
Abstract
Objective
To test associations between socio-clinical factors, self-management and patient activation among patients with Parkinson's disease (PD), and to explore the use of regression tree to find the cut-off levels of socio-clinical factors which associate with lower or higher self-management behaviours and patient's activation.
Methods
A cross-sectional study of patients with PD (n = 62) who underwent assessment of their socio-clinical factors including age, gender, cognitive status, comorbidities, disease severity (motor and non-motor symptoms) and social support. The associations of these factors to specific aspects of self-management behaviours including utilization of rehabilitative treatments, physical activity and patient activation were tested.
Results
Most patients did not utilize rehabilitative treatments. Non-motor symptoms and cognitive status were significantly associated with physical activity (R2 = 0.35, F(3, 58) = 10.50, p < 0.001). Non-motor symptoms were significantly associated with patient activation (R2 = 0.30, F(1, 30) = 25.88, p < 0.001). Patients with Mini-Mental State Exam score ≤24 performed less physical activity, relative to those with a higher score. Patients with ≤5 non-motor symptoms showed higher activation relative to those with >5.
Conclusion
In PD, disease-specific clinical characteristics overshadow other personal factors as determinants of self-management behaviours. The role of non-motor symptoms in reduced self-management behaviours and activation is highlighted.
Keywords
Introduction
Self-management has an important role in the long-term management of chronic diseases, and accordingly, has become a central approach in the management of these diseases.1,2 This approach focuses on the behaviours that people with chronic disease use in order to maintain and improve their health and well-being and includes aspects such as medical (e.g., doctor visits) and lifestyle (e.g., regular exercising) management. In its broad framework, it also includes people's knowledge, abilities and confidence in managing their health.3–5 A higher activation level indicates a patient's higher internal readiness to adopt behaviours that maintain or improve health. 6 Previous studies have shown that engagement in self-management behaviours (SMBs) and a high level of activation result in better health and well-being in a variety of chronic conditions.7–10
Parkinson's disease (PD) is a chronic, progressive, incurable neurodegenerative disorder that affects motor and non-motor (cognitive, emotional and autonomic) functions.11,12 As the life expectancy of patients with PD (PwP) is only slightly shorter than that of the general population,13,14 PwP have to cope for many years with the symptoms of serious illness, including severe disability. Therefore, engagement in SMBs, including rehabilitative care, 15 physical activity16–19 and high activation may be effective tools in fighting the long-lasting burden of the disease. However, knowledge about activation levels among PwP is very limited.
Personal factors such as individual's beliefs, socio-demographic, cognitive variables and disease-specific related clinical characteristics may play an important role in engaging in SMBs in chronic conditions.20–29 In PwP, disease severity (i.e., non-motor symptoms) and social support were found to have a major role in engagement in SMBs, 30 and factors such as poor cognition, lower income and longer disease duration were associated with medication non-adherence, while higher education, living with a spouse and being female were positively associated with adherence. 31 A few other studies have explored the lifestyle domains of SMBs, and specifically regular engagement in physical activity. They found that lack of time, low energy, physical symptoms and the fear of falling were the most frequently reported barriers for all types of exercise, while being male, married and enjoying exercise were positive predictors.32–34
Identifying socio-clinical determinants of SMBs and patient activation is important because it may provide data needed to develop programs that effectively support SMBs and activation. Although socio-clinical determinants are not always modifiable, acknowledging their impact may contribute to a more specific and targeted program. For example, if cognitive decline is associated with reduced engagement in SMBs, it may be useful to include patients’ caregivers in the support program.
As the base of knowledge in PD about the contribution of socio-clinical factors to SMBs is limited, and there is no current knowledge about the contribution of these factors to patient activation, the goal of the current study was to identify socio-clinical factors that associated with specific SMBs and patient activation among PwP. Specifically, we specifically aimed to test the association between socio-clinical factors (that include age, gender, cognitive status, comorbidities, disease severity [motor and non-motor symptoms] and social support) and SMBs (including utilization of rehabilitative treatments, physical activity and patient activation). In addition, we explored the use of regression tree to find the cut-off levels of the socio-clinical factors, which are associated with lower or higher SMBs and patient's activation.
Based on the available reports from research on PD and other chronic conditions, we hypothesized that PwP, who are younger, do not suffer from cognitive decline, have fewer comorbidities, have low disease severity and high family support, will show higher engagement in SMBs, including utilizing rehabilitative treatment and physical activity and will show a higher level of patient activation.
Methods
This was a cross-sectional study with convenience sampling.
Study population
PwP were recruited from the Movement Disorders Institute in the Department of Neurology at the Rambam Health Care Campus in Haifa. Patients were included in the study if they were diagnosed with PD without severe cognitive decline (Mini-Mental State Exam [MMSE] score of more than 20). The ethics committees of the University of Haifa and Rambam Health Care Campus approved the study. All participants provided written informed consent.
A sample size calculation conducted by GPOWER version 3.1.9, based on one-tail correlation, indicated that a sample of 66 respondents would be sufficient to reach a value of r ≥ 0.4, with a statistical power of 0.85 and α = 0.01.
Procedure
Patients attending their routine visit at the Movement Disorders Institute were screened for eligibility by the treating neurologist. Eligible patients were given a short explanation about the study procedure and were invited to participate in a one-hour session consisting of an interview and assessments conducted by a trained research assistant. Data about the disease and comorbidities were retrieved from electronic medical records.
Research tools
The independent study variables were socio-clinical factors that included age, gender, cognitive status, comorbidities, severity of motor and non-motor symptoms and family and social support. Cognitive status was evaluated by the MMSE. 35
A screening test comprising of 11 items evaluates orientation to time and place, attention/concentration, short-term memory (recall), language skills, visuospatial abilities and ability to comprehend and follow instructions, with scores of >24 being considered within the normal range. 35 Comorbidities were assessed using the Charlson Comorbidity Index. 36 It assesses the comorbidity level by taking into account both the number and severity of 19 pre-defined comorbid conditions and provides a weighted score of the participant's comorbidities. Higher scores represent a greater burden of comorbid conditions.. 36 The disease severity of the motor symptoms was assessed by the motor part of the Unified Parkinson's Disease Rating Scale (MDS-UPDRS). 37 The UPDRS is a widely used scale for assessing both motor and non-motor aspects of Parkinson's disease. In the present study, we utilized Part 3, which focuses on the motor examination of PD motor signs. 37 Scores on this section of the UPDRS range from 0 to 132, with higher scores indicating greater severity of motor symptoms.
The non-motor symptoms were assessed by the 30-item self-report Non-Motor Symptoms Questionnaire (NMSQ). 38 This is a 30-item patient-reported screening questionnaire. Non-motor symptoms are categorized into nine domains: gastrointestinal, urinary, sexual, cardiovascular, apathy/attention/memory, hallucinations/delusions, depression/anxiety/an-hedonia, sleep/fatigue and miscellaneous. Each item is scored as either ‘yes’ or ‘no’. Higher scores indicate a higher burden of non-motor symptoms. 38 Social and family support was assessed with the Multidimensional Scale of Perceived Social Support. 39 This is a 12-item scale that assesses the support of significant others, family and friends on a 7-point Likert scale. The scores range from 0 to 49, and higher scores indicate greater social and family support. 39
Parkinson's disease-related aspects of SMBs included utilization of rehabilitative treatments, physical activity and patient activation. Utilization of rehabilitative treatments was assessed by asking the participants about the frequency of physical therapy, occupational therapy and speech and language pathology treatments during the past year. Physical activity level was assessed by the International Physical Activity Questionnaire–Short version (IPAQ-Short). 40 The IPAQ is a commonly used, self-report questionnaire of time spent in four categories of physical activity (i.e., vigorous, moderate, walking and sitting) during the last seven days. Scores are interpreted as total physical activity in metabolic equivalent units (METS) in the last seven days. Patients’ activation was assessed by the Patient Activation Measure (PAM-13). 41 The PAM-13 is a self-reported, validated and licensed tool to measure a patient's knowledge, skills and confidence for self-management. 41 We used a validated, licensed Hebrew version of the PAM-13 supplied by Insignia Health https://www.insigniahealth.com/products/pam-survey). It consists of 13 statements rated on a four-point Likert scale of level of agreement. The PAM-13 score is transformed into a 0–100 continuous scale according to a licensed conversion table (Insignia Health). 42 The overall score captures the extent to which people feel engaged and confident in taking care of their health conditions, with higher scores indicating stronger activation. 41 Based on their PAM-13 score, people are divided into four ordinal levels of activation. Level 1 represents patients who tend to be passive and feel overwhelmed managing their own health, while level 4 represents patients who have attitude, knowledge and skills that are important for self-management.
Statistical analysis
Continuous variables were represented as means with standard deviations, and discrete variables as absolute and relative numbers.
Spearman's correlation was used to evaluate the strength of the relationship between the specific SMBs, patient activation and socio-clinical factors. Factors that significantly correlated with the outcomes of SMBs including the severity of non-motor symptoms, family and social support, number of non-motor symptoms and cognitive status, were entered into a linear stepwise regression analysis for physical activity and for patient activation (i.e., the outcome measures). The inclusion criteria for the regression models were based on Schwarz Bayesian information criterion.43,44
A machine learning regression tree analysis was conducted as an exploratory investigation of cut-off levels of the socio-clinical factors, which associate with lower or higher SMBs and patient's activation. To that end, we used the party R package 45 with random forest variable selection and Monte Carlo simulation for multiple testing adjustment. 46 Potential explanatory variables for the tree were the same as for the linear regression. Roughly, the algorithm works as follows: (1) Test the global null hypothesis of independence between any of the input variables and the response (mean of PAM score, mean of total IPAQ). Stop if this hypothesis is rejected. Otherwise, select the input variable with the strongest association to the response. The strength of the association is measured by a p-value corresponding to a test between a single input variable and the response; (2) Implement a binary split in the selected input variable and (3) Recursively repeat steps 1 and 2. The corresponding p-value must be less than .05 to implement a split. The potential explanatory variables for each split were the remaining variables. A regression tree model can define the mean level of the dependent variable based on exploring interactions between potential independent variables. 47 This statistical approach is not constrained by model assumptions. 48
The IPAQ score was highly skewed therefore it was normalized using square root. The square root IPAQ score was used in the linear regression and the regression tree analysis to maintain consistency between the procedures. Therefore, the decision tree presents the value of the square root of the IPAQ.
The R Foundation for Statistical Computing version (4.0.5) software was used for all the analyses.
Results
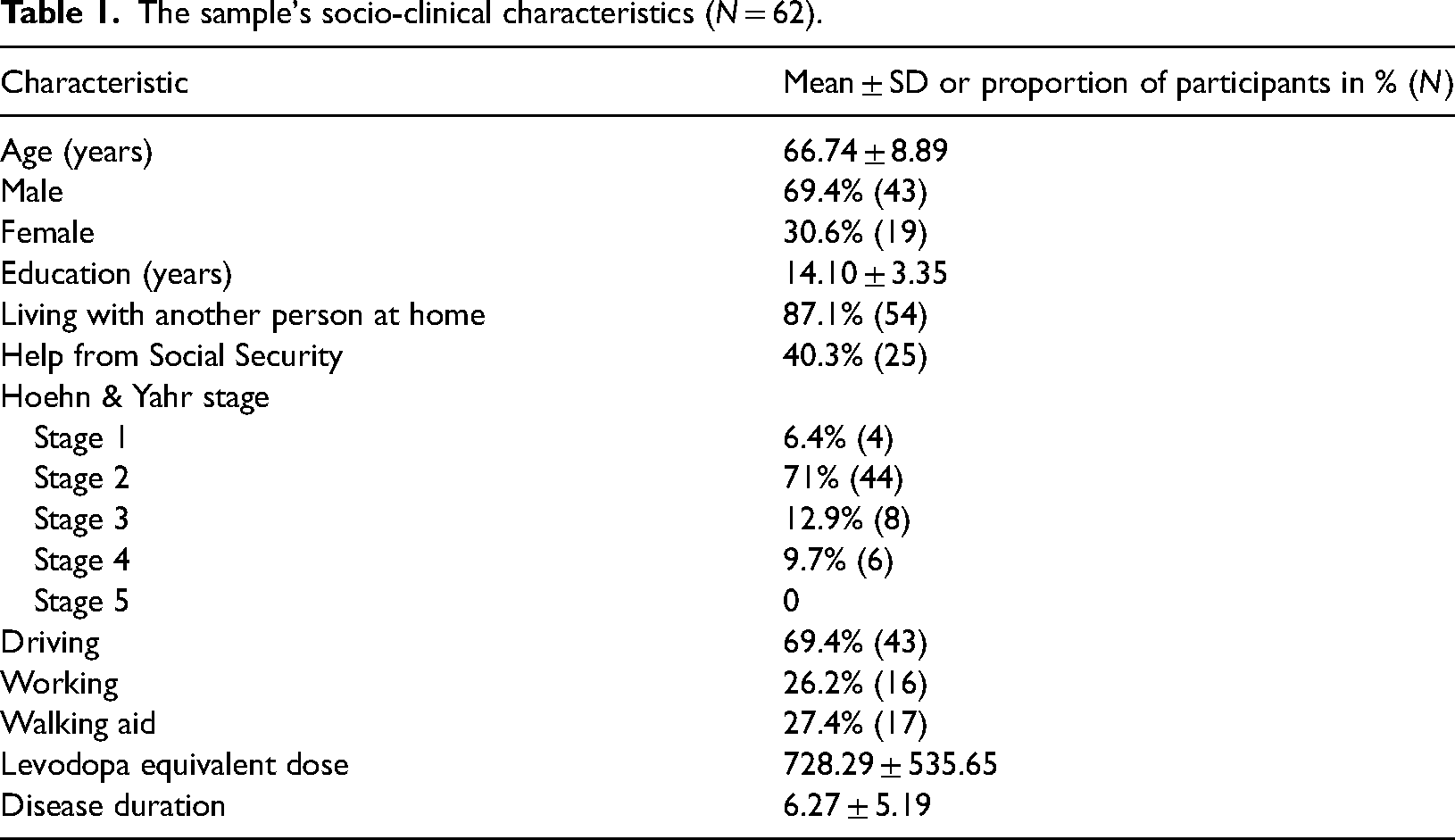
The study population included 62 PwP of whom 43 were men and 19 were women. The mean age was 66.74 ± 8.89 years, and the mean Hoehn & Yahr stage was 2.13 ± 0.81. Table 1 presents the sample's demographics and disease-related characteristics.
The sample's socio-clinical characteristics (N = 62).
The descriptive statistics of the model variables are presented in Table 2.
Descriptive statistics of the models’ variables.
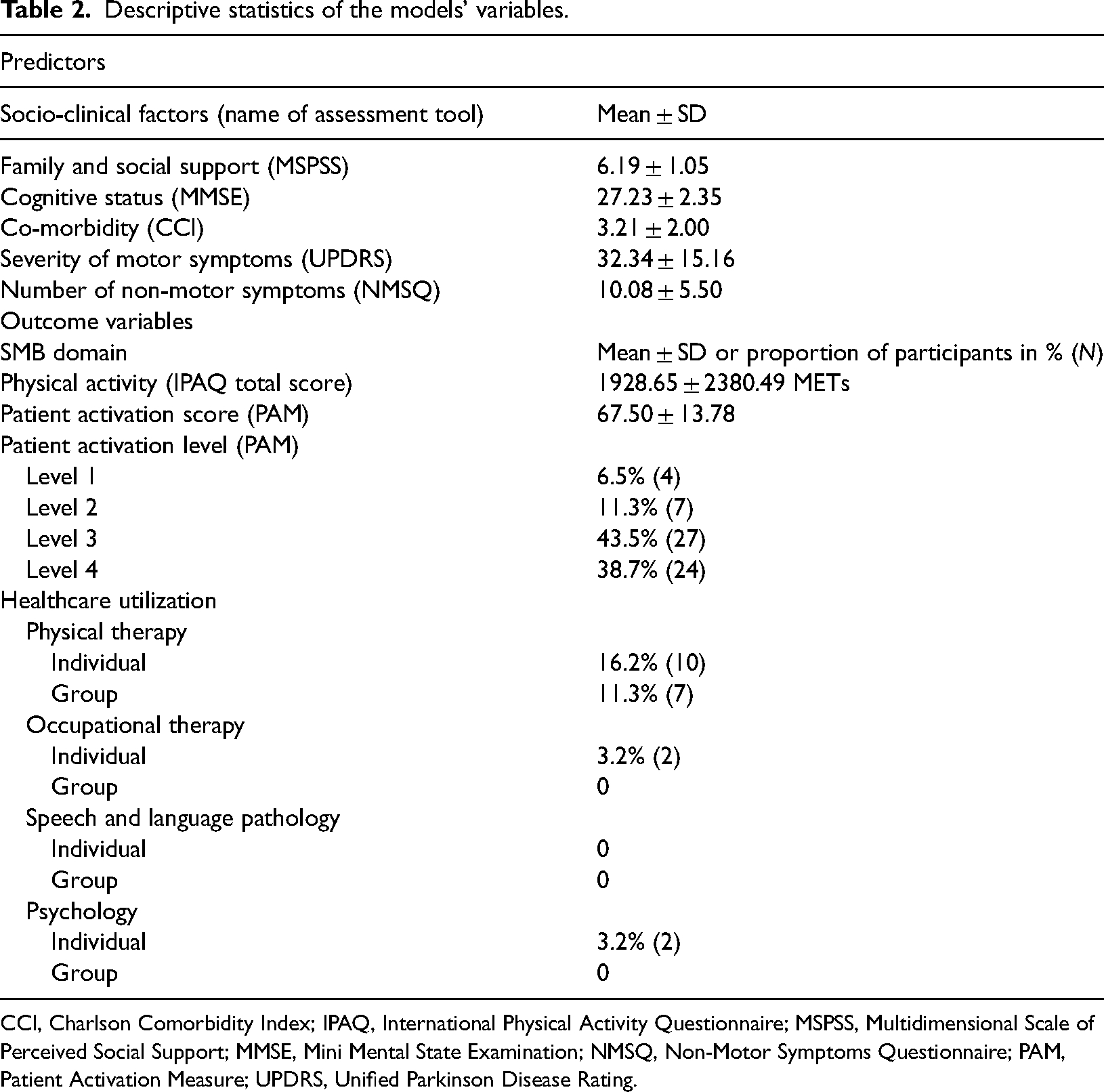
CCI, Charlson Comorbidity Index; IPAQ, International Physical Activity Questionnaire; MSPSS, Multidimensional Scale of Perceived Social Support; MMSE, Mini Mental State Examination; NMSQ, Non-Motor Symptoms Questionnaire; PAM, Patient Activation Measure; UPDRS, Unified Parkinson Disease Rating.
Utilization of healthcare services by the study participants was very low. Therefore, this variable was not included in the regression analyses.
Correlations between the study variables
Table 3 presents the correlations between the study variables. The level of physical activity was significantly correlated with family and social support (r = 0.30, p = .01); with cognitive status (r = −0.47, p < .001); and with the number of the non-motor symptoms (r = −0.37, p = .003). The level of patient activation was significantly correlated with family and social support (r = 0.51, p < .001); with the number of non-motor symptoms (r = −0.30, p = .01); and with the severity of the motor symptoms (r = −0.49 p < .001).
Correlations between the study variables.
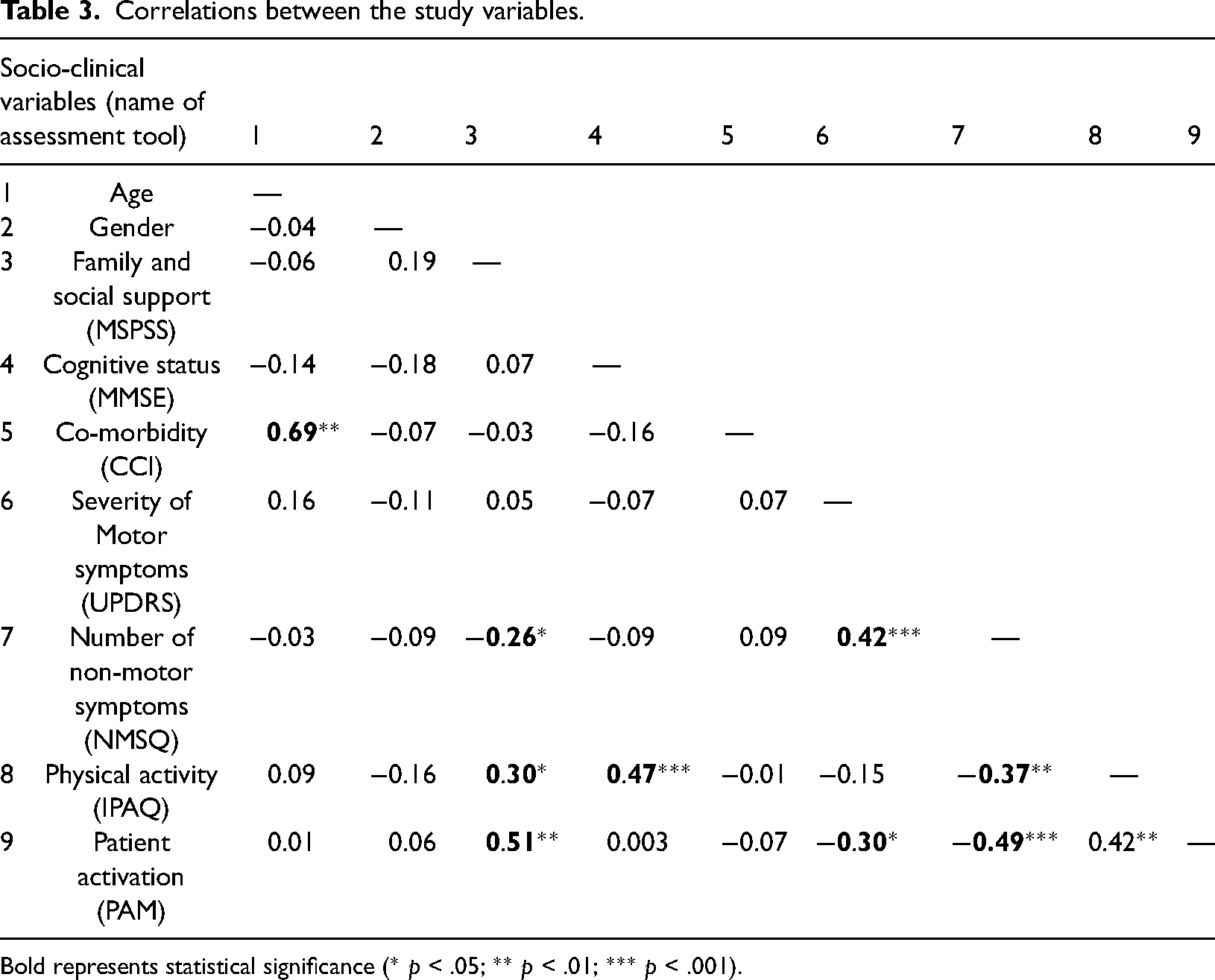
Bold represents statistical significance (* p < .05; ** p < .01; *** p < .001).
Linear stepwise regression analysis
Linear stepwise regression analysis (Table 4) explained 35% of the total variation of the IPAQ score and was statistically significant (R2 = 0.35, F(3, 58) = 10.50, p ≤ .001). It was found that low values of NMSQ (B = −1.37, p ≤ .01) and high values of MMSE (B = 4.70, p ≤ .001) increased the IPAQ score significantly.
Stepwise Regression Analyses results for the mean root square IPAQ score, N = 62.
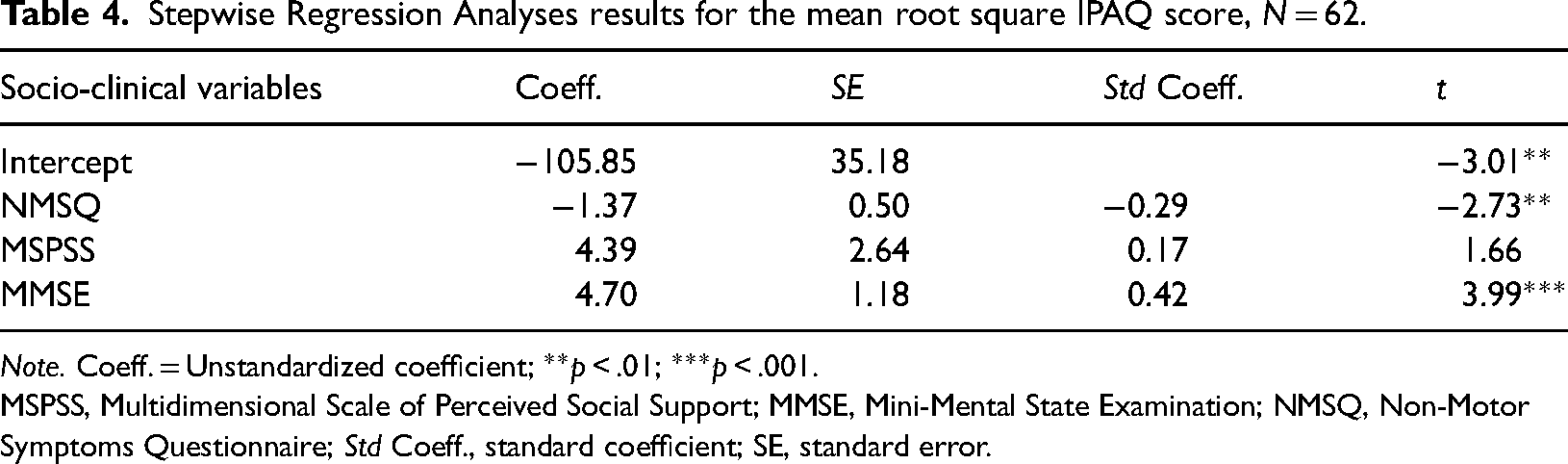
Note. Coeff. = Unstandardized coefficient; **p < .01; ***p < .001.
MSPSS, Multidimensional Scale of Perceived Social Support; MMSE, Mini-Mental State Examination; NMSQ, Non-Motor Symptoms Questionnaire; Std Coeff., standard coefficient; SE, standard error.
Linear stepwise regression analysis (Table 5) explained 30% of the total variation of the PAM score and was statistically significant (R2 = 0.30, F(1, 30) = 25.88, p ≤ .001). It was found that low values of NMSQ increased the PAM score (B = −1.37, p ≤ .001).
Stepwise Regression Analyses results for the PAM score, N = 62.
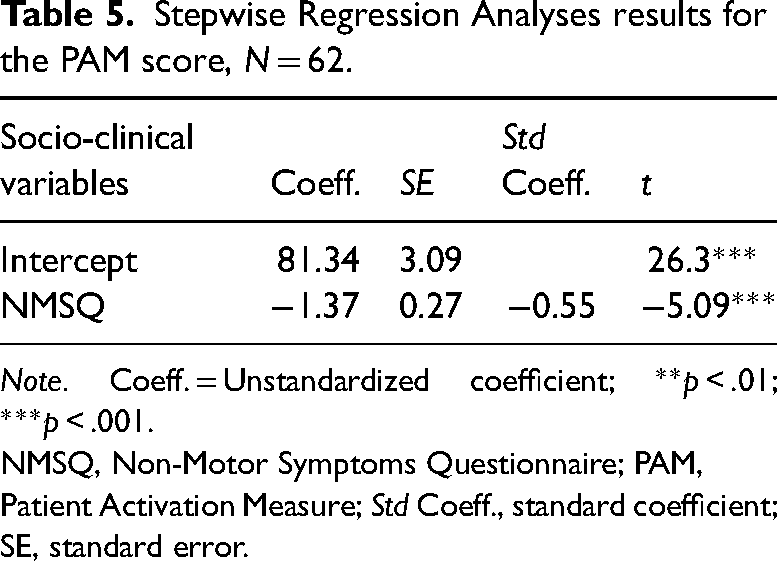
Note. Coeff. = Unstandardized coefficient; **p < .01; ***p < .001.
NMSQ, Non-Motor Symptoms Questionnaire; PAM, Patient Activation Measure; Std Coeff., standard coefficient; SE, standard error.
Regression tree analyses
The regression tree analysis for the mean square root IPAQ score is presented in Figure 1. The analysis revealed a significant split in the MMSE variable such that patients with a score below or equal to 24 showed a relatively low IPAQ score. Patients who had a MMSE score between 24 and 29 had a moderate IPAQ score, and patients who had a MMSE score above 29 had a relatively high IPAQ score.
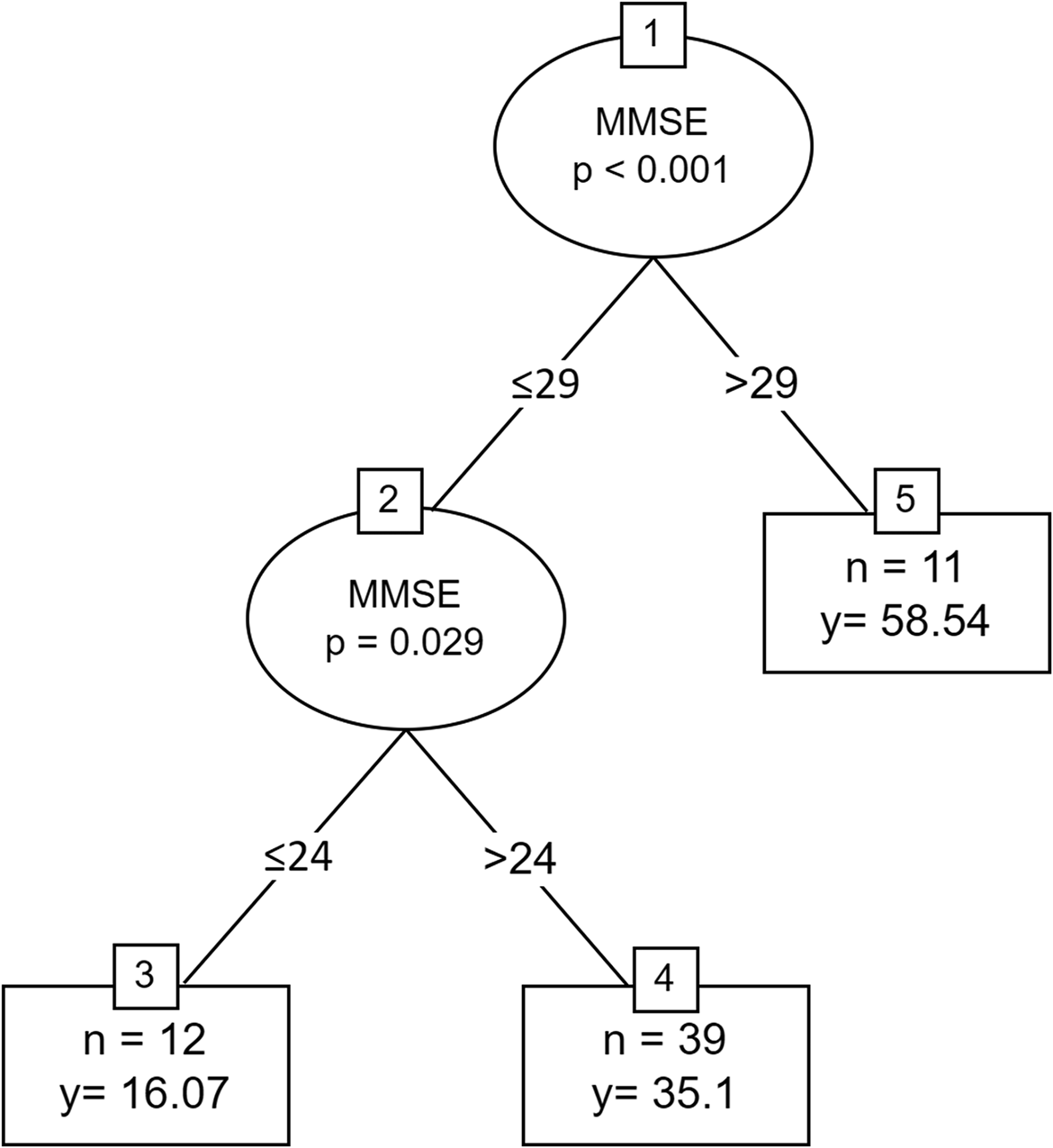
Regression tree for root mean square IPAQ score. y = mean square root of IPAQ score. IPAQ, International Physical Activity Questionnaire; MMSE, Mini-Mental State Examination.
The regression tree analysis for mean PAM score is presented in Figure 2. The analysis revealed a significant split in the NMSQ variable such that patients with a score below or equal to 5 showed a relatively high PAM score. Patients who had a NMSQ score above 5 and a UPDRS-motor part score below or equal 45 had a moderate PAM score, and patients who had a NMSQ score above 5 and a UPDRS-motor part score above 45 had a relatively low PAM score.
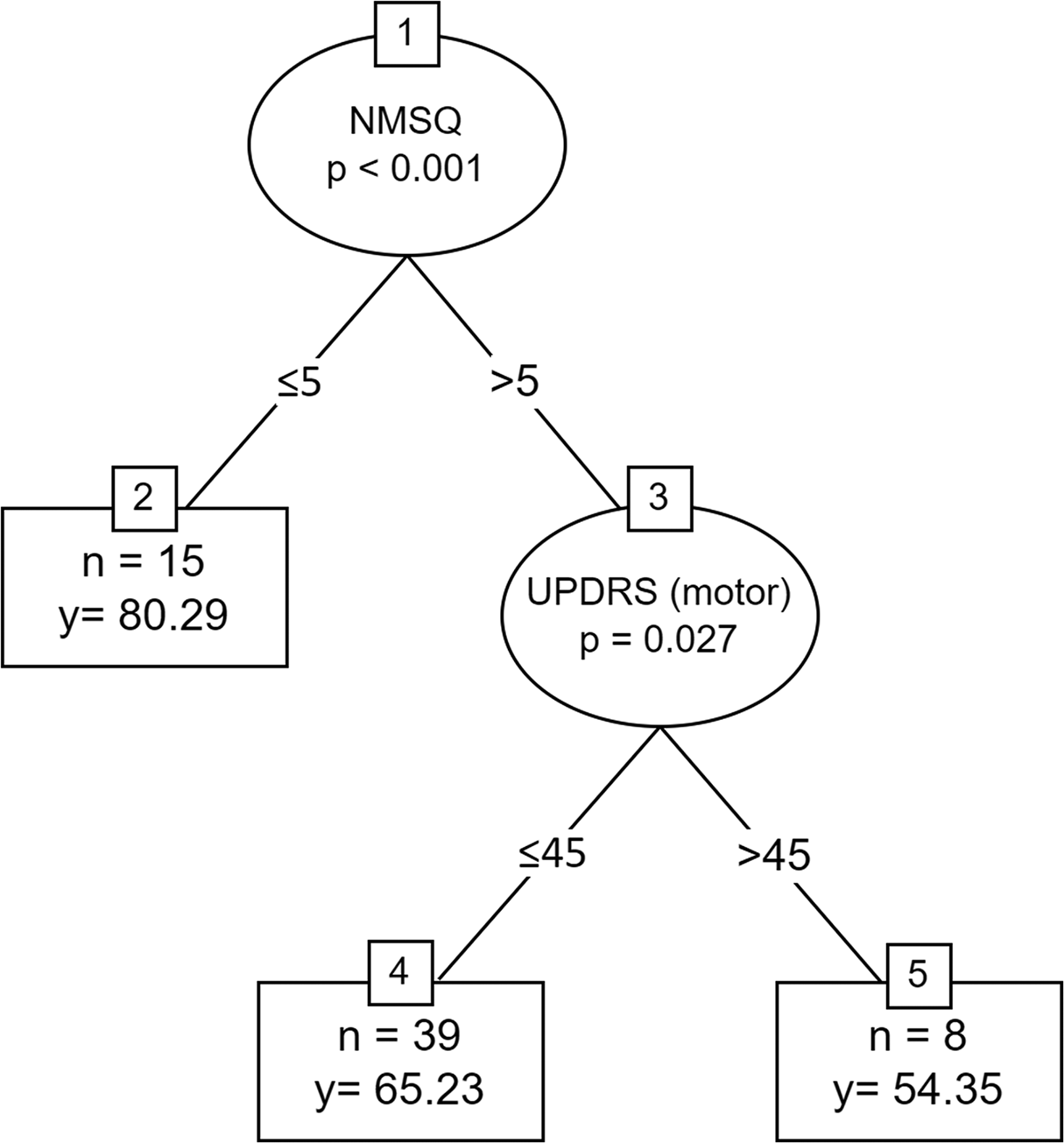
Regression tree for PAM score. y = mean PAM score. PAM, Patient Activation Measure; NMSQ, Non-Motor Symptoms Questionnaire; UPDRS, Unified Parkinson Disease Rating.
Discussion
Overall, the study sample consisted of PwP in the mid-stage of the disease, with preserved cognitive status, a low number of co-morbidities and high social support. The number of non-motor symptoms was within the middle of the range previously reported for PwP. 49
As for the dependent variables, our sample was engaged in physical activity at a moderate mean level (1876.74 ± 2127.04 MET-min./week). 32 This is similar to the level of physical activity previously reported in PwP in an Australian cohort (1823.6 ± 1693.6 MET-min./week). 33 The majority of participants in our sample were at PAM levels 3 or 4, indicating high activation. This result is similar to other chronic diseases such as cancer, diabetes mellitus and asthma. 6
We found that among the socio-clinical factors that were hypothesized to associate with the domains of SMBs, cognitive status, number of non-motor symptoms and to a lesser degree the severity of motor symptoms, are the prominent explanatory variables of engagement in physical activity and patient activation. PwP with better cognitive status and fewer non-motor symptoms showed higher engagement in physical activity, and PwP with fewer non-motor symptoms showed better patient activation. Accordingly, these results indicate that in PD, disease-specific clinical characteristics overshadow other personal factors (e.g., family support) as determinants of SMBs. In addition, the novel contribution of the current study is the finding of an association between socio-clinical factors and PwPs’ activation.
Most PwP suffer from non-motor symptoms, and the average number of these symptoms per patient range from 4 to 19. 49 In recent years, the contribution of non-motor symptoms in PD to the overall disease burden and to patients’ quality of life has been acknowledged.49,50 Moreover, Martinez-Martin et al. 51 found that non-motor symptoms had a larger contribution to quality of life of PwP than motor symptoms. Our findings are aligned with this report, and extend the notion of the importance of non-motor symptoms to aspects of self-management (i.e., physical activity). Furthermore, concerning patient activation, the results show that when the number of non-motor symptoms is low, patient activation is relatively high (i.e., patients hold attitudes and skills that promote and maintain their health, PAM level 4), and the severity of motor symptoms is not a determinant of activation. In contrast, when patients manifest more than five non-motor symptoms, the severity of their motor symptoms significantly contributes to the level of patient activation, i.e., a UPDRS motor score of 45 distinguishes between PwP with PAM levels 3 and 2.
Using the MMSE in the current study, we were also able to specifically focus on the role of the patients’ cognitive status concerning SMBs and patient activation. The MMSE provides more detailed information about patients’ cognitive function than the cognitive-related items in the NMSQ. Our findings highlight the importance of cognitive function to SMBs. Cognitive status was associated with engagement in physical activity and was the only important variable in the physical activity tree model. The split value of the MMSE was 29 on first node and 24 on the second node. The two split values on the MMSE (i.e., less than fully normal cognition, and less than 24 which is the common cut-off score for differentiation between patients with normal cognition and those with mild cognitive impairment), 52 suggest that even a mild change in cognition can affect the adoption of a healthy lifestyle. Furthermore, this finding supports the notion that maintaining SMBs (such as engagement in physical activity) requires cognitive skills such as problem solving, decision making and taking action 53 and with the presence of cognitive decline, the ability to preserve engagement in SMBs may be reduced. This finding is supported by previous studies in diabetes that used the MMSE for the cognitive evaluation and showed that cognitive function is related to SMBs.54–57 Furthermore, Sinclair et al. 54 found that people with diabetes with an MMSE score of <23 were significantly less likely to be involved in diabetes self-care and diabetes monitoring than those without cognitive impairment.
We found that many patients do not utilize rehabilitative treatments. For instance, only 16.2% utilized physical therapy at all. Among the services we recorded, physical therapy had the highest utilization rate, and hydrotherapy, occupational therapy and speech and language pathology had substantially lower rates. The percentage for physical therapy is lower than that reported in other countries, which ranged from 14% in the U.S. to 60% in the Netherlands.58–61 Personal and healthcare system barriers may explain the low utilization; however, such analysis requires a larger sample. A SWOT analysis was performed in a recent study to determine factors that may hinder PwP from utilizing OT treatments. 62 For that, occupational therapists and neurologists answered a survey. The findings suggested that patients’ and physicians’ limited acquaintance with OT was a threat, followed by low referral rates for treatments. Unawareness of the benefits of rehabilitation treatments may not be the only explanation. Other barriers may include the low availability of some rehabilitative services for PwP (e.g., Speech and language pathology63–65) and limited accessibility (e.g., remote clinics, inadequate public transportation or dependency on others for transportation). 62
The current research findings have some important clinical implications. First, they suggest that to promote physical activity and patient activation there is a need to identify and treat the non-motor symtoms of PD. This implication is important because the non-motor symptoms are often neglected. 66 Important insights for the development of self-management support programs is the need to incorporate specific strategies to cope with the burden of the non-motor symptoms and the cognitive decline. For example, self-management programs may include education about common non-motor symptoms and possible coping strategies and may integrate caregivers of patients with cognitive decline.
This study has few limitations. The sample size was relatively small and represents a section of PwP who have mid-stage disease characteristics. Our participants were recruited from a Movement Disorder Institute and thus were likely to be already more active in managing their care and had a stronger social support. This may limit the generalizability of the study findings.
Also, the current study examined only specific aspects of SMBs. The ON/OFF periods were not formally documented, but all meetings with the participants took place during the morning hours when participants visited the movement disorder clinic and were able to perform the testing procedure. In addition, levodopa-induced complications such as dyskinesias were not specifically recorded. Future research can consider these factors in the regression analysis. The theoretical concept of self-management encompasses a wide range of behaviours, therefore, in order to fully understand the contribution of personal factors to engagement in SMBs, further studies should explore other aspects of SMBs that were not studied in the current study.
Conclusions
Our study joins a growing body of knowledge that emphasizes the role of non-motor symptoms in various aspects of PwP life. Specifically, the number of the non-motor and to a lesser degree the severity of motor symptoms is prominent exploratory variables of patient activation. In addition, cognitive status is a prominent exploratory variable of physical activity. Self-management support programs need to incorporate specific strategies to cope with the burden of the non-motor symptoms and the cognitive decline.
Footnotes
Acknowledgements
The authors are grateful to the study participants for their generous time when participating in this study.
Contributorship
GYS and MK conceived the study design. IS, MN and RH recruited subjects and MAT and MD performed the measurements. IS and IE were responsible for project administration. MK, GYS and MAT analyzed the data and drafted the manuscript with inputs from all co-authors. IS, MN and RF contributed to the critical revision of the manuscript. GYS, MK and IS supervised the study. All authors read and approved the final.
Declaration of conflicting interests
The author(s) declare the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Ethical approval
Ethical approval for this study was obtained from the Ethics Committee of the Faculty of Social Welfare & Health Sciences, University of Haifa (approval number 471/18) and was also approved by the Helsinki committee of Rambam Health Care Campus (Application number 0067-19-RMB).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Faculty of Social Welfare & Health Sciences, University of Haifa and Rambam Health Care Campus under Grant 10/12-83. This work was supported by the Center for Research and Study of Aging, Faculty of Social Welfare & Health Sciences, University of Haifa.
Guarantor
Michal Kafri
Informed consent
Written informed consent was obtained from all subjects before the study.