
Abstract
To translate, cross-culturally adapt, and psychometrically evaluate the Older People’s Quality of Life Questionnaire (OPQOL-35) among the Igbo older adult population in Enugu State. The original English OPQOL-35 (E-OPQOL-35) was translated into Igbo language, synthesized, back translated, and subsequently subjected to expert panel review, pre-testing and cognitive debriefing interview. The final Igbo version (I-OPQOL-35) was tested for internal consistency, concurrent, and structural validities in a cross-sectional study of 115 consenting apparently healthy older adults that were conveniently recruited from Enugu State, at 0.05 level of significance. The Spearman correlation coefficients between the participants’ domain and total scores on the I-OPQOL-35 and E-OPQOL-35 (rho = .92-1.00) were excellent. The Mann–Whitney U test revealed no significant difference between corresponding scores in the E-OPQOL-35 and I-OPQOL-35 (P = .65-.94). The internal consistency coefficient of the I-OPQOL-35 was 0.78. The ceiling and floor effects were 0% respectively. The I-OPQOL-35 is therefore a valid and reliable instrument for the assessment of quality of life among Igbo older adults in Nigeria.
The need for availability of culture- and environment- specific tools for assessment of Quality of Life.
Provision of an instrument suitable for use within Igbo population especially for older adults who are non-literate and can neither communicate nor understand English language
Educators and health professionals would need to assess the older adults’ quality of life using the Igbo version of the Older People’s Quality of Life questionnaire that is suitable for them, considering their literacy level.
Introduction
Despite the increase in the proportion of older adults being a victory for humanity, it does not necessarily guarantee living well. 1 Aging is usually accompanied by numerous health challenges including the presence of frailty symptoms, which consequently impacts negatively on quality of life.2-4 Quality of life (QoL) is a subjective, complex concept that depends on the socio-cultural level, ethical and religious values, age group, and personal goals and perceptions of the individual; incorporating several theoretical approaches and assessment methods that needs to be socially relevant.5,6 It can be affected by several factors such as poor physical and mental health status, poverty, retirement, loss of independence, inadequate social interactions, and so on.7,8 With advancing age, maintaining a good QoL at an older age is of increasing relevance and priority globally, requiring valid measurement. 9 As QoL is a largely subjective concept, it is important to reflect lay views in any instrument designed to measure it. 10
Most (if not all) of the QoL scales were originally developed in English (and probably other European languages) that could not be understood by many older adults in low- and middle- income countries (such as Nigeria) who do not receive sufficient formal education. According to National Bureau of Statistics, 11 the English literacy level among older adults in Nigeria is 42.1%. With this literacy level, a good proportion of older adults in Nigeria will not be able to understand nor complete the English version of the OPQOL-35 (E-OPQOL-35). It is therefore imperative to make provision of a validated instrument suitable for use within Igbo population especially for older adults who are non-literate and can neither communicate nor understand English language. Igbo language is one of the 3 major native languages in Nigeria and a minor language in Equatorial Guinea.12,13 Cross-culturally adapting instruments is usually preferred to development of new ones, as the former reduces the costs and the time spent in development and ensures ease of intercultural comparisons.14-16 Beaton et al 14 guideline is the frequently utilized guideline for cross-cultural adaptation. 17 The OPQOL-35 has been translated and validated in other languages: Iranian, 18 Chinese, 19 Czech, 20 Indian, 21 and Australian. 22 However, the OPQOL-35 has not been cross-culturally adapted in Nigerian language and culture. This study was therefore designed to translate, cross-culturally adapt, and psychometrically evaluate the OPQOL-35 among the Igbo older adult population in Enugu State.
Methods
Design
This was a validation study that adopted the protocol for the American Academy of Orthopaedic Surgeons for cross-cultural adaptation developed by Beaton et al. 14 Ethical approval was obtained from the Ethical Review Committee of the University of Nigeria Teaching Hospital, Ituku-Ozalla, Enugu (NHREC/05/01/2008B-FWA00002458-1RB00002323). The OPQOL-35 was not under license, and permission was obtained from the developers to translate and validate the E-OPQOL-35. Older adults who met the inclusion criteria were consecutively recruited from communities of conveniently selected local government areas in Enugu State (Enugu South, Enugu East, Igbo-etiti, Nsukka). All participants were informed about the purpose and procedures of the study, and assured confidentiality; and gave informed consent. The eligibility criteria were inclusion of older adults (≥65 years) who could understand both English and Igbo languages, and were well-oriented in time, place and person; while excluding older adults with communication impairment and any life-threatening condition that could affect result outcomes.
Instruments for Data Collection
Older People’s Quality of Life Questionnaire (OPQOL-35)
This is a 35-item questionnaire developed for assessing QoL among older adults. The 35 statements of the questionnaire consider the following 8 domains of QoL: life overall, health, social relationships and participation, independence, control over life and freedom, home and neighborhood, psychological and emotional well-being, financial circumstances, and religion and culture. Items are scored (with reverse coding of positive responses) so that higher scores indicate a better QoL. Thus the total score ranges from 35 to 175. The OPQOL-35 is a validated instrument and has been shown to have acceptable psychometric properties.23,24
Translation, Cross-Cultural Adaptation, and Validation of the OPQOL-35
Translation stage
This stage involves forward translation of the items and response choices of the E-OPQOL-35 into Igbo language by 2 independent bilingual translators, a linguist and a physiotherapist, whose native language is Igbo, with fluency in English to produce 2 Igbo translated versions (FT1and FT2). The translators were instructed to aim for conceptual instead of literal translation; to provide a language translation as used by the population, thus providing a more reliable equivalence from a measurement and clinical perspective. The 2 translators reconciled and synthesized the 2 translations to produce a single common version (ST-12). For items and responses that were linguistically or culturally ambiguous, the translators chose more preferred options after exhausting all available choices. The ST-12 was translated back to English language by 2 different bilingual translators for conceptual equivalence with the original English version, producing 2 back-translated English versions (BT1 and BT2). The 2 back-translated English versions were compared with the original English version, to check for mistakes and misinterpretations, in order to ensure the reproducibility of the same item content as the original version. Both translators were physiotherapy lecturers who were fluent in both English and Igbo languages, and also knowledgeable in cross-cultural adaptation procedure.
Adaptation Stage
All the translations including the E-OPQOL-35 were examined by an expert committee review while ensuring operational, experiential, conceptual, measurement, idiomatic, and semantic equivalences. The expert panel comprised the 4 translators, 4 physiotherapy researchers, and a lay person. The expert committee were very familiar with the Igbo culture and environment, and identified the comprehensiveness, relevance and comprehensibility of the instructions, items and response options. Some modifications were made to some words and phrases. Differences in the translations were unanimously resolved, thus producing a pre-final Igbo version of the questionnaire.
This pre-final version was pretested on 30 consenting eligible older adults. These participants were taken through the process of cognitive debriefing interview in order to determine the clarity, perception, applicability, and understanding of various terminologies used on each item on the questionnaire and the responses. Each participant was expected to answer “YES” or “NO” for each item and response options. Items or response option with less than 80% positive answers were supposed to be amended. However, all the items had at least 95% positive answers. Hence, the final Igbo version of the OPQOL-35 (I-OPQOL) was accordingly developed.
Validation Stage
The E-OPQOL and the I-OPQOL were either interviewer-administered or self-administered. A sample size of 112 had an 88% power to detect a moderate change of 0.3 at 0.05 level of significance. Sample size was calculated using G* Power 3.0.10. 25 The purpose of administering the E-OPQOL was to ascertain the concurrent validity of the I-OPQOL. Simple randomization method was used to administer the questionnaires. Participants that picked “I” responded to the I-OPQOL first while those that picked “E” responded to the E-OPQOL first.
Data Analysis
Data was analyzed using the Statistical Package for Social Sciences version 21. The demographic information and the scores from the I-OPQOL and the E-OPQOL were summarized using frequency counts, percentages, mean and standard deviation. The Spearman rank order correlation was used to determine the concurrent validity of the I-OPQOL. The questionnaire was tested for ceiling and floor effects. The instrument would be regarded as having floor or ceiling effect if more than 15% of the participants achieved minimum or maximum possible scores respectively. 26 The Cronbach’s correlation coefficient was used to determine the internal consistency of the I-OPQOL. The standard error of mean (SEM) and the minimal detectable difference (MDD) of the total and domain scores on the I-OPQOL were calculated using: MDD = 1.96 × SEM × √2. 27 Principal component analysis (PCA) was used to estimate the structural validity of the I-OPQOL.
In order to check the suitability of data for factorial analysis before performing the PCA, the Kaiser-Meyer-Olkin (KMO) 28 value must exceed the recommended value of 0.6 and Barlett’s test of sphericity 29 value must be significant. When all the correlation matrix coefficients between each item pair on the I-OPQOL exceeded the recommended value of 0.3, it would reveal that all the items measured the same construct. Communality values that are less than 0.3 may indicate that the item did not fit well with the other items loading on the same component. Throughout the PCA, only factors with its eigen values exceeding one are normally retained. The retained factors were further illustrated using the scree plot. 30 Any component with initial eigen value lower than the random eigenvalue are often rejected. The number of components to retain was decided by the Monte-Carlo parallel analysis. Level of significance was set at P < .05.
Results
Pilot Testing of the Pre Final Version of the I-OPQOL-35
The pre-final version of the I-OPQOL-35 was pretested on 30 older adults who were taken through cognitive debriefing interview. These participants had at least 95% of clarity and ease of understanding of most of the items except for 3 items (2, 4, & 24). These items were considered and modified at the second panel meeting based on the more suitable option for it. The second item (I am happy much of the time) was modified from “A na m enwekarị obi an˙ụrị” to “A na m enwe obi an˙ụri ọtụtụ oge. The fourth item (Life gets me down) was modified from “Ndụ na-akụtu mmụọ m” to “ndụ kụturu m ala,” and finally the 24th item (I tend to look on the bright side), from “A na m enwe an˙ụrị na nchekwube na agbanyeghị ịhe ọ bụla” to “A na m elegara anya na ihe ọma dị n’ọnọdụ niile.” No further modifications were made on the questionnaire, and hence, the final Igbo version of the OPQOL-35 was produced.
Validation of the I-OPQOL-35
Socio demographic profile of the participants
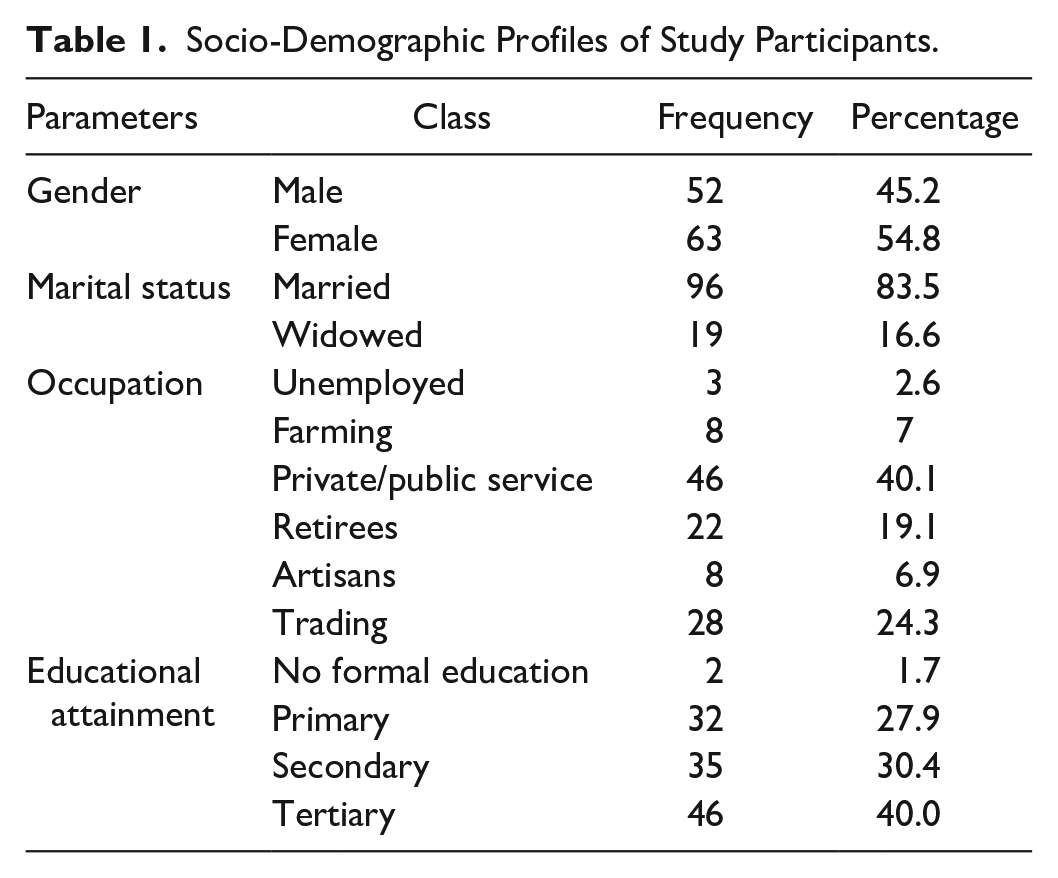
A total of 115 (male 45.2%, female 54.8%) older adult respondents participated in the psychometric testing. Majority of the participants (83.5%) were still married; 70.4% had at least a secondary education; 19.1% were retirees; while 40.1% were civil/public servants (Table 1).
Socio-Demographic Profiles of Study Participants.
Validity and Reliability Analysis of the I-OPQOL-35
Concurrent validity
The coefficients of correlations between corresponding domain and total scores on the E-OPQOL-35 and the I-OPQOL-35 were all excellent and significant (rho = 0.92-1.00; P < .001), with the “religion and culture domain” and “total” scores having the least and highest correlation coefficients respectively. This indicates excellent concurrent validity in all the total and domain scores on the I-OPQOL-35 (Table 2), thus suggesting that the E-OPQOL-35 and the I-OPQOL-35 can produce equivalent scores when administered to the same individuals. The scatter plots of the correlation between the total scores on the I-OPQOL-35 and the E-OPQOL-35 is shown in Figure 1. The Bland-Altman plot pictorially illustrates the total scores on the I-OPQOL-35 and the E-OPQOL-35, revealing homoscedasticity of both results (Figure 2). A comparison between the domain scores on the E-OPQOL-35 and the I-OPQOL-35 using the Mann-Whitney U test showed no significant difference (P > .05) in any of the domains, thus indicating the linguistic and conceptual equivalence of the 2 versions (Table 3). The ceiling and floor effects are 0% respectively as no participant scored the lowest or the highest score.
Spearman Rank Order Correlation Between the Domains in the English and Igbo Versions of the Older People’s Quality of Life Questionnaire.

Mann–Whitney U test Comparing Scores on Both the English and Igbo Versions of the Older People’s Quality of Life Questionnaire Domain.
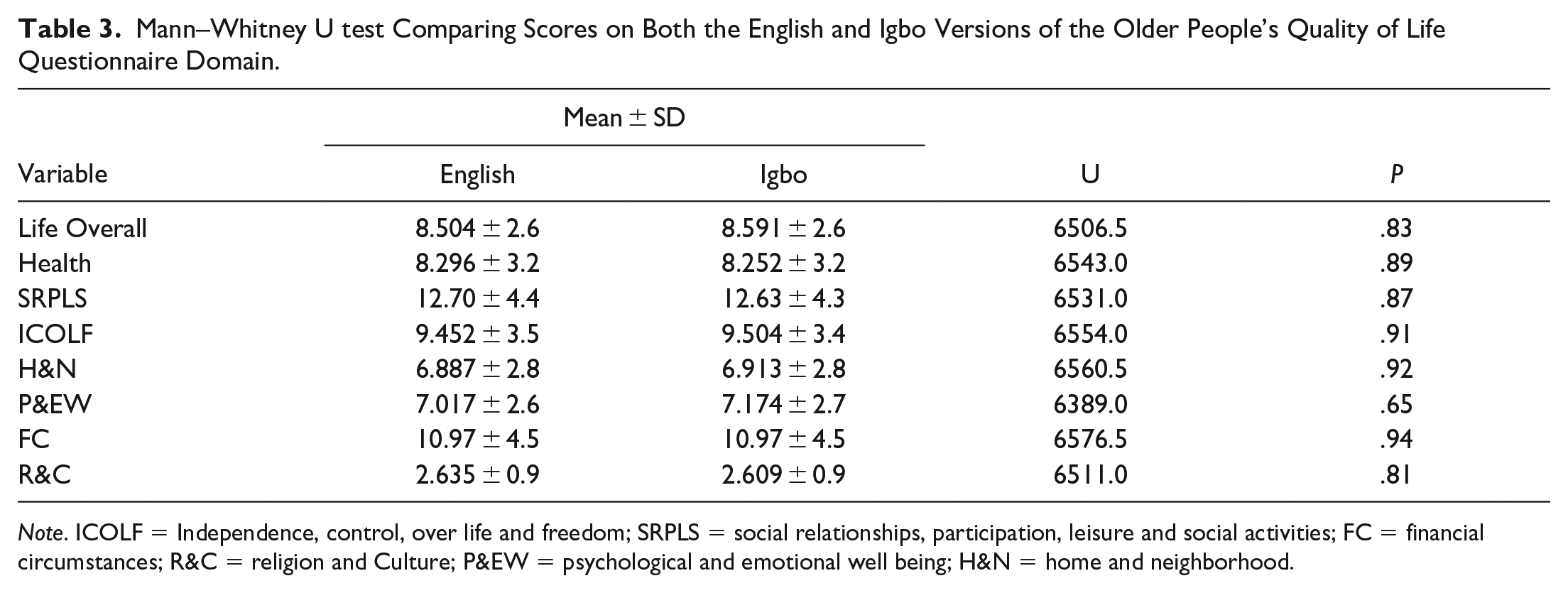
Note. ICOLF = Independence, control, over life and freedom; SRPLS = social relationships, participation, leisure and social activities; FC = financial circumstances; R&C = religion and Culture; P&EW = psychological and emotional well being; H&N = home and neighborhood.

Scatter diagram for total scores on the I-OPQOL-35 and the E-OPQOL-35.

Bland-Altman plot of the total scores on the I-OPQOL-35 and the E-OPQOL-35.
Structural Validity of the I-OPQOL-35
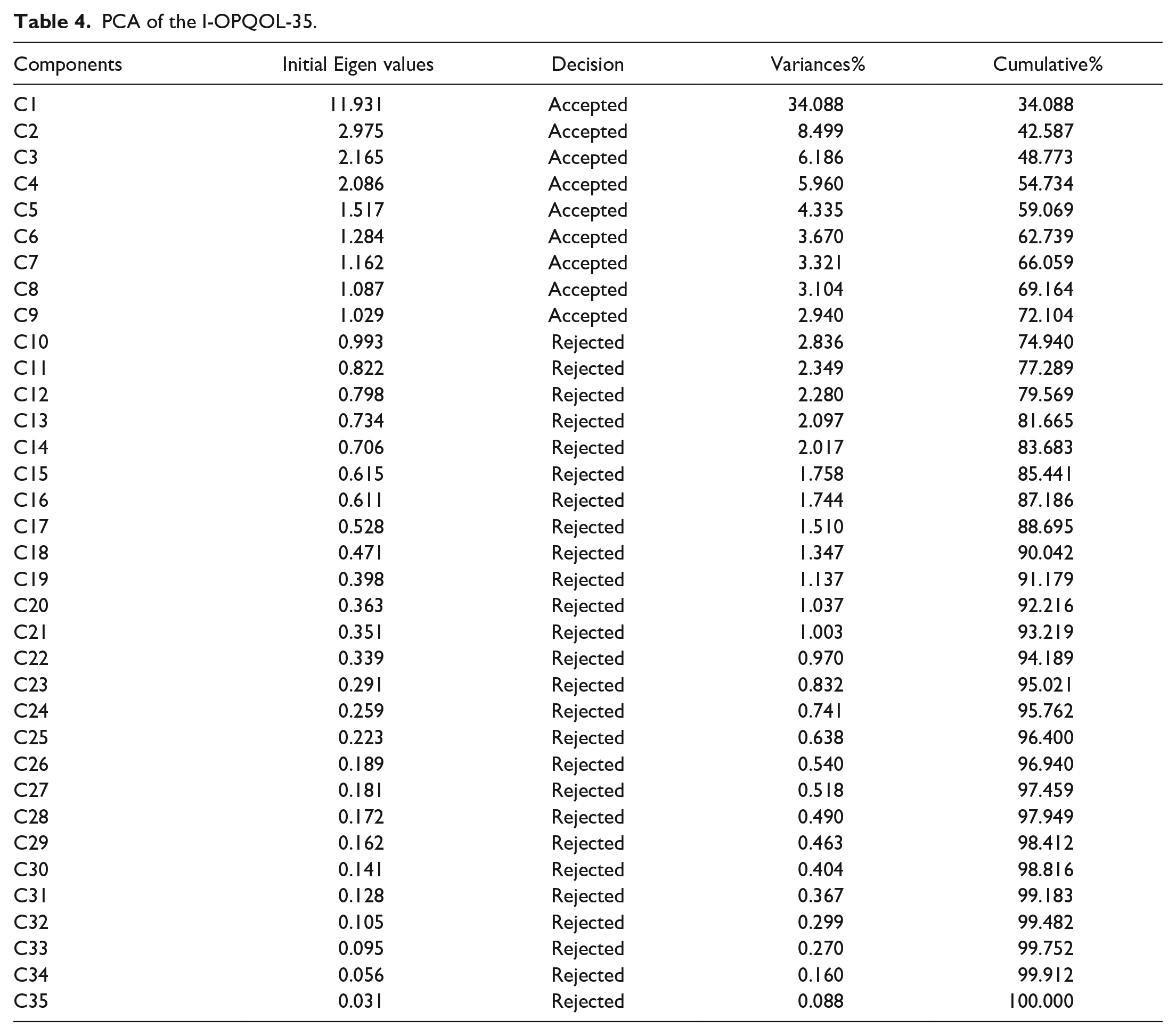
Prior to performing PCA, the suitability of the data for factor analysis was assessed. The KMO value of 0.833 exceeded 0.6, which is the recommended value, while the Barlett’s test of sphericity reached statistical significance (X2 = 2794.665; P < .001), thus supporting reasonable factorability of the data. The PCA revealed the presence of 9 factors with eigenvalues exceeding 1, describing 34.088, 8.499, 6.186, 5.960, 4.335, 3.670, 3.321, 3.104, and 2.940 of the variances respectively. The 9 component solution thus explained a total of 72.103% of the variances. Other factors had eigen values less than 1 (Table 4). Scree plot also illustrated the presence of these 9 factors (Figure 3). All the 35 scale items had communality values that were >0.3 which indicated that all the items fit well with one another, and are to be retained for use on the scale (Table 5).
PCA of the I-OPQOL-35.
Communalities of the Items on the I-OPQOL-35.

Note. Extraction Method Principal Component Analysis; I-OPQOL-35: Igbo version of the Older People’s Quality of Life questionnaire.

Scree plot of the components on the I-OPQOL-35.
Internal Consistency
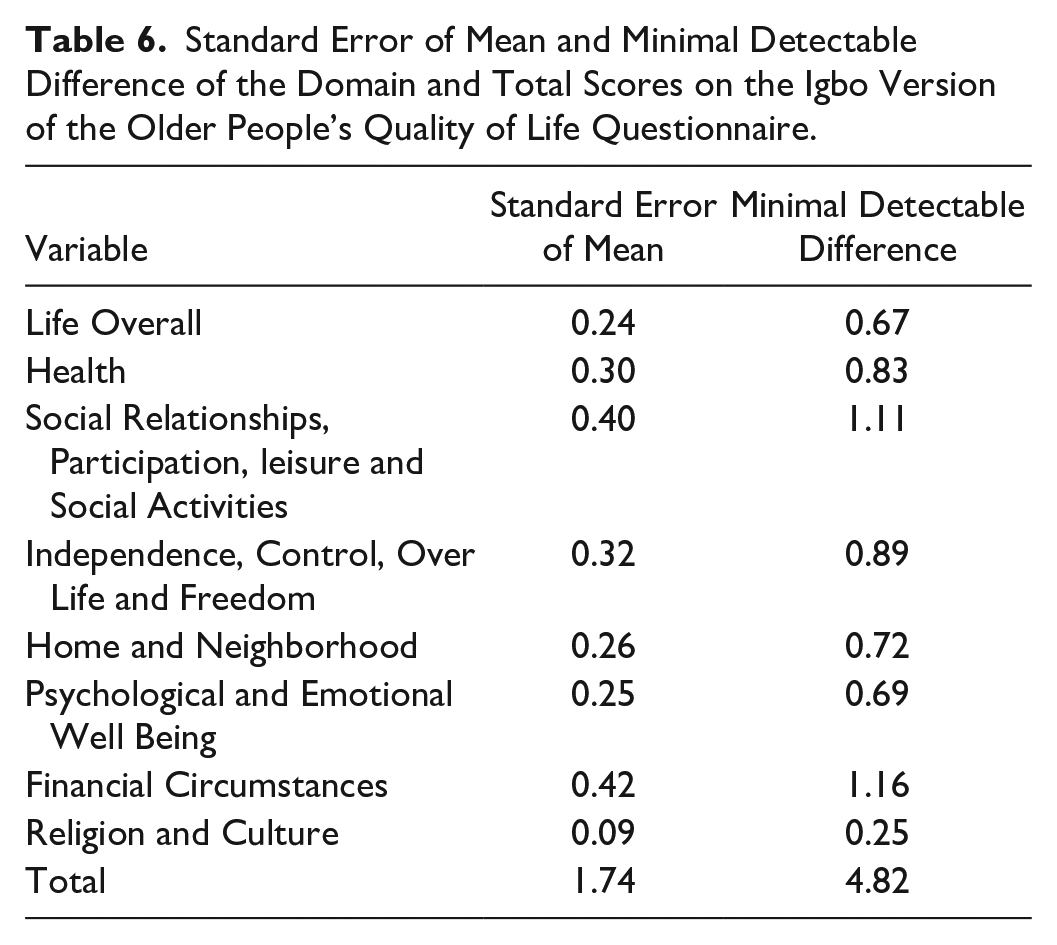
The internal consistency of the I-OPQOL was tested using the Cronbach’s correlation coefficient. The Cronbach’s alpha for the domain-to-total correlation on the I-OPQOL-35 was 0.78. This value shows that the internal consistency was good, thus indicating that the items on the I-OPQOL-35 measure different aspects of the same construct. The standard error of mean and minimum detectable difference values for the domain and total scores on the I-OPQOL-35 are shown on Table 6. The MDD values ranged from 0.25 (Religion and Culture domain) to 4.82 (total score).
Standard Error of Mean and Minimal Detectable Difference of the Domain and Total Scores on the Igbo Version of the Older People’s Quality of Life Questionnaire.
Discussion
This study was devised to cross-culturally adapt and validate the Igbo version of the OPQOL among Igbo older adults in Enugu following a widely accepted and standardized guideline. 14 The study findings revealed that the OPQOL-35 is a multidimensional scale and has acceptable psychometric properties.
During the translation process, 2 different translators at each of the forward and backward translations were involved. This procedure was also followed in other studies.31,32 It was also ensured that one of the forward translators had no medical background and that 3 of the translators were blinded about the concept of the instrument. This was to reduce the possibility of bias in the translation. All the items on the original version of the OPQOL-35 were considered by the expert panel to be of relevance for the measurement of QoL among Igbo-speaking older adults and environment. However, little modifications were made in order to ensure semantic, experiential and conceptual equivalence of the terms in Igbo Language and culture; in agreement with the recommendations by Beaton et al 14 that a newly adapted scale should comprise terms that are experientially equivalent in the new culture for which it was developed.
The OPQOL-35 has been translated into various languages and used in numerous countries (eg, Iran, 18 China, 19 Czech, 20 India, 21 and Australia. 22 These translations are used in place of the original English version in these places and anywhere the speakers of these languages are found. Consequently, this could be obtainable with the I-OPQOL-35 and may be applicable to persons who speak the Igbo Language irrespective of where they find themselves. The Igbo language maintains a central cultural and linguistic pattern which is well understood across all Igbo-speaking regions and by all Igbo-speaking persons, despite its varying dialects. The translation into Igbo language which is one of the major native Nigerian Languages will aid the effectiveness of its use among speakers of Igbo language.
There was no significant difference in the total and domain scores of both the I-OPQOL-35 and E-OPQOL-35. Furthermore, there were significant correlations between the participants’ total and domain scores on the Igbo and the English versions of the OPQOL-35, suggesting an excellent concurrent validity of the I-OPQOL-35, which suggests the equivalence of the I-OPQOL-35 and E-OPQOL-35 in concept, semantic and context. The original English or Igbo version of the OPQOL-35 can therefore be administered on an Igbo-speaking individual with the likelihood of obtaining the same result.
No participant had either the highest or the lowest total scores on the I-OPQOL-35 indicating that the scale had no ceiling or floor effects. The I-OPQOL-35 showed good internal consistency demonstrated by a Cronbach’s alpha value of 0.78 which falls within the acceptable range. This suggests that the items on the I-OPQOL-35 are homogenous and are all measuring various aspects of the same variable. Similarly, studies also reported good internal consistency for the OPQOL in different settings. This is consistent with previous reported values in the Czech (0.73-0.91) and Italian (0.78) versions.20,23 A 0.86 Cronbach’s alpha value was also reported in Sri Lanka. 6 Soleimani et al 33 had opined that though the Cronbach’s alpha coefficient is improved by a large number of items, the high Cronbach’s alpha value observed for the entire measure however may not suggest a unidimensional measure. The SEM and MDD values of the I-OPQOL-35 reported in this study will be helpful in the future in knowing when a significant change is produced.
Findings from the principal component analysis demonstrated that 9 factors had eigen values exceeding 1. This shows that the I-OPQOL-35 has nine domain scores which could be named as follows: 1 independence, control over life and freedom; 2 financial circumstances; 3 belief, home and neighborhood; 4 loneliness; 5 leisure and activities; 6 health; 7 psychological and emotional wellbeing; 8 family, social relationships and participation; 9 Satisfaction with life. The 9 components explained a total of 72.10% of the variance, with factor 1 (34.09) contributing the most to the variance. This finding of factor 1 contributing the most to the total variance observed, is in consonant with previous studies.18,34 This suggests that the prevalent nature of older adults’ perception of their life overall contribute the most to the assessment of QoL globally. Though the original version of the OPQOL contained 8 factor structures which was based on open survey, its PCA revealed 9 components whose eigenvalues were greater than 1, accounting for 60.583% of the total variance.10,34 In Iran and China, eight factors with eigenvalues greater than one, accounting for 67.4% and 63.7%of the variance respectively were reported 18,19; in Czech, 7 factors explained 62.3% of the total variance. 20 This could suggest the ambiguity and multidimensionality of the factor structure of OPQOL. Furthermore, factor 9 had only 2 items with highest loadings, and so, could be merged with others to ensure a more stable factor structure.
Factor analysis usually answers the question of validity and provides a diagnostic tool to evaluate the suitability of the data in terms of pattern and structure, thereby determining the accuracy of the said tool in measuring what it is designed to measure.35,36 Kaiser recommends that only KMO value greater than 0.6 is acceptable. 28 KMO values that are less than this usually lead to either collection of more data or an evaluation of the items to be incorporated. The present study has a KMO value of 0.83 which is highly acceptable. The Bartlett’s test of sphericity also revealed that P < .001 which is highly significant, thus suggesting that factor analysis was appropriate.
Limitations
The first limitation is the small sample size. As a rule of thumb, validation of the instrument required at least 10 participants per item. The inclusion criteria of being fluent in both English and Igbo languages greatly reduced the number of potential participants. Individuals who were unable to understand English Language were excluded from the study, which might have introduced some degrees of bias. This was a fundamental requirement of the adopted protocol, and hence the investigators had no control over this eligibility criterion.
Conclusions
The OPQOL-35 was successfully translated, adapted and validated into Igbo language. The I-OPQOL-35 is a valid and reliable instrument. It is recommended that the I-OPQOL be translated and validated into other major languages in Nigerian and international languages. The availability of this tool in numerous languages would enhance its applicability across various cultures. Further researches should be performed to explore the responsiveness and predictive validities, test-retest reliability, inter-rater, and intra-rater reliabilities of the I-OPQOL; and also more robust statistical analysis should be performed.
Supplemental Material
sj-docx-1-inq-10.1177_00469580221126290 – Supplemental material for IGBO Version of the Older People’s Quality Of Life Questionnaire (OPQOL-35) Is Valid and Reliable: Cross-Cultural Adaptation and Validation
Supplemental material, sj-docx-1-inq-10.1177_00469580221126290 for IGBO Version of the Older People’s Quality Of Life Questionnaire (OPQOL-35) Is Valid and Reliable: Cross-Cultural Adaptation and Validation by Ukamaka Gloria Mgbeojedo, Chisom Cassandra Ekigbo, Emmanuel Chiebuka Okoye, Echezona Nelson Ekechukwu, Adaora Justina Okemuo, Chioma Nneka Ikele and Christopher Olusanjo Akosile in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
The authors acknowledge the Emerging Research and Professionals in Ageing-African Network.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the Ethical Review Committee of the University of Nigeria Teaching Hospital, Ituku-Ozalla, Enugu (NHREC/05/01/2008B-FWA00002458-1RB00002323).
Informed Consent
Informed consent (written or verbal, as applicable depending on the level of literacy) was also obtained from the participants after the study procedures had been thoroughly explained to them.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.