporting other diseases such as diabetes (17.4%), hypertension (20.1%), high dyslipidemia (23.9%), asthma (19.4%), stroke (21.6%), and cancer (16.3%). Our findings revealed that the UMN experience rate among patients with arthritis in the era of COVID-19 was 38.2%, much higher than that before COVID-19. 34 The social distancing campaigns to limit the spread of COVID-19 may have limited social and physical activity, making patients unable to exercise and worsening their arthritis. Moreover, people may have avoided using medical services to reduce the risk of being infected with COVID-19, which can lead to UMN. The promotion of physical activity is a good measure to prevent arthritis and may reduce UMN. Therefore, the city of Daejeon should conduct an education and training project on daily management and exercise methods for the elderly in response to the COVID-19 pandemic, which could include facilities such as an aerobic gymnastics program with people spaced 5 m apart in outdoor spaces.
This study had some limitations. First, the self-reported data may have included biases and measurement errors. Second, causality cannot be assumed because it was a cross-sectional study design. Third, although the pandemic has been affecting Daejeon since early 2020, this study only investigated the findings from August 1, 2020, to September 23, 2020; therefore, we could not perform a time-series analysis. Fourth, the study focused only on Daejeon, a provincial city in Korea, and the results may not be generalizable to the entire country. Therefore, we suggest that further research should conduct in other similar metropolitan areas and compare the results with this study.
This study analyzed the factors affecting UMN during the COVID-19 pandemic, focusing on Daejeon, Korea. Our findings could contribute to the rethinking of healthcare systems, especially those in provincial cities, and their response during the current, and any future, pandemics.
Footnotes
Acknowledgements
None
Author Contributions
Conceptualization: HyunWoo Jung, Xianhua Che; Data curation: Xianhua Che; Formal analysis: Xianhua Che; Methodology: HyunWoo Jung, Xianhua Che, Hee-Jung Park; Writing—original draft: HyunWoo Jung, Xianhua Che, Hee-Jung Park. All authors have read and agreed to the published version of the manuscript.
Data Availability
The data that support the findings of this study are available from Daejeon Metropolitan City Public Health Policy Institute but restrictions apply to the availability of these data, which were used under license for the current study, and so are not publicly available. Data are however available for the authors upon reasonable request and with permission of Daejeon Metropolitan City Public Health Policy Institute.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study was granted an exemption by the Institutional Review Board of the National Bioethics Committee, Seoul, Korea (P01-202203-01-015).
Informed Consent
All participants provided written informed consent in advance of the examination, and original data accessible to the public were used in this study.