
Abstract
Insight into the current status of long-term care facilities (LTCFs) and chronic diseases in underdeveloped areas in China is scant. Using a census method to survey older adults ≥60 years old (154 older adult residents) in all LTCFs in Jishou area. The International Resident Assessment Instrument for Long-Term Care Facilities (interRAI-LTCF) was used to collect information and analyze the current status of chronic diseases among older adult residents. There were 62 187 residents ≥60 years old in Jishou area. According to the survey, there were only 154 older adult residents living in the LTCFs of Jishou, with a ratio was 0.3% of all older adult residents, which was much lower than China’s 3.0%. Of respondents (109 older adult residents), the prevalence of chronic diseases was 70.6%. The prevalence increases with age, as well as in the female is higher than in the male. The top 3 chronic diseases were hypertension (41.3%), bone and joint disease (12.8%) and cerebrovascular disease (12.8%). It was found that different age groups and genders lead to differences in the prevalence and the order of chronic diseases. The prevalence of older adults with impaired balance ability, sleep disturbance and swallowing disturbance was higher than that of normal older adults. The results of the one-way analysis of variance showed that the age and balance ability of the older adults with chronic diseases were statistically significant (P < .05). In addition, the prevalence of chronic diseases in the LTCFs older adult was higher than the home care (HC) older adults in Jishou. The age and the prevalence of chronic diseases of LTCFs in older adults with professional nursing staff were higher than in those without. This study provides a theoretical basis for the healthcare distribution, prevention and treatment of chronic diseases in underdeveloped areas. The undeveloped area has lower LTCFs staying rate and chronic disease prevalence of older adults than relatively developed areas. More public health attention and capital investment are needed to increase the LTCFs number and strengthen disease testing and screening. As well as, the proportion of professional nursing staff and specialist doctors in LTCFs and improve the quality of care and medical treatment for older adults.
China’s disease surveillance has mainly concentrated on economically developed areas, with less surveillance in remote and impoverished areas.
Using a census method to survey older adults ≥60 years old in all LTCFs in Jishou area, analyze the current status of chronic diseases among older adult residents.
Investigating the current status of chronic diseases in the older adult population in Jishou area can compensate for the lack of an understanding of the current status of chronic diseases in older adults, which is of great significance for understanding the current status of chronic diseases in older adults in similar areas in China.
Introduction
Ensuring health services for older adults is a difficult problem that society needs to face and solve. The population of China has been aging since 1999. As the aging of the population further intensifies, chronic diseases have become a major public health problem. The World Health Organization 1 pointed out that chronic diseases accounted for 71% of all deaths and 88.5% in China. 2 The social economy, population types, medical resources, and topography of various regions in China are different, 3 which causes the prevalence of chronic diseases to varying from place to place.4-9 Jishou, Western Hunan area is a poor region in Central China with multiple ethnic groups, a high proportion of older adults 10 and large differences in medical skills. 11 Jishou is one of the key regions supported by the Healthy China 2030 plan. However, China’s disease surveillance has mainly concentrated on economically developed areas, with less surveillance in remote and impoverished areas. 12 Investigating the current status of long-term care facilities (LTCFs) and elderly chronic diseases in Jishou area can provide a theoretical basis for the prevention and treatment of chronic diseases in underdeveloped areas.
Wang et al 12 surveyed the health status of 31 provinces in mainland China, and the results showed that the prevalence of chronic diseases in older adults was 75.8% in 2013. The current status of chronic diseases in older adults in parts of China, such as Shanghai,4,5 Shandong, 13 Lanzhou City, 6 Nanjing City, 7 Qiannan ethnic area, 9 and Beijing Haidian District, 8 has been studied. The results showed that the prevalence of chronic diseases in older adults varies among regions. Zhou et al found that individuals living in economically developed areas usually have increased risks of various diseases, while the better medical services present in these areas significantly reduced the burden of diseases. 14
“Promoting the Combination of Medical Care and Nursing Care” is the health support system under the “Healthy China 2030 plan” in China. Underdeveloped areas similar to Jishou will be the most difficult and final areas for those policies to be implemented. In the present study, we investigated the current status of all LTCFs and the chronic diseases among their residents in Jishou, China. The different characteristics of older adults, such as age, gender, etc., were grouped to explore the influencing factors of chronic diseases. Moreover, chronic diseases in the undeveloped and relatively developed areas in China were compared and discussed. This work is the first to apply the internationally widely used International Resident Assessment Instrument (interRAI) tool to the health research of underdeveloped areas in China.
Methods
Study Design and Participants
This cross-sectional study was conducted between March 2021 and September 2021. A census method was used to survey older adults ≥60 years old in all LTCFs (2 LTCFs with professional nursing staff and 7 LTCFs without professional nursing staff) in Jishou, Western Hunan, China. These inclusion/exclusion criteria were validated for the application of the interRAI in China. 15 (1) Inclusion criteria: age ≥60 years old, clear awareness and barrier-free communication, the provision of informed consent, and willingness to participate in this study. (2) Exclusion criteria: people who were unconscious or unable to communicate and those who suffered from Alzheimer’s disease, mental disorders or terminal diseases. There were 154 residents living in all LTCFs. According to the inclusion and exclusion criteria, 45 residents were excluded due to age, unconsciousness, etc. Therefore, the final sample included 109 older adult respondents (Figure 1).
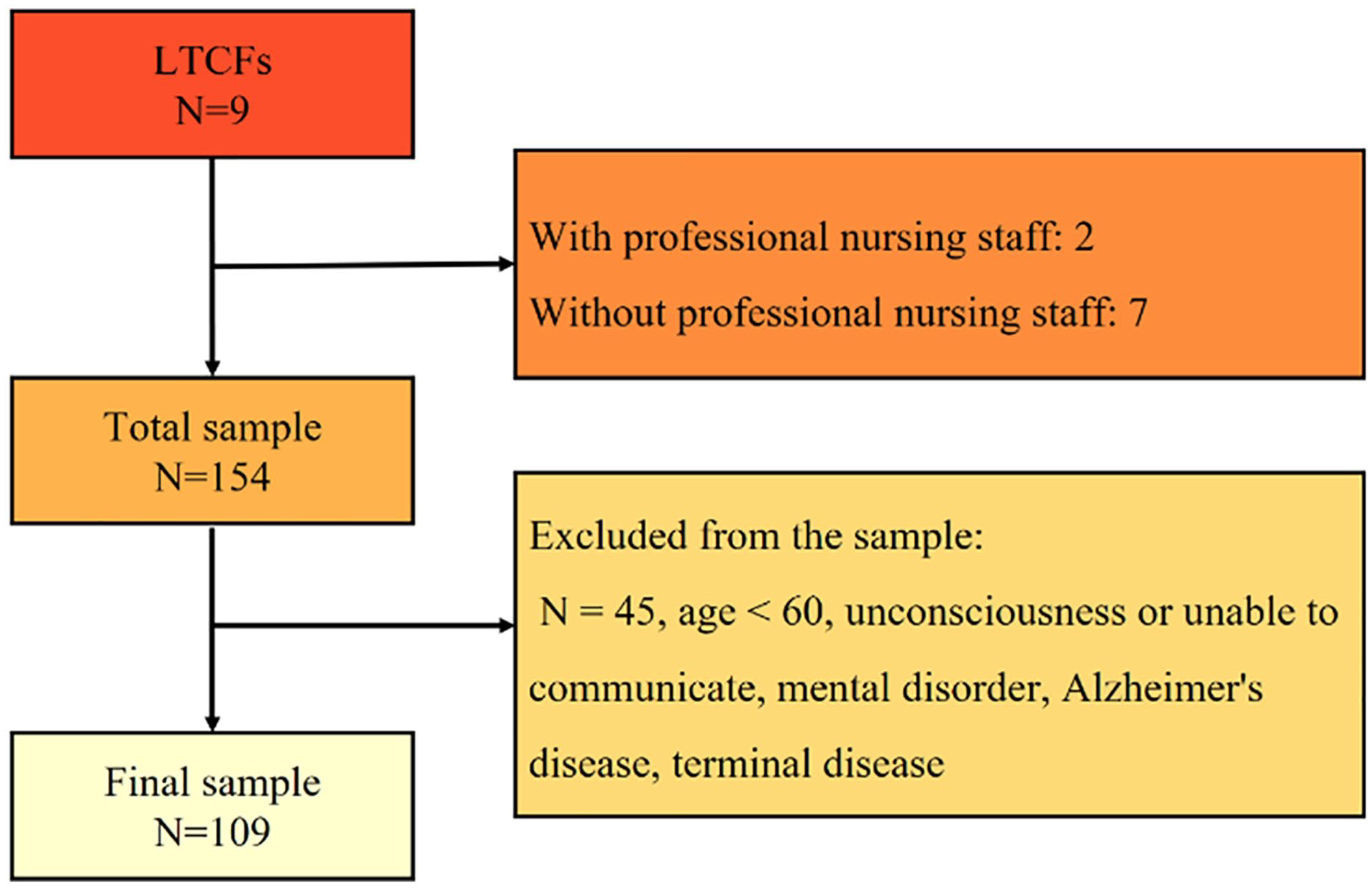
Assembly of the study sample.
The International Resident Assessment Instrument for Long-Term Care Facilities (interRAI-LTCF) has good reliability and validity,16-18 which is widely used in LTCFs older adults’ health research. Meanwhile, the interRAI has been applied in communities19-21 and LTCFs in China.22-24 InterRAI-LTCF assessment scale includes basic information and 14 dimension assessment of older adults, which are respectively cognition, communication and vision, mood and behavior, psychosocial well-being, functional status, continence, disease diagnosis, health conditions, oral and nutritional status, skin condition, activity pursuit, etc. In this study, the dimension of disease-related module information in interRAI-LTCF was selected as the survey tool, and it was approved by the interRAI and interRAI China. After obtaining the consent of the respondents, surveyors conducted face-to-face interviews using paper questionnaire surveys with the assistance of institutional management or nursing staff. Each questionnaire was collected on-site and reviewed by 2 surveyors to add missing items promptly. A total of 109 questionnaires were distributed, and 109 valid questionnaires were returned. The questionnaire response rate was 100%. The reporting of this study conforms to STROBE guidelines. 25
LTCFs Status
Jishou area includes 1 city and 5 towns. There were 408 812 residents in Jishou, of whom 62 187 residents were aged 60 and above. 26 Our work found that there were only 9 LTCFs in Jishou area, including 3 LTCFs in urban areas and 6 LTCFs in rural areas. The Jishou area includes 2 LTCFs with professional nursing staff (Xiangxi Social Welfare Home, Xiangxi Second Social Welfare Institute) and 7 LTCFs without professional nursing staff. The staying rate of the older adult population in Jishou LTCFs was 0.3% (for urban LTCFs, it was 0.2%, and for rural LTCFs, it was 0.5%); see Table 1.
LTCFs Status.

Statistical Analysis
We used IBM SPSS Statistics for Windows, Version 25.0 (IBM Corp., Armonk, NY, USA) for data sorting and analysis. The enumeration data such as gender was expressed as a proportion ratio or rate. The measurement data such as age were expressed by the mean ± standard deviation. The difference between the 2 groups was analyzed by one-way analysis of variance. A P value of <.05 was considered statistically significant.
Results
Different Characteristics of Older Adults and the Prevalence of Chronic Diseases
A total of 109 residents aged ≥60 years were included in the study, including 76.2% males and 23.9% females. The age range was 60 to 100 (75.76 ± 8.95) years old, 44% of residents had unmarried residents, 80.7% of residents had medical insurance, and 58.7% of residents lived alone before admission. Body mass index (BMI) was classified according to the Chinese guidelines for the criteria of weight for adults 27 : 29.4% of residents were overweight or obese (>24.0 kg/m2; see Table 2). In addition, the older adult had varying degrees of sensory impairment. The results showed 23.6% of residents with impaired balance ability and 26.6% of residents with sleep disturbance.
Different Characteristics of the Older Adult and the Prevalence of Chronic Diseases.
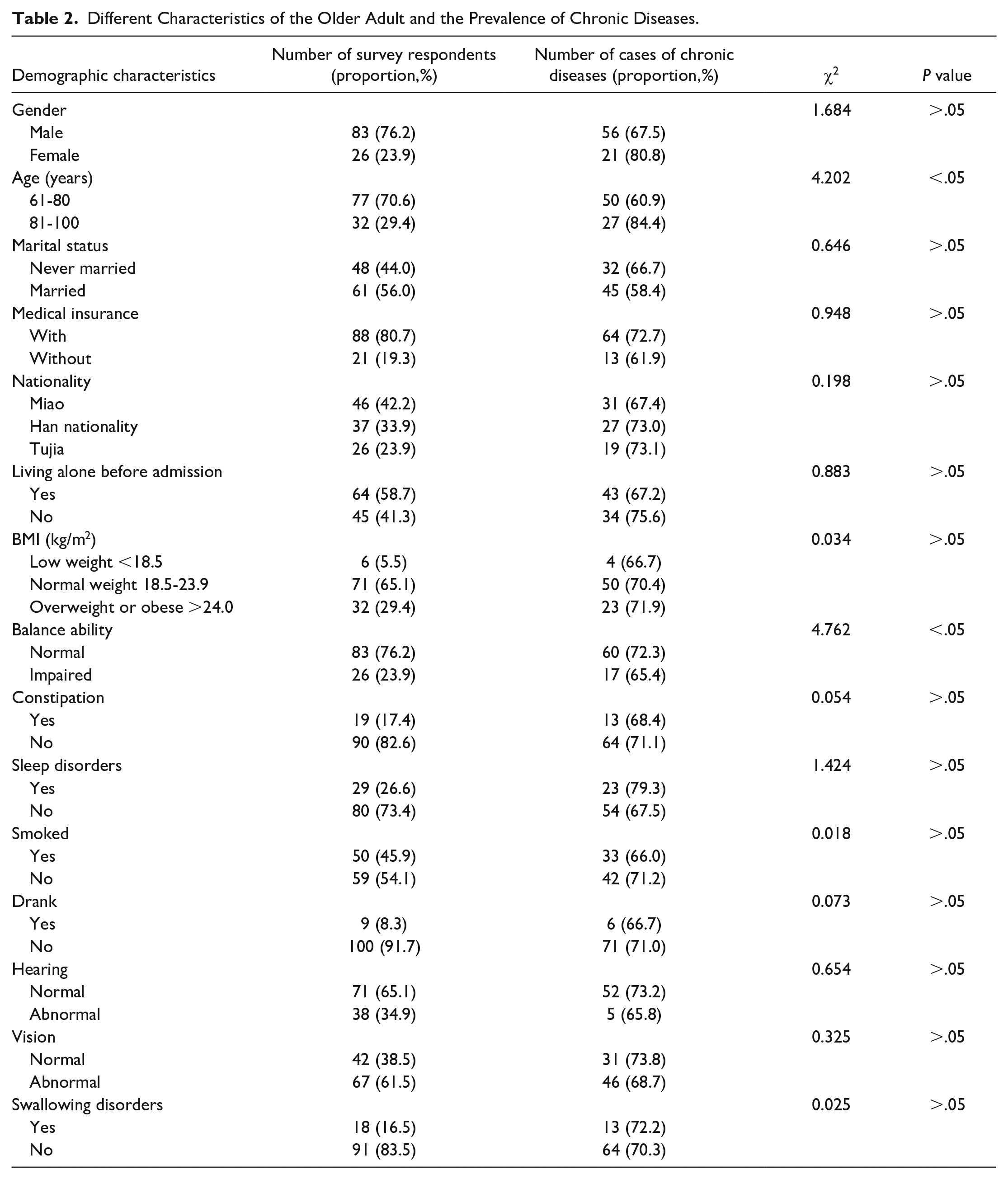
Table 2 shows that the prevalence of chronic diseases increased with age, the prevalence of the female older adult was higher than that of the male. The prevalence of older adults with medical insurance was higher than those without medical insurance. It is worth noting that older adults with impaired balance ability, sleep disorders, and swallowing disorders had a higher prevalence of chronic diseases.
The prevalence of chronic diseases by different characteristics was compared using a one-way analysis of variance. The results showed that chronic disease was statistically significant in older adults with age and balance ability (P < .05).
Current Status of Chronic Diseases
The prevalence of chronic diseases was 70.6%; the prevalence of chronic diseases in females was 80.8% versus 67.5% in males. In the older adult population, the top 6 chronic diseases in terms of prevalence were hypertension (41.3%), bone and joint disease (12.8%), cerebrovascular disease (12.8%), diabetes (10.1%), ischemic heart disease (7.3%), and gastrointestinal gallbladder disease (7.3%). Among all older adults, 48.6% suffered from only 1 chronic disease, and 22.0% suffered from 2 or more chronic diseases.
Prevalence and Order of Chronic Diseases in Different Age and Gender Groups
The types of high-incidence diseases in all age groups and gender groups were the same, while the prevalence and order of chronic diseases were different. Table 3 shows that with increasing age, the prevalence and order of bone and joint disease, ischemic heart disease, and gastrointestinal gallbladder disease moved higher, whereas those of cerebrovascular disease and diabetes moved lower. In addition, the prevalence of hypertension, bone and joint disease, cerebrovascular disease, and diabetes in females was higher than that in males.
Prevalence and Order of Chronic Diseases in Different Age and Gender Groups.
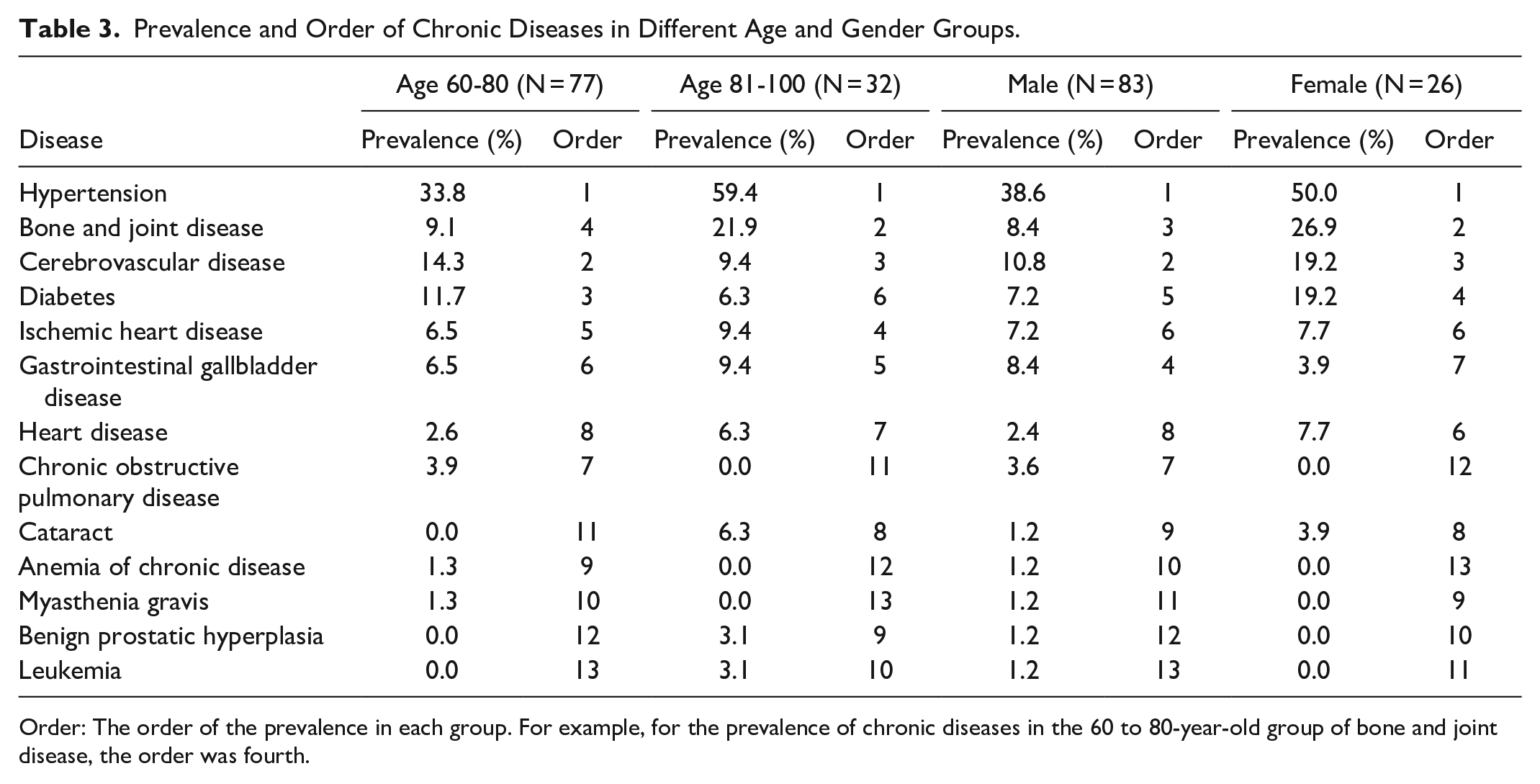
Order: The order of the prevalence in each group. For example, for the prevalence of chronic diseases in the 60 to 80-year-old group of bone and joint disease, the order was fourth.
Comparison of LTCFs With/Without Professional Nursing Staff
The prevalence of chronic diseases in LTCFs with professional nursing staff was 76.5%, versus 65.5% for LTCFs without professional nursing staff. In addition, in the older adults with chronic diseases in both types of LTCFs, most older adults had only one chronic disease (see Table 4).
Prevalence of Chronic Diseases Among Older Adults in LTCFs With/Without Professional Nursing Staff.

Discussion
There were 408 812 residents in Jishou area, of whom 62 187 residents were aged 60 and above. 26 However, there were only 154 older adults living in the LTCFs of Jishou, or 0.3% of all older adults, which was much lower than the 3.0% for all of China. An analysis of the staying rate of older adults found that the staying rate of older adults in urban LTCFs (0.2%) was lower than that in rural LTCFs (0.5%).
The results showed that the prevalence of chronic diseases in LTCF older adult residents in Jishou area was 70.6%, with the prevalence of chronic diseases in descending order being hypertension, bone and joint disease, cerebrovascular disease, diabetes, ischemic heart disease and gastrointestinal gallbladder disease. It is worth noting that the prevalence of chronic diseases in females (80.8%) was much higher than that in males (67.5%), which was consistent with mainland China 12 and other areas.4,5,8 This might be related to the physiological characteristics of females and the fact that they undertake more family affairs. 28 This means that the average life expectancy of females was higher than that of males, although this does not mean that females are healthier. 29 Park 30 divided national patients aged 18 or older in the United States into 4 age groups: early working age, prime working age, mature working age, and elderly age. They found the prevalence and comorbidity of chronic diseases increase with age groups. Our study subdivided the elderly age group into 2 groups 60 to 80 and 81 to 100. According to the results, the conclusion that chronic diseases are more prevalent with age is also true for the older age group. In addition, Shu et al 31 studied found that the medical insurance system was the primary factor affecting the utilization of healthcare services for patients with chronic diseases. In this study, the prevalence of older adults with medical insurance was higher than that of those without medical insurance. This might be related to the higher awareness of medical treatment and the relatively lower burden of disease. At the same time, medical insurance should be fully covered to protect the health rights of older adults. Although Jishou is an area inhabited by multiple ethnic groups, the results show that the difference in the prevalence of chronic diseases among ethnic groups is relatively small. Older adults have varying degrees of sensory impairment, such as impaired balance, sleep disorders, and swallowing disorders,23,32 which leads to an increased prevalence of chronic diseases. Table 3 summarizes and analyses the prevalence and order of chronic diseases based on age and gender. The high-incidence diseases in each group were similar, while the prevalence and order of chronic diseases were different. The order of bone and joint diseases moved higher with age increases, which might be related to the imbalance of bone formation and resorption. 33 In addition, the prevalence of chronic diseases in females suffering from bone and joint diseases was 18.5% higher than that in males, which might be related to menopause or estrogen deficiency. 34
Table 5 presents the composition and prevalence of chronic diseases in some regions of China. Compared with our previous study on older adults in HC in Jishou, Western Hunan, 32 the results showed that the prevalence of chronic diseases in LTCFs older adults was higher than that in HC older adults. Most LTCFs older adults with chronic diseases had only 1 chronic disease (48.6%), whereas most older adults in HC with chronic diseases had 2 or more chronic diseases (44.9%). Moreover, the HC older adults had the same disease composition as LTCFs older adults, while the prevalence and order of chronic diseases were different. Compared with other areas in China, the results showed that the prevalence of chronic diseases in Jishou LTCFs older adults was lower than that in those in mainland China 12 and the economically developed areas of Shanghai, 5 Jiangsu 35 and Changsha, the capital of the same province. 36 However, it was higher than that of the Qiannan ethnic area, which had a similar population structure, region, and economy. 9 The results showed that there were differences in the composition and prevalence of chronic diseases in different regions. It is worth noting that, compared to relatively economically developed areas, bone and joint diseases in the Jishou and Qiannan ethnic areas were the main chronic diseases of older adults, which might be related to the fact that these areas are mountainous with humid and cold climates.
Composition and Prevalence of Chronic Diseases in Older Adults in Some Regions of China.

Due to medical resources being scarce in undeveloped areas. The prevention and treatment of chronic diseases in older adults should not only be based on clinical treatment. It is more important to prevent and control risk factors for chronic diseases. Wang et al 12 surveyed 51 383 older adults in mainland China and found that female, urban, high educational level, and economically developed areas significantly increase the prevalence of chronic diseases (P < .05). Zhang et al 37 reported that the prevalence of the coexistence of chronic disease comorbidities was higher in females (P < .05). In addition, Mwangi et al 38 examined 9 sociodemographic factors, including gender, age, marital status, education, household head, ethnicity, religion, occupation status and economic situation, among 2873 older adults in Vietnam. They found that only females, higher education and advanced age significantly increased the prevalence of chronic diseases (P < .05). In conclusion, there are a number of related factors that can be explored for chronic diseases of older adults, but only a few of them are statistically significant. In our study, 15 factors were used to explore the influencing factors of chronic disease. It was found that only advanced age and impaired balance ability significantly increase the prevalence of chronic diseases (P < .05).
Chronic diseases have become the main cause of premature death in China. The Healthy China 2030 plan proposes that by 2030, the early death rate of major chronic diseases will be reduced by 30% compared with that in 2015. Older adults, as a major group with frequent chronic diseases, can effectively achieve this goal by obtaining an early diagnosis, early treatment and early recovery. “strengthening the health promotion and disease prevention in the older adult” and “promoting the combination of medical care and nursing care” are health support system policies for older adults. Jishou area is a key area supported by the Healthy China 2030 plan, and it is also an area with weak disease surveillance in China. The results of this work can supplement the current status of knowledge on chronic diseases in older adults in similar areas.
Strengths and Limitations of This Study
There are few reports of chronic disease of LTCF residents in the underdeveloped areas of China, this work complements the research in the related areas.
The proportion of chronic diseases in older adults was analyzed according to demographic statistics such as gender, age, living habits and functional disability.
There were 408 812 residents in Jishou, of which 62 187 residents were aged above 60. However, only 154 older adult residents in LTCFs of Jishou, with a ratio is 0.3% of all the older adult residents, results in a small sample size for this work.
It is a cross-sectional study, using the census method, sampling the entire population, without calculating sample size. The cross-sectional study design limited the ability to infer causal relationships from the findings.
Using self-reported questionnaires might have affected participants’ responses and caused their overestimation of their capabilities.
Conclusion
As the aging population expands, the demand for long-term care (LTC) for older adults continues to grow. The LTC model is professional in terms of health care, life assistance, rehabilitation services, etc. However, older adult residents living in LTCFs in Jishou account for 0.3% of all older adult residents, far less than the 3.0% for all of China. LTCFs with professional nursing staff in the Jishou area accounted for only 2/9 of the sample. In addition, the composition of chronic diseases in Jishou area is complex, and testing and screening for regional characteristic diseases such as bone and joint disease should be strengthened to establish a multilevel LTC security system. More importantly, more public health attention and capital investment are needed to increase the proportion of professional nursing staff and specialist doctors in LTCFs and improve the quality of care and medical treatment for older adults. In conclusion, our work comprehensively reports on the status of LTCFs and their elderly chronic diseases in underdeveloped areas of China, providing new insight into elderly chronic diseases.
Supplemental Material
sj-doc-1-inq-10.1177_00469580221128735 – Supplemental material for Long-term Care Facility and its Elderly Chronic Diseases in Jishou: Insights into Underdeveloped Area of China
Supplemental material, sj-doc-1-inq-10.1177_00469580221128735 for Long-term Care Facility and its Elderly Chronic Diseases in Jishou: Insights into Underdeveloped Area of China by Fen Xie, Jinxiu Li, Wenkai Song, Quanlong Liu, Siping Jiang, Zheng-ying Chen and Qingxia Shu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-2-inq-10.1177_00469580221128735 – Supplemental material for Long-term Care Facility and its Elderly Chronic Diseases in Jishou: Insights into Underdeveloped Area of China
Supplemental material, sj-pdf-2-inq-10.1177_00469580221128735 for Long-term Care Facility and its Elderly Chronic Diseases in Jishou: Insights into Underdeveloped Area of China by Fen Xie, Jinxiu Li, Wenkai Song, Quanlong Liu, Siping Jiang, Zheng-ying Chen and Qingxia Shu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
Thanks to the interRAI for their suggestions and help in this research. Thanks for the valuable support and cooperation of the respondents, as well as LTCFs managers and nursing staff.
Authors’ Contributions
FX participated in the design, data analysis and writing—original draft; WKS, QLL, SPJ participated in the data acquisition; QXS, JXL, ZYC participated in the funding acquisition, writing—review and editing. WKS, QLL, SPJ are the third joint works and have equal contributions. The final draft has been read and approved by all authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by The National Social Science Fund of China (21XMZ090) and the Hunan Provincial Innovation Foundation for Postgraduate (CX20211063). The funders had no direct role in the design, data collection, analysis, interpretation or writing of the manuscript.
Ethics Approval and Consent to Participate
The research scheme was reviewed and approved by the Biomedical Ethics Committee of Jishou University (JSDX-2021-0016), and obtained the informed consent of all participants.
Availability of Data and Materials
The datasets used for the current study are available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.