
Abstract
People with Parkinson’s disease (PwP) experience a variety of symptoms and fluctuations in these, which they have to cope with every day. In tailoring a person-centered treatment to PwP there is a lack of knowledge about the association between pre-dominant coping behaviors and clinical markers among PwP. To describe and compare specific clinical markers between 6 suggested coping behaviors. Thirty-four PwP, who previously had been classified into 6 different pre-dominant coping behaviors, were included in this mixed methods study. Six primary variables were included in the descriptive analysis; motor function (UPDRS-III), non-motor symptoms score (NMS-Quest), change in bradykinesia score, apathy score (LARS), personality traits (NEO-FFI), and cognitive status (evaluated by a neuropsychologist). The merged results of this mixed methods study indicate that clinical markers as apathy, burden of non-motor symptoms, cognitive impairments and personality traits, have the potential to impact the coping behavior in PwP. In a clinical setting the markers; NMS-burden, degree of apathy, cognition, and personality traits may indicate specific coping behavior. Three of the six suggested typologies of coping behaviors differed from the other groups when comparing descriptive data. In order to improve patient care and guide the development of person-centered therapies, each PwP should be approached based on those typologies.
Keywords
It is a fact that people with PD (PwP) have to live with a varity of fluctuations in symptoms, which leads to unpredictability in everyday life, and that they cope with these challenges with either problem-focused or emotion-focused strategies.
It requires specific coping behaviors to maintain quality of life and mental health in living with PD. This study aims to relate clinical markers with 6 previously identified types of coping behaviors.
We want to individualize and tailor the support to PwP in coping with everyday life. The distinctions between the 6 coping types were elucidated and analyzed in combination with the clinical data, thus creating new targets for therapeutic interventions in Parkinson’s disease based on specific coping behavior. The possible relationships between the 6 coping behaviors and the exploratory, descriptive results should form the foundation for further validation studies.
Introduction
People with Parkinson’s disease (PwP) have to cope with physical, cognitive and social consequences of the disease, and live with uncertainty about long term outcome as well as unpredictability of recurrent fluctuations in symptoms depending on the stage of disease.1,2 Coping can be defined as “cognitive and behavioral efforts to manage specific external and/or internal demands (stressors) that are appraised as exceeding the resources of the person.” 3 Certain coping strategies are negatively associated with risk of depression, mortality, Quality of life (Qol) and bodily comfort.4-6 It requires development of individual strategies to copewith the impairments, which again may be determined by several factors, such as response to medication, cognition, personality traits, non-motor symptoms (NMS), affective disorders and personal factors as age, gender and socio-demographics variables.5,6 However, uncertainty about phenotypes and variability in disease progression and how to cope with disease-related impairments in PD, still prevails.7,8 Therefore, we lack knowledge about the relationship between clinical variables and certain coping strategies among PwP.
Coping behavior can characterize how individuals’ interact with their environment, and what emotional, cognitive, and behavioral responses they employ to manage specific stressful encounters. 9 A few general coping questionnaires have been validated in groups of PwP. 8 The Ways of Coping Questionnaire (WCQ) is a quantitative tool and is commonly used to assess coping strategies in PwP.10-12 However, this scale may not accommodate a multi-dimensional approach to coping. A previous qualitative study using the method Video-based Narratives with an identical sample integrated in this mixed methods study, 6 predominant coping types, were suggested 13 :
(1) The convincing behavior (characterized by a focus on pushing physical capacity and level of daily activities to stop disease progression)
(2) The economizing behavior (characterized by always being a step ahead, building everyday life around physical disabilities, and preserving regular habits and routines)
(3) The encapsulating behavior (characterized by use of regressive strategies and withdrawal primarily from social relations, but also from the world in general)
(4) The evasive behavior (characterized by keeping the disease a secret, immersion into creativity, and attending social/cultural activities, which serve as mental “free spaces”)
(5) The adaptable behavior (characterized by balancing limitations and appreciating life, and letting symptoms shape activities during the day)
(6) The dynamic behavior (characterized by living through self-set goals, and willingness to make radical, life-altering changes to accomplish these goals).
The results from this previous study showed that the PwP`s specific coping behavior may impact the preservation of the integrity and the way in which the PwP cope with disease-related changes. 13
Traditional and early conceptualizations of coping behavior have been categorized as emotion-oriented (avoidant) versus problem-oriented (active) coping.14,15 Problem-oriented strategies focus on changing aspects of the environment and the person’s relationship to it (psychological mechanisms). Emotion-oriented strategies focus on managing one`s emotional responses to stressors (behavioral mechanisms) and preventing people from directly engaging with the stressor.14-16 Theoretically discussing the 6 pre-dominant coping behavior and the conceptualized coping styles, we found that the emotion-oriented coping behavior is exhibited by those demonstrating Encapsulating and Evasive behavior, and the problem-oriented coping style is exhibited by those demonstrating Convincing, Dynamic and Economizing behaviors. The Adaptable behavior seems to exhibit a mix of both styles.
What determines outcome of distinct coping behavior is complex, and the literature uncovers many different perspectives. Some studies suggest that individuals with moderate motor symptoms use more avoidance coping compared to individuals with mild motor symptoms14,17 whereas others find that behavioral factors depend on NMS rather than on motor symptom severity.18-20 Further, studies suggest that apathy is a frequent symptom in PD, and that apathy is significantly associated with specific cognitive impairments (especially executive dysfunctions), and manifest differently than depression.21,22 Also, a factor as personality traits is often discussed in terms of coping and how these may mediate behavioral strategies. 23 Thus, the interplay between coping behavior, the subsequent effect on different parameters related to the disease, and the best way to support the PwP based on knowledge about coping behavior, remains unclear. 12
The 6 pre-dominant coping types described in the previous study 13 can be seen as multi-dimensional phenotypes bridging the possibility to offer a more tailored support to PwP in coping with everyday life. However, prior to using these phenotypes, the distinctions between the predominant coping types must be elucidated, and be analyzed in combination with the clinical data from the individual PwP. Therefore, the aim of this mixed methods study is to describe and compare potential physiological, cognitive, affective, and psychosocial markers with the 6 coping typologies, creating new targets for therapeutic interventions in PD based on coping behavior.
Methods and Materials
Design
This study is the final sub-study of a mixed methods study (MM-study) with an identical sample. Both quantitative and qualitative data were concurrently collected within a timeframe of 6 weeks due to the MM-design. 24 The results in the quantitative study (Study I), where a quantification of the ADL-level based on accelerometer measurements was made, 25 co-determined both the data collection in Study II 13 and was used as a primary variable (Change in bradykinesia score) in this study (Study III). Hereby, clinical variables will be described and compared to each of the 6 pre-dominant coping behaviors, merging the quantitative and qualitative results. The different phases in the study are shown in Table 2.
Participants
Thirty-four patients with PD were included in the study. Participants were recruited consecutively from the neurological outpatient clinic for Movement Disorders at Zealand University Hospital, Denmark, and from the Danish Parkinson Association. The sample size was based on previous experience in similar studies26,27
Inclusion criteria were: Fulfilling the Movement Disorder Society diagnostic criteria, 28 age of 50 to 75 years (mean age of PD-diagnosis time), PD-duration of 3 to 7 years, mild to moderate PD (Hoehn and Yahr scale 2-3), and non-dementia based on a cut off score >26 in The Montreal Cognitive Assessment (MoCA). 29 Further, number of PD-drugs, minimum of 1 and a maximum of 3, and number of daily doses (max of 4) was set. Exclusion criteria were patients with advanced treatments (including Deep Brian Stimulation, DBS), and severity in co-morbidity (cut off <6, assessed in the Charlsson Co-morbidity Index). Characteristics of the participants are presented in Table 1.
Demographics and Clinical Characteristics for all the Participants.
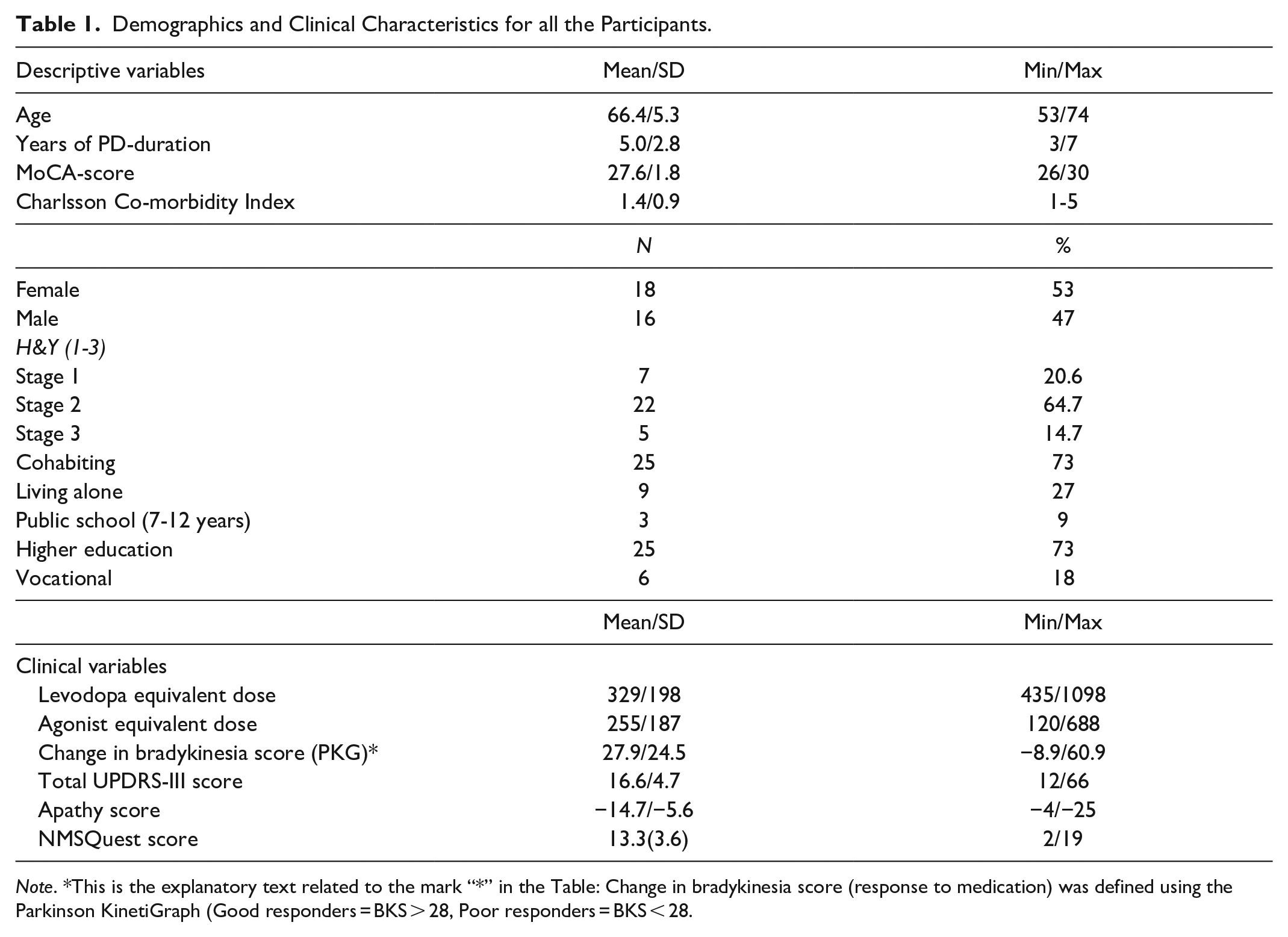
Note. *This is the explanatory text related to the mark “*” in the Table: Change in bradykinesia score (response to medication) was defined using the Parkinson KinetiGraph (Good responders = BKS > 28, Poor responders = BKS < 28.
Qualitative data collection
Data were collected with use of the qualitative method, Video-based Narratives (VN), 30 which consists of 2 phases: (1) PwP performing ADL-situations were recorded in their private homes, and (2) subsequently qualitative interviews were conducted based on the video-sequences. The PwP were presented with the video-files after a short introduction during the interview, and the following questions referred to and revolved around the challenges in everyday life with PD, the coping behavior presented in the video-sequences, the motivation leading to the behavior and the consequences of the behavior. Each interview was transcribed verbatim.
Qualitative Data Analytics
The identification and extraction of the 6 pre-dominant coping behaviors was based on an abductive content analysis inspired by Graneheim and Lundman and Lundmann. 31 The data sources and analysis procedures are previously described in more details. 13
Quantitative data collection
All participants underwent a comprehensive test battery consisting of both clinical tests, various ratings and questionnaires, and an extensive neuropsychological examination. Six primary variables were subsequently selected based on literature within the field suggesting relationships between some of the variables14,19,32 and from results of Study I. 25 Additionally, the selection of variables was based on the behavioral traits that emerged within the 6 pre-dominant coping types derived in the qualitative phase of the study. 13
Therefore, the 6 selected variables were: Unified Parkinson Disease Rating Scale part III(UPDRS-III) score, 33 response to dopaminergic treatment based on change in bradykinesia score (BKS-change) from the accelerometer measurements, Parkinson’s KinetiGraph™ (PKG), 34 Lille Apathy Rating Scale (LARS), 35 Non-motor Symptoms (NMSQuest), 36 personality traits (NEO-FFI) 37 and cognitive status determined by a neuropsychologist (IUL). All the questionnaires/scales are previous validated.
UPDRS-III
The severity of motor symptoms was evaluated using the UPDRS-III ( which is a widely used clinical tool for the assessment of motor symptom severity in PD.33,38 Scores range from 0 (asymptomatic) to 132 (most severe). 33
Change in BKS
In Study I as part of the overall study, the response to morning medication was shown to predict the overall ADL-level throughout the day25. The response to dopaminergic treatment was measured based on change in bradykinesia score (BKS) using the PKG™, an accelerometer placed on the wrist on the most affected side of the patient which was used to measure motor symptoms in 6 days. 34 All movements were recorded and processed through the algorithm that determined the bradykinesia-score (BKS). “Poor responders” to medication were classified by a small change in BKS (mean difference < 28 BKS), and opposite, “good responders” were those PwP with a greater change in BKS (mean difference > 28 BKS). 25 The mean change in BKS for each PwP was calculated and used as a variable in the present study.
Lille Apathy Rating Scale (LARS)
LARS is a 33-item semi-structured interview including 9 domains (everyday productivity, interests, taking initiative, novelty seeking, voluntary actions, emotional responses, concern, social life, and self-awareness). The scores range from −36 to +36, with higher scores indicating more apathy 35
Non-Motor Symptom Questionnaire (NMSQuest)
The NMSQuest is a dichotomous scale divided into yes/no answers. It measures frequency and severity of non-motor symptoms based on 30 self-reported questions of 9 domains. 36 The sum of all the positive answers (“yes”-answers) provides the total score on the scale, which indicates the burden of NMS in each individual 39
Assessment of Cognitive Status
A battery of neuropsychological tests sensitive to early stage PD cognitive dysfunction was applied. All patients were examined by the same neuropsychologist, and tests were applied in a fixed order. The assessment was built on different sensitive tests within the domains: memory, psychomotor speed/attention, executive functions and visuospatial functions.
For each test, a regression analysis was performed with the test score as the dependent variable and age, gender and education years as independent variables. These regression analyses were conducted using the existing Danish normative data collected at the Danish Dementia Research Centre, Rigshospitalet. For each patient, the observed score on a test was compared to the expected test score and the difference score between the observed and expected scores were used to evaluate impairment. Difference scores in the lowest 10% of the normal variation were categorized as impaired. This procedure has previously been described and used in different patient-groups40-42
Assessment of Personality Traits (NEO-FFI)
The Danish version of the NEO 5 Factor Inventory (NEO-FFI) was applied to assess personality traits. NEO-FFI is based on the 5 Factor Model (FFM) of personality traits which is the most widely used model of personality traits. According to the FFM personality can be described by 5 broad personality factors or dimensions, which are Neuroticism, Extraversion, Openness to experience, Agreeableness and Conscientiousness. 37 Data on the comprehensiveness of the model and on the reliability, validity, and stability of measures of the factors are reviewed and tested in several studies, and are widely used in clinical practice. The NEO-FFI consists of 60 items answered on a 5 point scale ranging from “strongly disagree” to “strongly agree.” Administration of the NEO-FFI takes 15 to 20 minutes and each participant completed the inventory in the presence of the neuropsychologist who answered questions regarding the formulation of items or specific words.
Quantitative Data Analysis
Statistical analyses were performed using R Studio
Descriptive statistics were used to describe and summarize the variables within the 6 groups and are presented in Tables 1 and 3 (joint display showing the integration of the results). P-values will not be presented since sample size is too small to present robust statistical conclusions.
The 6 primary variables were included in the analysis and characterization of the 6 groups with pre-dominant coping behavior: 1 = The convincing behavior, 2 = The economizing behavior, 3 = The encapsulating behavior, 4 = The evasive behavior, 5 = The adaptable behavior and 6 = The dynamic behavior. The 6 groups and each of the 4 numeric variables consisting of the LARS-score, the NMSQuest-score, the UPDRS-III score and change in BKS, were compared and the results are visualized in boxplots (Figure 1).
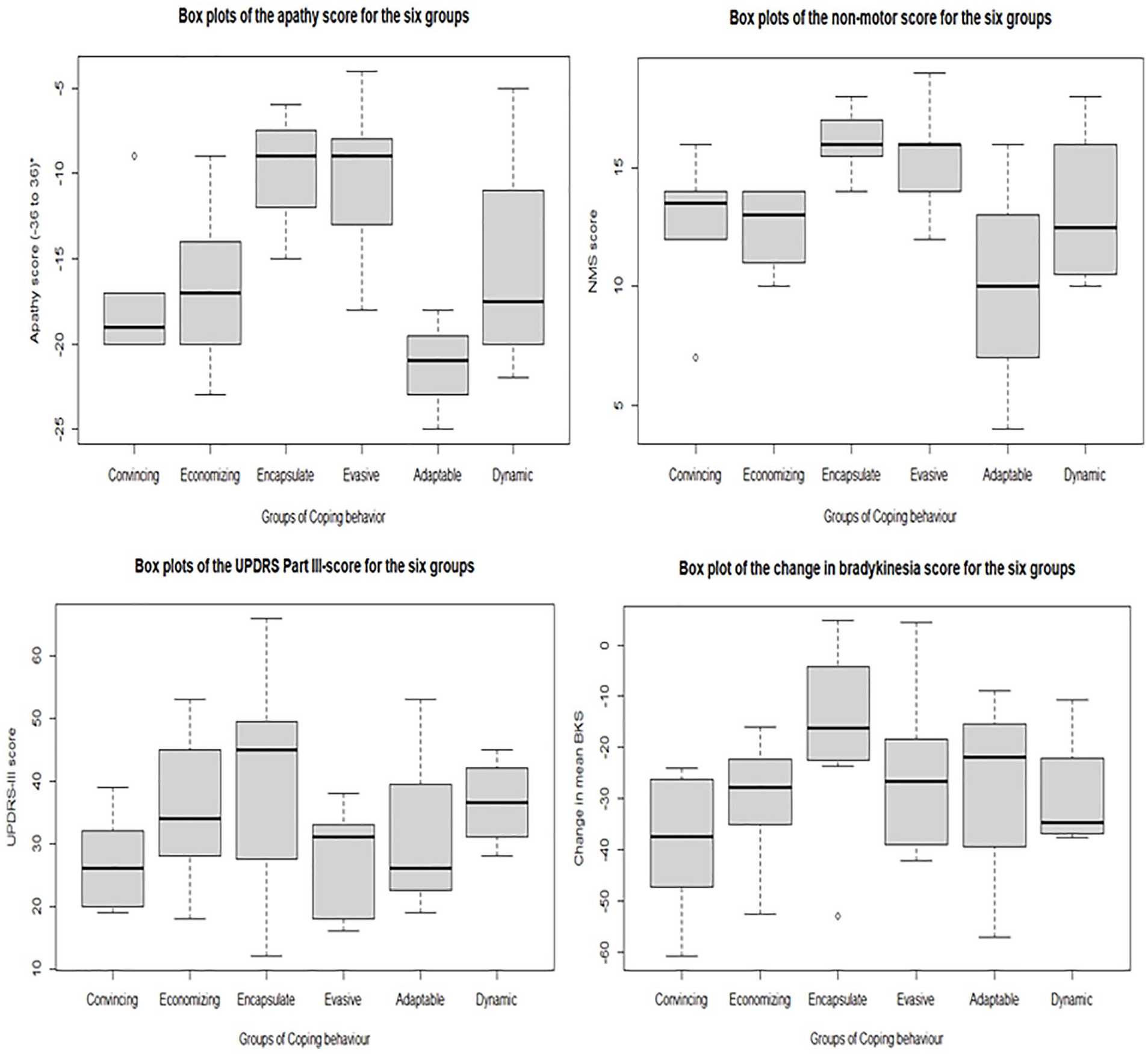
Boxplots of the descriptive analysis between the 6 groups and the 4 numeric variables.
Also, the 2 categorical variables (cognitive status and personality traits) were included in the descriptive analysis. The personality profiles for each of the 6 groups are presented in Figure 2. The T-scores (normal data) in NEO-FFI were used in the analysis. Each group was plotted against the 5 personality traits to descriptively detect differences in personality between the groups.

Boxplots of the 5 personality traits (NEO-FFI) presented in the groups.
Mixed Methods Integration
After completing the qualitative and quantitative analyses, the 6 pre-dominant coping behaviors were compared and merged with the quantitative results. The purpose of the mixed methods integration was to compare the 2 sources of data to gain a more complete understanding of clinical, descriptive variables related to the specific coping behavior. The analysis and interpretation are presented in a visual joint display (Table 3)
Results
Out of 47 initially recruited, 11 PwP were excluded due to a low score in the MoCA-test. Two PwP dropped out of the study. A total of 34 PwP fulfilled the required criteria and provided data for this study. Characteristics are presented in Table 1.
By comparing the scores the results showed that the apathy-score and the NMS-score differed between the groups. The individuals with the Encapsulating and Evasive behavior had a greater average value within apathy compared to the other groups. Within both groups all the individuals had either moderate (−16 to −9) or severe apathy (score > −9). The groups with Encapsulating and Evasive behavior also differed from the other groups within the NMS-score presenting a much higher NMS-burden. The response to medication (BKS-change) and the motor functionality (UPDRS-III-score) did not seem to differ between the groups when comparing the scores. The results are illustrated in Figure 1 via boxplots.
Descriptively, “Good responders” to dopaminergic medication (change in BKS > 28) display a low NMS-score and vice versa. This relation is not indicated comparing the scores in MDS-UPDRS (motor severity).
Summarizing the personality profile based on NEO-FFI, a rather high degree of diversity in personality profile between the groups, was found. In general, a low Neuroticism score and Extraversion score, and high level of Conscientiousness, Agreeableness and Openness were dominant features of the overall PwP personality traits. All the individuals with Economizing behavior presented the highest score in Conscientiousness. Individuals with Encapsulating behavior display the highest score in Neuroticism compared with the other groups.
Mixed Methods Findings
Conducting a mixed methods study a primary result is how the study is designed and how the different phases are integrated. 24 Table 2 shows the mixed methods design and the different phases in the overall study.
Overview of the Concurrent Mixed Methods Design Used in This Study.

Subsequently, the synthesizing of quantitative and qualitative results leads to the “core” result, the development of a joint display presented in Table 3. The joint display merges the qualitatively defined groups of coping behavior with the quantitative variables. The descriptive analysis of the variables showed several differences between the groups seen from a clinical perspective, but only the apathy-score and the NMS-score differed between the groups when comparing the scores.
Joint Display of the Qualitative and Quantitative Results and the Meta-inferences Drawn Based on the Integration of Methods.

High score in UPDRS-III = high level of impairments. bHigher score = higher degree of apathy. In the comparison, Group 3 and 4 differ in the apathy and NMS-score from the other groups.
The joint display is organized by the 6 coping groups, and merges the results of the analysis from the quantitative and qualitative data. The interpretations are based on a comparison on how data are congruent, discordant or expands the understanding of the research question. 24
The quantitative results expand the understanding of the qualitative findings (the 6 pre-dominant coping behaviors) as physiological, cognitive, affective, and psychosocial characteristics can be compared to each coping behavior.
Three of the 6 pre-dominant coping behaviors differed from the other groups when comparing the descriptive results between the groups. The individuals with Convincing behavior display the overall best scores on the clinical parameters compared to the other groups. Congruent with this the individuals’ present capability to focus on physical training and bodily functions. The behavior is reflected in this quote: “I have high demands to myself. . . it affects me every day. . .. I do not always enjoy it, but I have to be able to do things I could before, as much as possible” (C4). At the same time the individuals present the highest personality test score in Agreeableness and lowest score in Neuroticism (Figure 2).
The Encapsulating behavior and Evasive behavior share some of the same clinical features. However, the individuals with Evasive behavior have a rather good motor function. The high apathy scores in the individuals with Evasive behavior are discordant with the qualitative finding suggesting that they use social interactions as “free spaces” (mental strategies). This strategy is reflected in a high score in Openness evaluated by the NEO-FFI scale.
Apathy scores, non-motor scores and percentage of cognitive impairments were high within both the Encapsulating and Evasive behavior, confirming the qualitative findings as these groups use avoidance strategies in coping with PD. Additionally, individuals within the Encapsulating behavior show the highest degree of apathy and cognitive impairments among the groups.
Discussion of the Mixed Methods Findings
The results show that clinical markers such as apathy, NMS, cognitive impairments and personality traits may be related with distinct coping behavior in PwP. The groups with Convincing, Encapsulating and Evasive behavior separate themselves compared with the other groups.
Most PwP in stage 2 and 3 in H&Y report a score of 10 to 12 NMS-points. 36 Our cohort has a mean score of 2.2 in H&Y and 13.3 in the NMSQuest. A high NMS-burden and apathy-score are related to Encapsulating behavior and Evasive behavior, which indicate more emotion-oriented coping behavior with elements of avoidance embedded. 13 Previous research shows specifically that poorer mental and physical health is related to the use of emotion-oriented coping.15,43,44 This is in line with our results showing that individuals using Evasive or Encapsulating behavior also are more likely to have cognitive impairments compared to the other groups, and tend to have poorer motor function as indicated by a high UPDRS-III-score.
Studies have suggested that severity of motor symptom may affect coping behavior, as higher levels of overall motor symptom severity were associated with increased use of coping with avoidance elements.7,14,45 However, Ehlen et al suggest that behavioral factors depend on the degree of NMS, rather than on motor symptom severity, and NMS may be stronger determinants of coping strategies than motor symptoms. 46 Our results indicate that, coping behavior with avoidance elements, for example, Encapsulating behavior may primarily be related to the NMS-burden and apathy score. The results apply well with the results in Study I as “poor responders” to medication reported most disabilities in performing ADLs related to NMS-items. 13 However, the assumption needs to be verified in a larger study with a specific symptom profile included.
According to the NEO-FFM, low levels of Neuroticism and Extraversion, and high levels of both Conscientiousness, Agreeable and Openness were found in the cohort, thus, the results of the personality test revealed a different profile than anticipated. In several studies, as in a meta-analysis from 2018 including 17 studies, a personality profile in PwP was delineated and showing high levels of Neuroticism and low in Agreeableness in PwP. 47 However, this profile is characterized by involving PwP in the pre-motor phase of the disease. Other studies show that Neuroticism is associated with use of avoidance strategies and cognitive impairments23,48 and the persons tend to be more readily worried, have difficulties in managing stress, to be rigid, and resistant to changes. 48 This is in line with our results, as the individuals with Encapsulating behavior presented the highest score in Neuroticism compared to the other groups 6 out of 7 PwP with this coping behavior were evaluated by the neuropsychologist as being cognitive impaired. Specific personality traits may influence the type of coping behavior used to overcome sudden troubles and tolerate, reduce, or minimize stressful events. 47 However, given the fact that PD is characterized by the degeneration of the dopaminergic pathways, the personality traits may be interpreted as a consequence of decreased dopaminergic transmission in the striatal regions as previously reported.48,49
Both the Adaptable and Dynamic behavior present dynamic features with willingness to consider new ideas, are socially active, and find it easy to think about things in different ways, which help the individuals to adjust easily to changes. These features may also be a part of the coping behavior reflected in individuals with Evasive behavior, as they use social activities and interactions as a “free space,” where they can forget PD for a while. Paradoxically, they also score moderately high in apathy, but by going through the items in LARS, the scores reflect a flattening of affect and loss of emotional interest in other people and not lack of initiative. Also, the individuals with Adaptable behavior are characterized by involving their relatives as part of their coping strategies. Therefore, the behavioral traits may not be captured in “pure forms” but based on the specific features and dominant characteristics within each of the groups. Corti et al made a similar discovery regarding the original 8-factor structure of the WCQ that combined the Distancing and Escape Avoidance as strategies with the same core features. 12 Currently research within coping behavior and chronic illness has shown that individuals may use a pattern of different coping behavior as a repertoire of useful behaviors in different situations.16,50 In terms of the general categorization into emotion—and problem-focused coping a minority of patients with an overlapping form of disease management has been found. These patients with mixed coping strategies differed from those who employed more “pure forms” in terms of cognitive function, depressive symptoms and disease duration.16,50,51 Due to the exploratory nature of this study, future studies should evaluate in which aspects this entity of mixed coping strategies truly differ from other kinds of coping behaviors On basis of the aforementioned considerations, a better clarification of the current “clinical profile” related to distinct coping behavior might allow developing non-pharmacological interventions in order to exploit the coping behavior embedded in each group.
Relevance in Clinical Practise
The results of this study call for an awareness of coping behavior when addressing PwP in an individualized and person-centered approach. For example, individuals with Convincing behavior and Dynamic behavior should be involved in decision-making, perform self-care activities, and even monitor their own symptoms to preserve the sense of integrity and self-autonomy. Also, the Economizing behavior requires a more holistic approach based on patient involvement and an identification of what constitutes “an ordinary day” due to the necessity of regular habits, routines and structure in ensuring well-being and sense of control for those who exhibit this coping strategy. PwP who exhibit Encapsulating and Evasive behavior may benefit from more focused interventions, as there is a growing evidence that emotion-oriented coping with avoidance elements has a significant negative impact on daily life, as this strategy tends to increase daily-life stressors and reduces QoL.15,19,52 Most psychological interventions aimed at changing maladaptive thinking, feelings and behaviors, such as cognitive behavioral therapy (CBT), are predicated on emotion-oriented coping. 53 Also, non-pharmacological interventions such as mindfulness, educational programs, health promotion programs, and positive reframing have all shown positive effects on both motor and non-motor symptoms as well as on affective parameters.52-54 Therefore, when considering treatment and psychosocial adjustment to PD, it is important to focus on specific coping behaviors, as it may be advantageously in the context of offering tailored activating therapies. The results of this study should lead to the development of a clinical screening tool enabling healthcare professionals to distinguish between different coping behavior, and thus, different needs. The future screening-tool may have the potential to be generalized to other neurodegenerative chronic disorders with similar symptom profile, for example, people with multiple sclerosis.
Method Discussion
The small sample size of this study precludes robust statistical analysis of the variables, and thus, the results can only generate hypotheses and should be evaluated solely with a clinical perspective. Subsequently, the results do not allow conclusions about causal relationships between the clinical markers and the coping behaviors to be drawn. However, the results of this exploratory study should be seen as a starting point for further research studies testing the possible associations. Using a MM-design allowed us to combine the methods within qualitative and quantitative research and use them as a collective strength in the identification of pre-dominant coping types (Study II) and find clinical markers on each type (Study I+III).13,25 However, this study emphasizes the need for conducting longitudinal research to evaluate the impact of tailored approaches designed to help PwP manage the disease. Future studies should include a larger cohort (divided into the 6 groups) for a longer time period and consider the use of supportive psychoeducational to individualize the treatment.
Conclusion
Specific physiological, cognitive, affective and psychosocial markers were described and compared between the 6 pre-dominantly coping behaviors. In a clinical perspective the markers; NMS-burden, degree of apathy, cognition, and personality traits may indicate specific coping behavior. Change in BKS-score (response to levodopa) and severity in motor symptoms do not seem to indicate specific coping behavior. Of note, the Convincing, Encapsulating and Evasive behavior differed from the other groups based on their descriptive data. Each PwP should be approached based on the typologies within the 6 groups of coping behavior in order to improve patient care and guide the development of evidence-based therapies to improve well-being in PwP and enable healthcare professionals to take the precise therapeutic path in a person-centered approach.
Footnotes
Acknowledgements
This work was supported by grants from the Danish Parkinson Association, and Aase & Ejnar Danielsens Foundation. The authors also want to thank all the PwP for volunteering for this study. Also a thank you to Louise Feldborg Lyckhage for statistical support.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Troels Wesenberg Kjær: Consultant for UNEEG medical. The other authors declare that there is no conflict of interest relevant to this work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Neurological Department, Zealand University Hospital, and from grants from the Danish Parkinson Association, and Aase & Ejnar Danielsens Foundation.
Ethical Compliance
The study conformed to the ethical principles defined in the Declaration of Helsinki and was approved by The Danish Data Protection Agency (REG-110-2017) and the Regional Committee on Health Research Ethics (IRB 58638). All participants received written and/or oral information about the study and gave consent on that basis.
Presence of Declarations,Ethics,and Consent Statements
The study conformed to the ethical principles defined in the Declaration of Helsinki and was approved by The Danish Data Protection Agency (REG-110-2017) and the Regional Committee on Health Research Ethics (IRB 58638). All participants received written and/or oral information about the study before giving consent. We confirm that we have read the Journal′s position on issues involved in ethical publication and affirm that this work is consistent with those guidelines.