
Abstract
Continuous nursing education has a significant correlation with increasing knowledge, improving skills, and personal preparedness for disasters among nurses which leads to a decrease in mortality rate and enhances the quality of care. However, there is limited literature evaluating the effect of educational programs on the knowledge, skills, and personal preparedness for disaster preparedness among emergency nurses at Arab countries including, Jordan. This study evaluated the effect of an educational program on knowledge, skills, and personal preparedness for disasters among emergency nurses. A quasi-experimental study and one-group pretest-posttest design was used. A convenience sample was adopted to recruit registered nurses who are working in emergency rooms in the private and government health sectors in Jordan (N = 50). This study was conducted between May and June 2021. The intervention included an educational program consisting of 5 topics about disasters. The participants attended this program for 8 h over 1 week via Zoom application. There were significant differences between the pre-post educational intervention for knowledge (t = 4.79, P ≤ .001), skills (t = 6.66, P ≤ .001), and personal preparedness (t = 9.56, P ≤ .001) for disasters. These findings suggested the importance of implementing continuous education and training programs for emergency nurses about disasters due to increasing frequency of disasters worldwide.
Nurses are the major group of the healthcare staff that have a direct contact with disaster victims, they play a significant role in minimizing the influence of these crisis. Thus, they need to improve their knowledge and skills, in addition to their practices by attending disaster preparedness programs or by continuous education. There is a lack of preparedness and continuing programs for nurses toward any emergency conditions and disasters.
There is a limited literature exploring the effect of educational program on the knowledge, skills, and preparedness toward disasters in emergency nurses at the Arab countries including, Jordan. Implementing disaster education programs might be necessary for emergency nurses to enhance their knowledge, skills, and personal preparedness for disasters in order to provide effective patient care and minimize negative consequences.
This study can inform the policy-makers and decision-makers that disaster preparedness of emergency nurses is important for developing the capacity to respond to a disaster situation. The emergency nurses must have the proper knowledge, skills, and personal preparedness for disasters to optimize the response to an emergency. Local officials, hospital administrators, and healthcare professionals especially emergency nurses need to ensure high-quality personal and institutional disaster preparedness and response. New plans are needed to develop continuous disaster education programs to meet emergency nurses’ needs regarding preparation and response to disasters.
Introduction
Disaster is a severe disturbance in a whole community due to natural or man-made hazards that lead to massive casualties, deviations in public health, financial losses, and decline in the quality of life, whereas management of disaster is beyond the ability and capacities of the country’s need for external assistance. 1
Disaster can cause multiple health problems (eg, physical and psychological) for the victims such as injuries, hemorrhage, amputations, fractures, and others. 2 Accordingly, nurses are the major group of healthcare professionals that have direct contact with the victim, thus they play a significant role in minimizing the influences of these crises. As a result of that, they need to improve their knowledge and skills, in addition to their practices by attending disaster preparedness programs or by continuous education about disasters. 3
The findings of studies regarding nurses’ knowledge and skills were diverse, some studies reported that there was insufficient knowledge and skills among nurses, 4 which could be due to a lack of nurses’ preparedness toward any emergency conditions and absence of continuous education programs. 5 Hodge et al 6 found that 44.6% of the American nurses were less familiar with the preparation for catastrophe. Another study conducted by Ghezeljeh et al 7 found that there were higher knowledge and attitude scores regarding disaster preparedness after education using the virtual social network. An integrative literature review found that studies using the Disaster Preparedness Evaluation Tool (DPET) reported moderate disaster preparedness and knowledge, while studies using other instruments largely reported inadequate disaster preparedness and knowledge. 8
Continuous nursing education has a significant association with increasing knowledge and improving clinical skills among nurses which leads to a decrease in mortality rate and enhances the quality of care. 9 Alim et al 10 found that training programs and disaster drills promoted knowledge and improved skills and attitudes among nurses. Additionally, Koca and Arkan 5 demonstrated the effectiveness of training programs in raising the awareness level among nurses in response to disasters.
In Jordan, which is considered one of the Arab countries, the risk of disasters increased due to the presence of wars in neighboring countries, the presence of refugees, and pandemics such as the virus COVID-19, which led to many negative consequences and psychological problems. 11 A few years ago, the region was exposed to terrorist attacks in November 2005 with the occurrence of casualties and injuries. 12 Another catastrophic event occurred in 2008, after a heavy ice storm, a motor vehicle accident on the Amman-Irbid way in which the victims were referred to 4 hospitals. 12 These disasters consumed the hospitals’ resources, which created difficulty in providing quality healthcare. In 1991, Jordan developed a risk reduction plan to prevent and reduce damage, then in 2008, the National Centre for Security and Crisis Management was established. 13 According to the world risk report in 2019, Jordan ranked 130 among countries that have the possibility of disasters based on vulnerability, susceptibility, and lack of adaption. 14 Hence, all these reports obligate healthcare personnel to enhance catastrophe preparedness and increase public awareness.
There is limited literature exploring the effect of educational programs on knowledge, skills, and personal preparedness for disasters among emergency nurses in Arab countries including, Jordan. There are only 2 published studies about disaster preparedness in Jordan.12,15 Thus, identification and evaluation of such educational programs on disaster preparedness might be necessary for principals, hospital administrators, and emergency nurses to implement this intervention and enhance continuous updating of workshops and training programs to enhance emergency nurses’ knowledge, skills, and personal preparedness for disasters.
Purpose and Research Hypotheses
This study assessed the effect of educational program on the knowledge, skills, and personal preparedness for disasters among emergency nurses. Also, the following hypothesis was suggested; the emergency nurses will experience higher levels of knowledge, skills, and personal preparedness for disasters after attending an educational intervention program.
Methods
Design, Setting, and Sample
A quasi-experimental study and one-group pretest-posttest design was used. The target population was all Jordanian registered nurses (RNs) who are working in emergency rooms from all different health sectors between May 2021 and June 2021. The inclusion criteria involved registered nurses who have at least 1 year of experience in emergency department and didn’t attend any triage or disaster preparedness training courses. However, the exclusion criteria included nurses who were working in administrative positions and did not have direct contact with the patients.
G * power 3.1.9.7 program was utilized to calculate the required sample size. For an effect size of 0.5, a significance level (α) of 0.05, and a power of 0.80, The minimal sample size was 34 participants, so 41 participants were needed according to a rate of 20% expected attrition. The present study recruited the participants using a convenience sampling method.
Approval was obtained from Al-Zaytoonah University of Jordan with reference No# (30/7/2020-2021). All participants who were eligible to participate and agreed to fill the questionnaire were invited after receiving full instructions on how to complete it, so their responses reflected implied consent. Participants were informed that they can withdraw at any time, and they ensured that all data collected will only be used for this research purpose. Data were protected by storing on a password-protected laptop.
Outcome Measures
A structured self-reporting questionnaire was utilized. This questionnaire included the disaster preparedness evaluation tool (DPET) and demographics of the participants (eg, age, gender, level of education, work experience, working hours/week, type of hospital, and participation in a real disaster situation).
DPET questionnaire that was developed by Tichy et al 16 was used in this study, however, the modified Arabic version was adopted. 12 This version divided into 3 sections: the disaster preparedness phase includes 25 items. The second section referred to mitigation phase, which measures the response to the disaster and consists of 14 items and the third section is the disaster recovery phase that measures response to a disaster and consists of 6 items. Additionally, these items assess knowledge (13 items), skills (11 items), and preparedness for disaster management (21 items). All items’ responses were measured on a Likert scale from one (strongly disagree) to 6 (strongly agree). The scoring system for the DPET scale and subscales according to the mean was as follows: 1 to 2.99 reflects weak perception of preparedness, 3 to 4.99 indicates moderate perception, and 5 to 6 reflects strong perception. 12 The Arabic version of the DPET was valid and reliable, in which the Cronbach’s alpha for the total DPET scale was 0.90, and for the knowledge, skills, and post-disaster management subscales were 0.91, 0.90, and 0.91, respectively. 12
A pilot study was conducted on 5 emergency nurses to assess the clarity, understandability, comprehensibility of the questionnaire before it was administered to participants. The results confirmed that the questions were clear, understandable, and comprehensive. Those 5 RNs were excluded from the main study sample.
Intervention Procedure and Data Collection Process
At the beginning in order to recruit a study sample, announcements about the study were sent to the Jordanian Nurses and Midwives Council (JNMC) to disseminate to emergency nurses who met the inclusion criteria in all health sectors. Around 100 emergency nurses agreed to engage in this intervention study, but when the program was initiated, only 50 RNs completed the pre-assessment questionnaire. The data in pre-assessment were collected, in which the online survey was launched using the “G-mail Google” platform, and the link to a google form was shared on social media, for example, Facebook and WhatsApp. This survey link was pilot tested for usability and technical functionality on 10 nurses who met the inclusion and the findings demonstrated that the link was easy to use and functioned well. All the questions were indicated as mandatory, thereby, all submitted forms were complete. Additionally, each nurse had one chance to submit the questionnaire and a second trial was automatically denied. The nurses were also asked to mention their telephone numbers in order to contact them for program induction.
The intervention consists of an educational program that was developed by the researchers based on the literature. This program was validated using the content validity index (CVI), which evaluates the degree of matching of intervention with the study. The CVI was assessed by asking 3 experts in disaster and crisis management who were provided with a full description of the study purpose, questionnaire, and the intervention, in addition to CVI form for scoring the items related to the intervention. All aforementioned data and CVI form were sent by e-mail to the experts. CVI consists of a scale of 4 options for each item of the tool, which was scored as follows: 1 = no relevance, 2 = somewhat relevant, 3 = has relevance but needs to be changed slightly, and 4 = has relevance. After returning the experts’ responses, they reported that the intervention was clear, simple, and accurate, but they suggested adding a brief part related to psychological management.
Due to the COVID-19 pandemic and work overload, in addition to restrictions regarding social distance, the Zoom application was chosen to be the best way to conduct the educational program. The nurses who completed the questionnaires were contacted through their phones and the link was provided to them.
The intervention was performed as follows: firstly, the pre-assessment was performed before the program to assess their levels of knowledge, skills, and personal preparedness for disasters. Secondly, the nurses were divided into 2 groups according to their time preferences, then they enacted the intervention sessions. These sessions were held over 8 h, in which 2 sessions were conducted over 1 week (4 h for each session), and a break time of half an hour was provided after every 2 h.
This educational program was divided into 5 topics, which are explained in Table 1. Also, PowerPoint presentations, scenarios, videos, and group discussions were utilized as learning strategies. The program was run under the supervision of the researchers to monitor nurses during the intervention. The Zoom application was synchronous, in which the participants were asked to open cameras during their attendance for sessions. Furthermore, upon the completion of each session, a group discussion was facilitated by the researchers to obtain participants’ reflections on the contents. The same sessions were administered for every group.
Educational Program of Disaster Management.

At the end of all sessions, the same 50 RNs nurses were requested to complete the questionnaires online. All the data were recorded in one file, which was kept on the computer with a special code and was not backed up to maintain confidentiality. The participants did not receive any gifts or compensation due to their participation due to difficulty in reaching those nurses because of COVID-19 quarantine.
Statistical Analysis
Data were analyzed using the Statistical Package for Social Sciences (SPSS) version 25 software (IBM Corp., Armonk, NY, USA). Descriptive statistics (mean, standard deviation (SD), frequency, and percentages) were used to describe the study variables. The paired t-test was used to compare the differences in knowledge, skills and personal preparedness for disaster before and after conducting educational program. The P value ≤.05 was considered as level of significance.
Results
A total of 50 nurses completed the study. The findings found that 58% of the participants were females. The mean age of the participants was 32.3 years (SD = 6.3) and the mean of their experience was 8.2 years (SD = 6.4). The mean of working hours/week was 45.9 h (SD = 9.2). One-half of the nurses (50%) did not participate in a real disaster. For more details, depict Table 2.
Demographic Characteristics of the Study Sample.
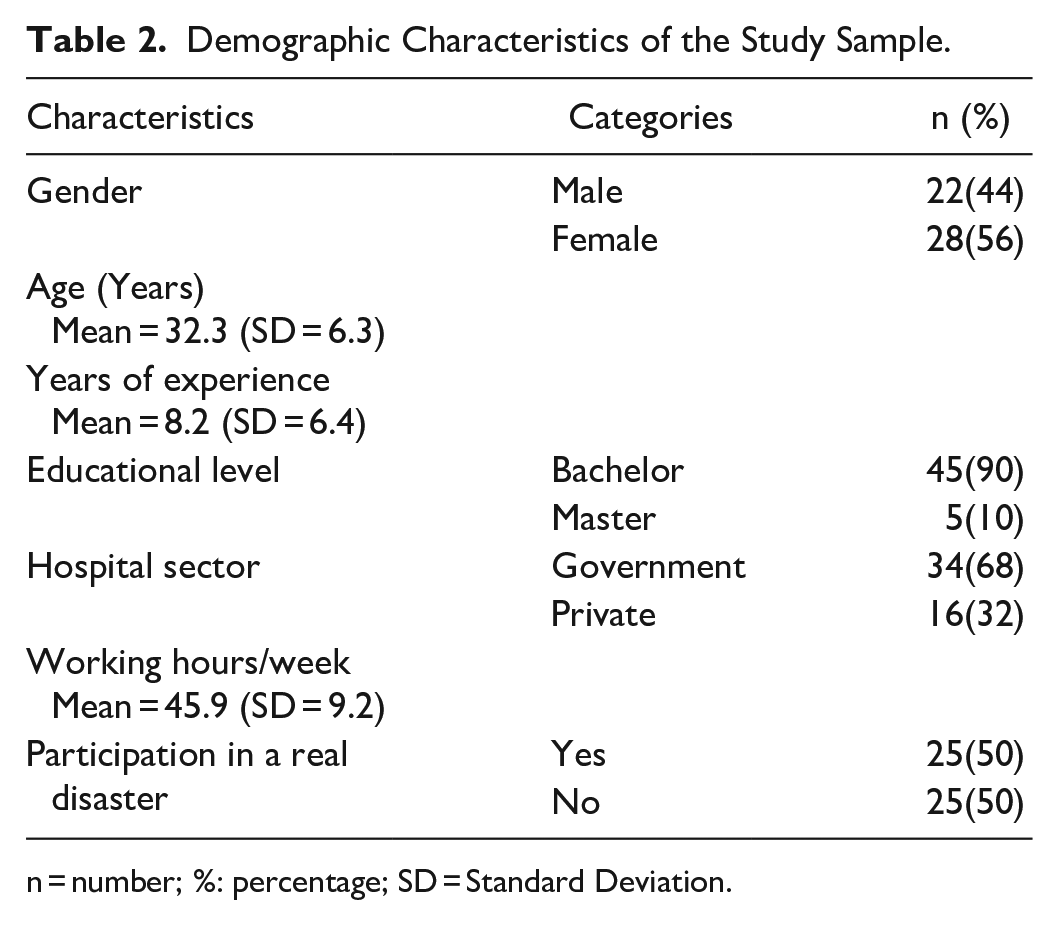
n = number; %: percentage; SD = Standard Deviation.
Regarding pre-intervention knowledge, skills, and personal preparedness levels, the findings showed that nurses’ mean score of DPET was 3.90 (SD = 0.9), which reflected a moderate level. Additionally, the mean scores for knowledge, skills, and personal preparedness were as follows: 4.27(SD = 0.14), 3.88 (0.16), and 3.8 (SD = 0.14), respectively, which indicated that the nurses had moderate levels of knowledge, skills, and personal preparedness as shown in Table 3.
Differences Between Pre-post Intervention Regarding Knowledge, Skills, and Personal Preparedness About Disaster.
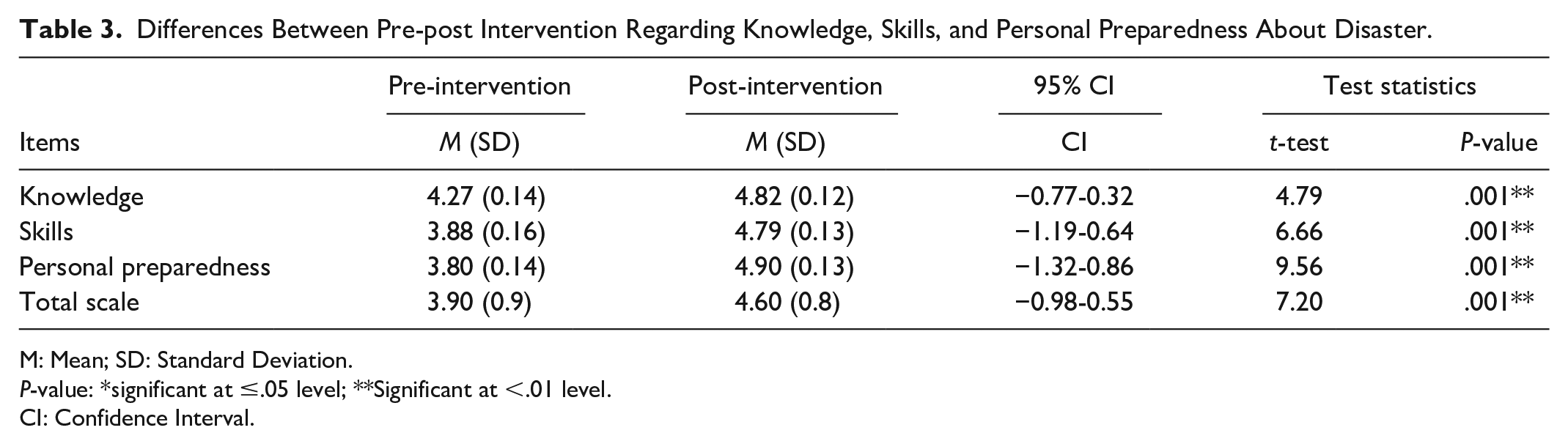
M: Mean; SD: Standard Deviation.
P-value: *significant at ≤.05 level; **Significant at <.01 level.
CI: Confidence Interval.
On the other hand, post-intervention findings showed that the nurses knowledge, skills, and personal preparedness had mean scores of 4.82 (SD = 0.12), 4.79 (SD = 0.13), and 4.9 (SD = 0.13), which reflected that the nurses reported moderate levels of these variables. Also, the mean score of DPET was 4.60 (SD = 0.8), which indicated a moderate level of DPET (Table 3).
Table 3 explains the differences between study variables pre-post intervention program using the paired t-test for the study sample. Findings showed significant differences between pre-post intervention for knowledge (t = 4.79, P ≤ .001), skills (t = 6.66, P ≤ .001), and personal preparedness (t = 9.56, P ≤ .001). Furthermore, there was a significant difference between the pre-post intervention for total DPET (t = 7.20, P ≤ .001). These findings supported the positive effect of an educational intervention program on increasing the nurses’ knowledge, skills, and personal preparedness for disasters.
Discussion
This study aimed to evaluate the effect of disaster education program on emergency nurses’ knowledge, skills, and personal preparedness for disasters. Our findings supported the study hypothesis, in which nurses had higher knowledge, skills, and personal preparedness for disasters after attending an educational program as an intervention, however, the levels remained moderate. Our results are consistent with previous studies adopting educational programs as intervention for disasters. Brewer et al 17 found a moderate level of knowledge, skills, and preparation for disaster management among Australian emergency nurses. Palameta and Gyarmati and colleagues 18 found that effective training enables the gaining of knowledge and skills. Also, Pesiridis et al 19 demonstrated that continuous education and training courses increase the knowledge level of disaster management. Alim et al 10 reported an improvement in the level of knowledge in addition to practice after disaster preparedness training and disaster drill. Xia et al 20 found the improvement in triage skills may be due to training on scenarios that contribute to improving the level of these skills. Ahayalimudin and Osman 21 documented that training creates preparedness to cope with the effects of disasters. Additionally, multiple teaching methods such as videos and presentations were effective in improving skills and knowledge about disaster. 22 On the contrary, Al razeeni 23 found weak to moderate knowledge and skills among Saudi emergency medical services personnel.
The findings found that the levels of knowledge, skills, and personal preparedness for disasters after the intervention program were moderate, which could be due to a lack of nurses’ knowledge of workplace emergency management plans and emergency response procedures, lack of experience in disaster causality and preparedness, and inadequate practical disaster training programs.13,24 The capability of nurses to make significant contributions to disaster planning forums is affected by lack of access to disaster management policies and management commitment and support, in addition to lack of research.24,25 The participants of this study demonstrated that lack of local official resources and support, lack of research and international literature, and lack of participation in disaster planning and management were the lowest scores on the scale. Thus, this program clarified the importance of having knowledge and skills for nurses to respond effectively in emergency cases. 26
Our findings showed that the nurses reported a moderate level of disaster preparedness after intervention program, but there was a significant improvement after attending an educational program, which may reflect the positive effect of disaster training. Other studies found a moderate level of preparedness.12,13,27-29 On the contrary, earlier studies demonstrated low disaster preparedness levels.3,6,30-33 Joes and Dufrene 34 considered preparation for disastrous events as the highest priority for healthcare professionals. Additionally, Al-Ali and Abu Ibaid 13 demonstrated that nurses who receive continuous training in their workplace were more prepared than others. Therefore, continuous educational programs should be implemented for emergency nurses.
Limitations of the Study
Regardless of the significant results, this study had the following limitations; the design was one group, which could affect the results due to the lack of a comparison group to determine if other situations influenced them during the implementation of the program. Additionally, this study was conducted during the COVID-19 pandemic, in which the findings could be due to this emergency situation that required nurses to acquire knowledge about disaster preparedness. The present study evaluated short-term acquisition of knowledge and skills, while monitoring and assessment may require a longer time to evaluate changes in knowledge, skills, and personal preparedness. Also, the skills part was not completed as intended, in which the researchers planned to do demonstration/re-demonstration on models /manikins, such as BLS, wound care, triage scenarios, and others due to the COVID-19 quarantine. Moreover, a mixed method or qualitative approach would improve understanding of the study results by exploring nurses’ experiences of their disaster preparedness.
Implications for Practice
Recurring global disasters threaten human life. Disaster preparedness of emergency nurses is important for developing the capacity to respond to a disaster situation. Emergency nurses must have the proper knowledge, skills, and personal preparedness for disasters to optimize the response to an emergency. Healthcare administrators and healthcare professionals need to ensure high-quality personal and institutional disaster preparedness and response. New plans are needed to develop continuous disaster education programs to meet emergency nurses’ needs regarding preparation and response to disasters.
Local officials and hospital administrators should provide facilities and resources including support and access to literature or research about disaster preparedness for the emergency nurses. Limited access to internationally published research, especially in many developing countries, can significantly affect effective disaster preparedness and management. 25 Also, emergency nurses should be active participants in creating new guidelines, emergency plans, on the local or national level. Lack of involvement in disaster emergency planning means that nurses are not involved in disaster planning for communities.
Conclusion
This study confirmed that an educational intervention program about disasters was an effective intervention that can improve the knowledge, skills, and personal preparedness among emergency nurses. The results provide evidence for hospital administrators the need for implementing continuous education and training programs about disasters due to increasing frequency of disasters worldwide. Study findings emphasized that the disaster preparedness of nurses can be improved and emergency nurses should play their best role in coping with future disaster situations. In-service educational departments in each hospital should develop disaster guidelines and provide continuous disaster training to emergency nurses. Furthermore, a pre-posttest control group design is recommended to evaluate the effects of such a program among emergency nurses.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The approval to conduct this study was obtained from the Institutional Review Board (IRB) at Al-Zaytoonah University of Jordan with reference No# (30/7/2020-2021).