
Abstract
Purpose
This study examines how the coronavirus disease 2019 (COVID-19) is affecting utilization of medical and behavioral health services through school based health centers (SBHC s).
Methods
We leveraged the electronic health records from one of the largest sponsors of SBHCs in the country, and tested differences in SBHC utilization with chi-square tests one year prior to the pandemic (pre-pandemic: March 2019-February 2020) compared to one year into the pandemic period (March 2020-February 2021).
Results
A significant difference in SBHC utilization was found between pre-pandemic and pandemic periods (P <.001). 63.5% of SBHC patients accessed medical services pre-pandemic compared to 51.2% during the pandemic. In contrast, 36.5% of SBHC patients accessed behavioral services pre-pandemic compared to 48.8% during the pandemic, representing a 12.3% increase in SBHC behavioral service utilization since the pandemic.
Conclusions
SBHCs may serve as an invaluable means of ensuring youth, particularly those from disadvantaged communities, have access to needed behavioral health services during the current public health crisis.
Keywords
School based health centers serve as the primary, and often, sole source of healthcare for youth from underserved communities. Understand how school based health center utilization, inclusive of medical and behavioral health services, by disadvantaged youth has changed during the pandemic. Underscores importance of school based health centers in providing behavioral health services to underserved youth, particularly during the pandemic and co-occurring mental health crisis.What Do We Already Know About This Topic?
How Does Your Research Contribute to the Field?
What Are Your Research’s Implications Towards Theory, Practice, or Policy?
Introduction
Youth in the U.S. experience many disparities in healthcare access and outcomes.1-4 Black, Indigenous, and People of Color (BIPOC) youth and youth from disadvantaged communities in particular, continue to experience longstanding challenges to accessing routine and preventive services.5,6 In addition, most recent national surveillance data found an increasing percentage of youth feeling sad or hopeless for at least two weeks that impaired their ability to engage in usual activities. 7 More specifically, the percentage of youth who seriously considered suicide or made a suicide plan increased significantly among disadvantaged and underserved communities in the last decade. 8 The pervasiveness of adverse childhood experiences (ACEs, eg, physical, emotional, or sexual abuse; poverty; parental absence, incarceration, or addiction), along with increased incidents of community trauma (eg, mass shootings, natural/manmade disasters) are also taking a toll on youth across the U.S. 9
Additionally, it is important to highlight the significant disparities in youth mental health outcomes. For example, 1 in 6 youth in the U.S. have diagnosed with mental health disorders. The rates are even higher for low-income youth and youth of color (17.8% to 34.4%). 10 Similarly, approximately one quarter of youth in the U.S. have experienced two or more ACEs, with a higher rate for low-income youth and youth of color (30.7%). 11 There is strong evidence suggesting that low-income youth of color have the highest rates of unmet need for mental health services.7,12 The social and economic repercussions of the current COVID-19 pandemic, including major academic disruptions, heightened food insecurity, and household income loss and stress, have both shed light on and exacerbated existing health disparities among youth of color and their families who have been hardest hit by the pandemic. 13 In addition, strategies to slow the spread of COVID-19 will compound longstanding underlying health and racial disparities. 14
There is a growing body of research supporting the role of school based health centers (SBHCs) in promoting health care access and improving health outcomes among underserved youth. SBHCs have been associated with increased primary care services, increased mental health-seeking behavior, decreased alcohol and substance use, as well as reduced school suspensions and increased graduation rates.15-20 Moreover, SBHCs have been maintained their service delivery amid COVID-19 pandemic challenges.21,22
According to the School-Based Health Alliance’s most recent census, more than 2500 SBHCs provide health care services access to over six million youth across the U.S., and are more likely to be located in communities with higher percentages of youth of color, and low socioeconomic status. 23 SBHCs are organized through school, community, and health provider relationships, and provide services in accordance with state and local laws. 24 SBHCs are increasingly sponsored and operated by Federally Qualified Health Centers (FQHCs). 23 FQHCs are able to provide financial sustainability for SBHCs by having Federal funding from the Health Resources and Services Administration (HRSA), 25 as well as reimbursement incentives by serving patient populations who are eligible for Medicaid or Child Health Insurance Program (CHIP). 26 Moreover, FQHC sponsorship of SBHCs has been shown to be a viable means of expanding access in schools with predominantly low-income, BIPOC student populations. 27
Nonetheless, with policies affecting school closures and the pivot to remote learning and telehealth, less is known about health care access and utilization through SBHCs during the pandemic. To our knowledge, this is the first study to examine changes in SBHC access and utilization among underserved youth during COVID.
Methods
Data
Data was extracted from all electronic health records at SBHCs sponsored by Community Health Center, Inc (CHC), a large FQHC in Connecticut and one of the largest sponsors of SBHCs in the U.S. CHC sponsors over 180 SBHCs across the state, serving the healthcare needs of over 17 000 students annually. 28 The demographics of the sample population managed through CHC-sponsored SBHCs is generally representative of those seen at SBHCs across the country given the focus on schools with a significant percentage of students with low SES. For the purposes of this study, we classified data one year prior to COVID (March 2019-February 2020) as pre-pandemic, and one year since the inception of COVID (March 2020 –February 2021) as pandemic. This study has been reviewed and deemed exempt by the Community Health Center, Inc Institutional Review Board.
Measures
Sample characteristics and outcome measures.
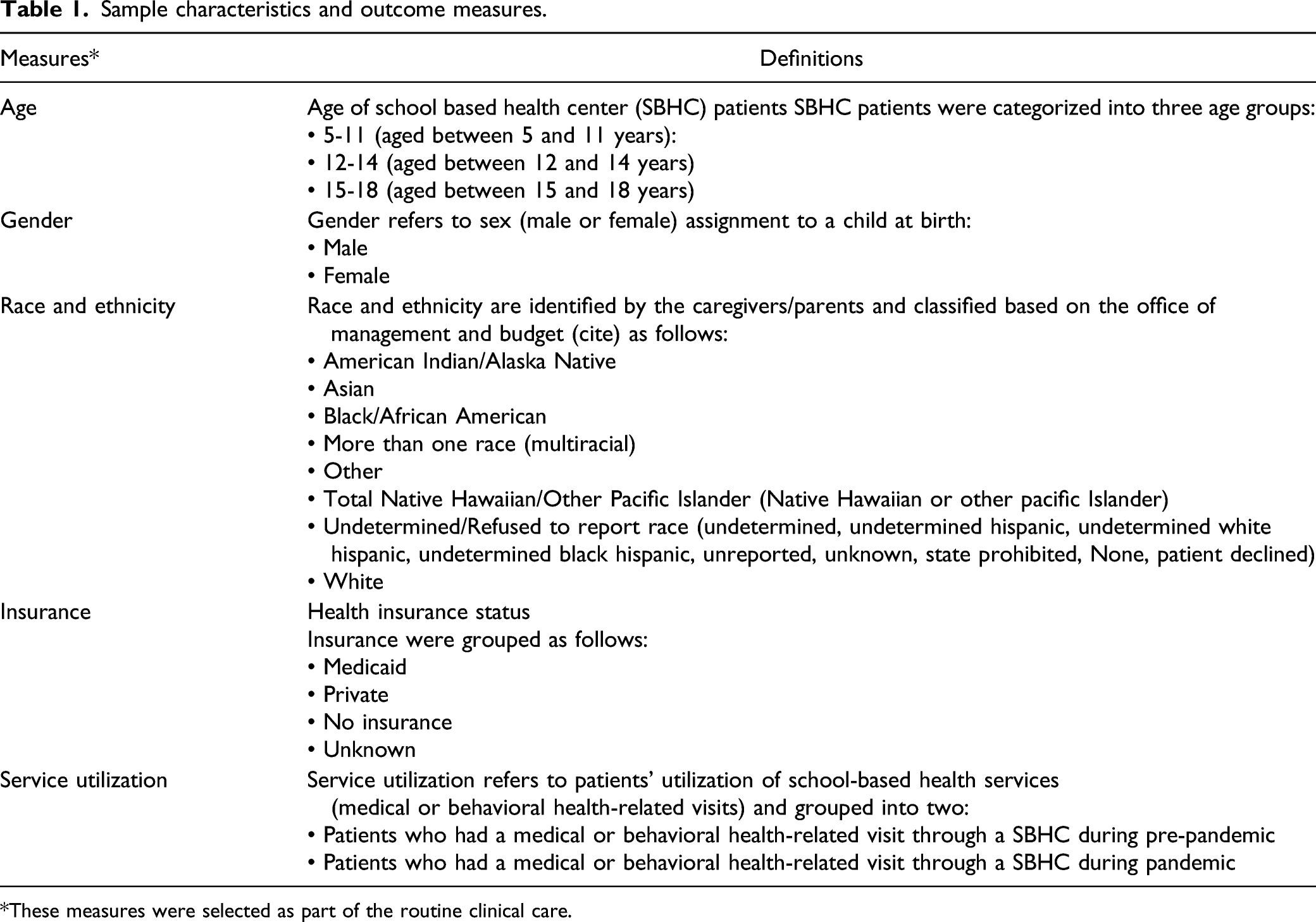
*These measures were selected as part of the routine clinical care.
Analysis
We tested differences in SBHC utilization during pre-pandemic and pandemic periods with chi-square tests. Descriptive data were also compared in the analyses. An alpha value of P less than .05 was used to consider the statistical significance. All data were analyzed using SPSS (version 27).
Results
Sample characteristics during pre-pandemic (March 2019-February 2020) and pandemic (March 2020-February 2021) periods.

A significant difference in SBHC service utilization was found between pre-pandemic and pandemic periods (P <.001). 63.5% of SBHC patients accessed medical services pre-pandemic compared to 51.2% during the pandemic, a 12.3% decrease in SBHC use for medical purposes. In contrast, 36.5% of SBHC patients accessed behavioral services pre-pandemic compared to 48.8% during the pandemic, representing a 12.3% increase in SBHC behavioral service utilization since the pandemic (Figure 1). School based health utilization of medical and behavioral services in pre-pandemic (March 2019-February 2020) and pandemic (March 2020-February 2021) periods.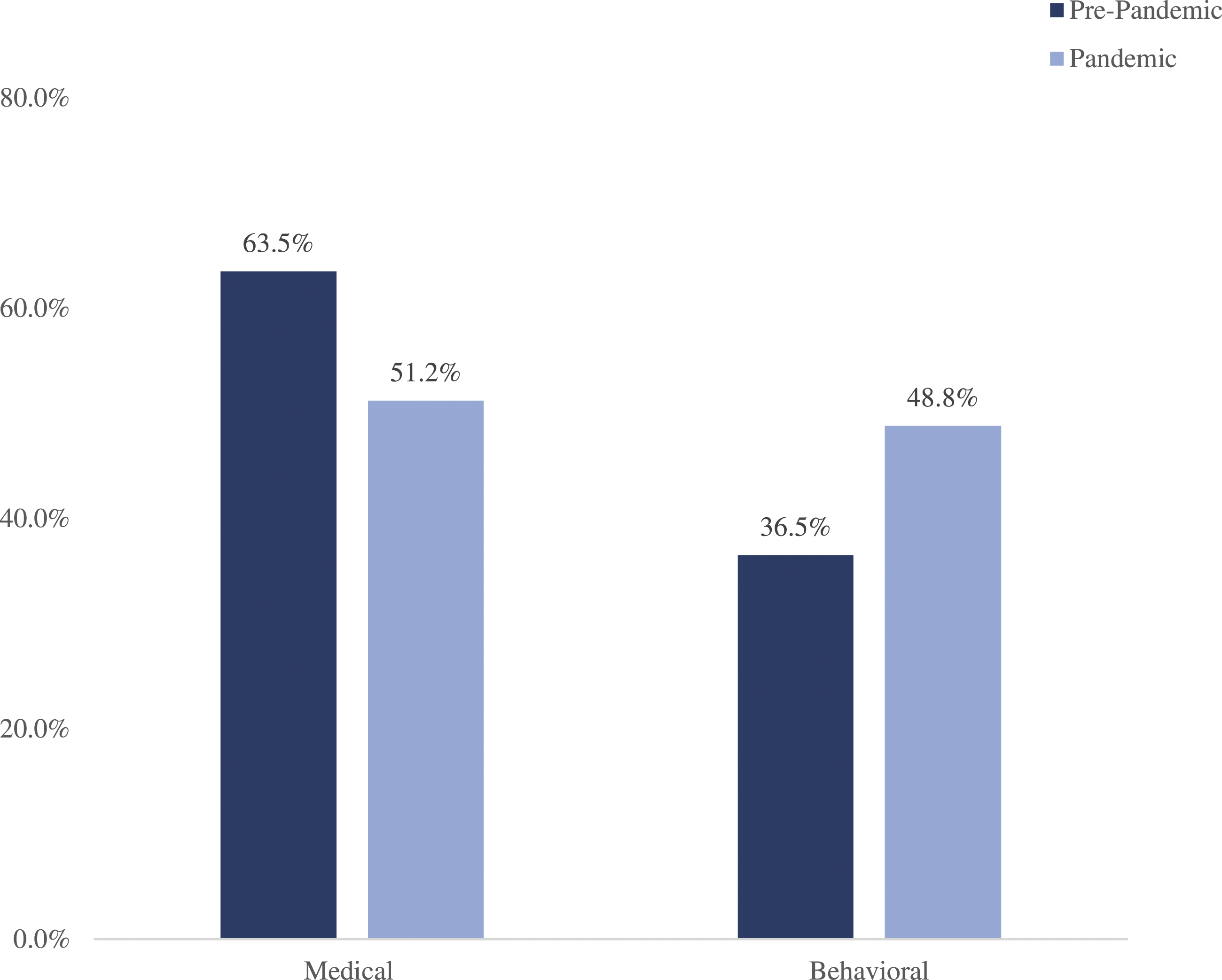
Discussion
Our study is the first to examine changes in SBHC utilization during COVID. Moreover, our study contributes to the existing literature supporting the unique role of FQHCs in expanding SBHCs and subsequently, promoting access in underserved communities. 23 Data suggest that utilization of behavioral health services through SBHCs has increased during the pandemic, which is consistent with the growing body of literature regarding the mental health crisis that the pediatric population is experiencing related to the pandemic.13,29,30
There are several limitations worth noting. Our sample of SBHCs are sponsored by a relatively large FQHC in Connecticut that has been sponsoring SBHCs for over two decades, and had the reimbursement incentives, infrastructure, and capabilities to transition to telehealth early in the pandemic; thus, findings from this study may not necessarily be reflective of other SBHCs that lacked the resources to continue to provide health care services during the pandemic, or are in the early stages of implementation. Also, we lacked race/ethnicity data for a third of our sample, which makes it challenging to draw any conclusions regarding changes in health care utilization by race/ethnicity since the pandemic. Lastly, while the current study incorporate SBHC-level and patient-level data, additional familial- and communal-level factors may influence SBHC utilization, which were not accounted for here.
Despite these limitations, our study highlights the potential for SBHCs to promote health service access and utilization among underserved youth, including during public health emergencies. Future research should continue to explore the role of SBHCs in addressing unmet needs among underserved youth, including youth not explicitly examined in this study (eg, sexual minority, undocumented youth).
Implications for Practice And/Or Policy
The social and economic repercussions of COVID-19, alongside political and racial strife, have exacerbated the existing mental health challenges that youth have been facing prior to the pandemic. SBHCs appear to be effective service delivery system in preventing mental health problems, especially for youth of color and their families with barriers to health care access. 30 For that reason, SBHCs can serve as a viable means of ensuring youth, particularly those from underserved communities, have access to needed mental health services, thereby mitigating future strain on the health care system.
Footnotes
Acknowledgments
We would like to acknowledge Community Health Center, Inc. For allowing us to use school based health service utilization data for research purposes.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.