
Abstract
The aim of the current study was to examine the mental well-being of healthcare personnel (HCP) working in COVID-19 units in Greece and to calculate the prevalence of burnout (BO) amongst them. A questionnaire based on the Maslach Burnout Inventory for Medical Personnel was utilized between February 21st, 2021 and March 5th, 2021. A total of 190 HCP responded to the questionnaire, of which 73.7% were nurses and midwives. The mean age of the participants was 38.3 (8.4) years. Overall, 71.6% of the participants had a high BO score, while 20.5% had a moderate and 7.9% had a low BO score. Night shifts in COVID-19 wards and job dissatisfaction were significantly associated with a high BO score (P = .03 and P < .0001, respectively). The majority of HCP working in COVID-19 wards in Greece is experiencing high levels of overall BO and emotional exhaustion.
Multiple studies have already demonstrated the devastating psychological implications of COVID-19 pandemic in HCP, including the increased risk of burnout syndrome. Our study examines how the ongoing pandemic is affecting the mental well-being of HCP working in COVID-19 units specifically in Greece and calculates the prevalence of BO amongst them, in the course of the third wave of the pandemic. The results of the study clearly indicate the need to establish policies preventing and managing the burnout symptoms in HCP.What Do We Already Know About This Topic?
How Does Your Research Contribute to the Field?
What Are Your Research’s Implications Towards Theory, Practice, or Policy?
Introduction
The novel coronavirus that was registered as Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), the cause of coronavirus disease 2019 (COVID-19) 1 spread worldwide, causing World Health Organization (WHO) to declare a pandemic in March 2020. Since then, over 480 millions of confirmed cases of COVID-19 and over 6 million deaths in over 220 countries have been reported. 2 In the course of this crisis, healthcare personnel (HCP) have endured severe physical and psychological distress. Reports published since the dawn of the pandemic clearly demonstrate the magnitude of mental trauma experienced these past years by HCP,3,4 especially by those working in the frontlines. 5 On top of the burden of social distancing and the government-enforced quarantine that every member of the society is facing, frontline medical workers have to also handle the constant threat of exposure to the virus, risking not only their health but also the wellbeing of their families. Adding to the fear of the actual disease, current research also suggests long term effects of the infection with the emergence of the “post COVID-19 syndrome”.6,7 All the aforementioned factors, alongside the limited resources of the hospitals, the longer working hours and the need for more night shifts, are putting “frontliners” at great risk of psychological trauma and burnout (BO). 8
Burnout Syndrome in COVID-19 Healthcare Professionals
BO is a remarkable psychosocial problem that has been increasingly recognized in demanding professions and is caused by the unsuccessful management of chronic stress in the workplace. It is a psychological syndrome marked by energy depletion, increased mental distance from one’s work (i.e., cynicism or negativism), and reduced professional efficacy. 9 Considering the nature of the healthcare-related professions, healthcare workers were found to be susceptible to depressive symptoms, anxiety and BO even prior to the COVID-19 crisis. 10 Both individual and work-related factors contribute to this situation. 11 Multiple studies conducted with nurses and physicians working in COVID-19 hospital units, indicate a high prevalence of self-reported feelings of anxiety, depression, psychological exhaustion and BO.5,12 A meta-analysis published in November 2021 demonstrated that nearly half of the HCP experienced burnout during the current pandemic. 13
Purpose
The aim of this questionnaire-based study was to examine how the ongoing pandemic is affecting the mental well-being of HCP working in COVID-19 units in Greece, by calculating the prevalence of BO amongst them, in the course of the third wave of the pandemic.
Materials and Methods
This study constitutes a cross-sectional, questionnaire-based survey aiming to identify the effect of the COVID-19 pandemic on healthcare personnel working in COVID-19 wards. The questionnaire was developed based on the Maslach Burnout Inventory for Medical Personnel (MBI-HSS). 14 The necessary license to use the MBI-HSS was acquired. We used the “Google Forms” online platform (Google, Inc.) to distribute an electronic questionnaire, utilizing the mailing list of the Local Scientific Institution (nurses, midwives and doctors working in COVID-19 wards), between February 21st, 2021 and March 5th, 2021. The mailing list of Local Scientific Institution includes burses, midwives and doctors that work all across Greece and thus allows for a representativeness of the population. Reminder emails were sent 1 week after initial distribution to increase response rate. We also utilized the Facebook account of the Local Scientific Institution, for questionnaire distribution. We didn’t collect data through which the participants could be personally identified. Informed consent was required before questionnaire initiation. The current study was approved by the research and ethics committee of Local Scientific Institution (approval ID: 01/21-02-2021). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
The questionnaire consisted of 35 questions, including the 22 items that constitute the MBI-HSS. The rest of the questions concerned basic demographic data (age, gender, marital status, profession, number of years from graduation) and basic work-related data (number of hours working per week, amount of sleep each night, number of months working in a COVID-19 ward, number of COVID-19 patients that the individual cares for weekly, number of night shifts per month, job satisfaction, thoughts about changing career).
The validated for Greece MBI-HSS calculates the level of burnout (high, moderate, low) of healthcare personnel based on three categories, namely emotional exhaustion (EE subscale), depersonalization (DP subscale) and personal accomplishment (PA subscale). The level of burnout for an individual is considered high if one or more of the following conditions are met: (1) PA subscale score ≤31, (2) EE subscale score ≥27, (3) DP subscale score ≥13. Similarly, the level of burnout is considered moderate if the PA score ranges from 32-38, the EE score ranges from 17-26 or the DP score ranges from 7-12. If none of the above criteria are met, the burnout level is considered low (PA ≥39, and EE ≤16, and DP ≤6). 15 To perform the univariate and multivariate analyses, the moderate and low categories were combined into one category.
All statistical analysis calculations were performed using the GraphPad Prism (version 8.4.0 for MacOS, GraphPad Software, San Diego, California USA, www.graphpad.com). Data are presented as median and interquartile range (IQR)/mean and standard deviation (SD) for quantitative values and as percentages for qualitative values. In the case of categorical variables, the Fisher’s exact and χ2 tests were used, as appropriate, to analyze and test for statistical significance. The statistical significance threshold was set at P = .05. A logistic regression model was used to further study the risk factors associated with a high burnout level. The variables that were significantly associated with high burnout in univariate analysis were used in the regression model. The odds ratio (OR) and 95% Confidence Interval (CI) was calculated for each parameter.
Results
Table Presenting the Basic Demographic Information of the Participants.

COVID-19 = Coronavirus disease 2019.
Overall, 71.6% of the participants had a high burnout score, while 20.5% had a moderate and 7.9% had a low burnout score.
When only the EE subscale of the MBI-HSS was taken into account, 63.7% of the participants had a high, 21.6% a moderate and 14.7% a low burnout score. The median EE score was 31 (21-40). When only the DP subscale of the MBI-HSS was taken into account, 31.1% of the participants had a high, 26.3% a moderate and 42.6% a low burnout score. The median DP score was 8 (3-14). When only the PA subscale of the MBI-HSS was taken into account, 18.4% of the participants had a high, 37.4% a moderate and 44.2% a low burnout score. The median PA score was 38 (34-42.25).
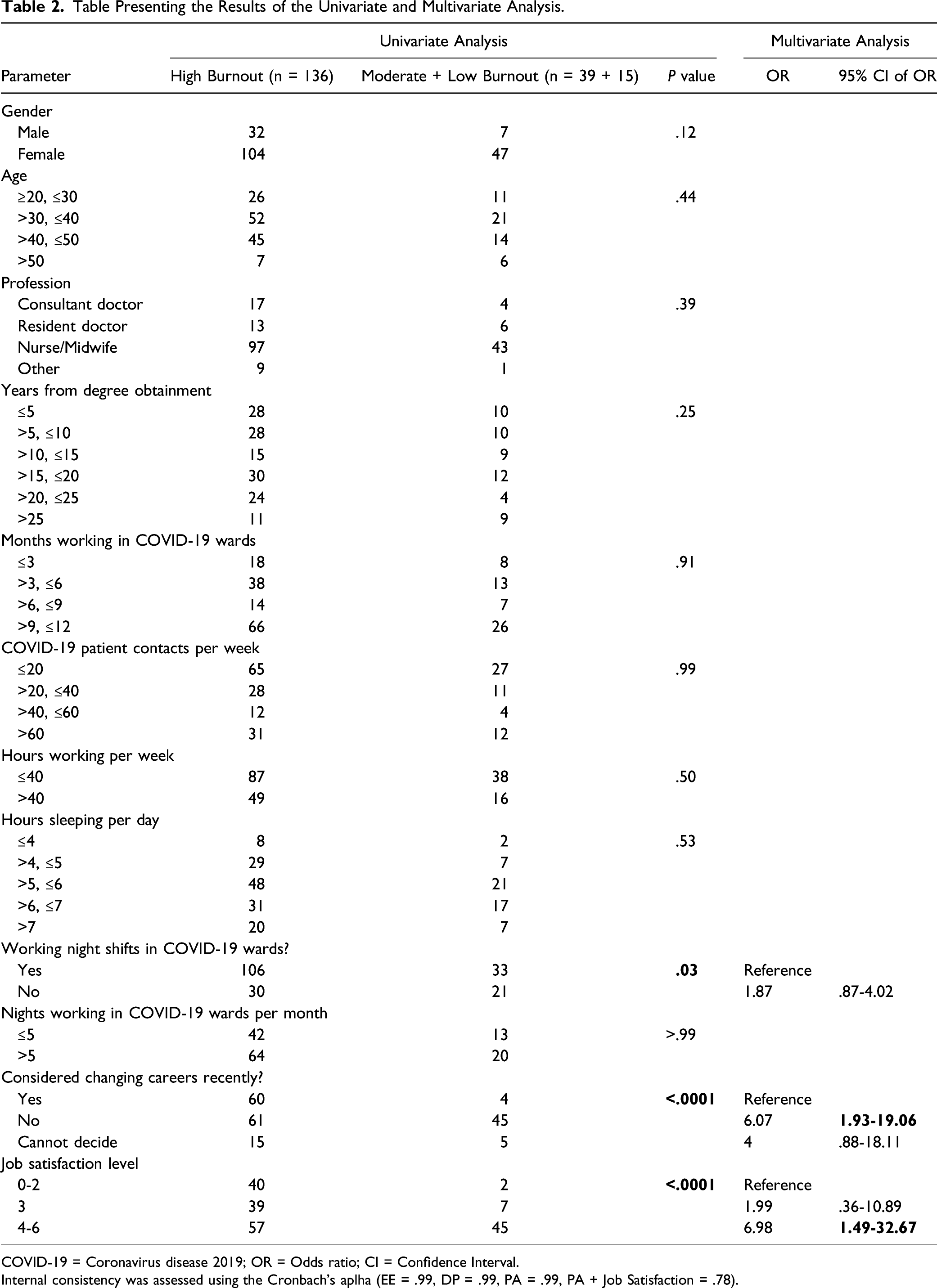
Univariate analysis showed that night shifts in COVID-19 wards (Figure 1A) and job dissatisfaction (Figure 1B) were significantly associated with a high burnout score (P =.03 and P < .0001, respectively). Furthermore, participants with a high burnout level (Figure 1C) were more likely to have thought of changing careers (P < .0001) (Insert Figure 1). In the multivariable testing model, job dissatisfaction [OR: 6.98; 95% CI: 1.49-32.67] and thoughts of changing careers [OR: 6.07; 95% CI: 1.93-19.06] remained significantly associated with high burnout. Table 2 summarizes the results of univariate and multivariable analyses. Figure illustrating the number of participants with high and moderate + low burnout levels on the basis of (A) Night shifts, (B) Job satisfaction, (C) Thoughts of changing career. Table Presenting the Results of the Univariate and Multivariate Analysis. COVID-19 = Coronavirus disease 2019; OR = Odds ratio; CI = Confidence Interval. Internal consistency was assessed using the Cronbach’s aplha (EE = .99, DP = .99, PA = .99, PA + Job Satisfaction = .78).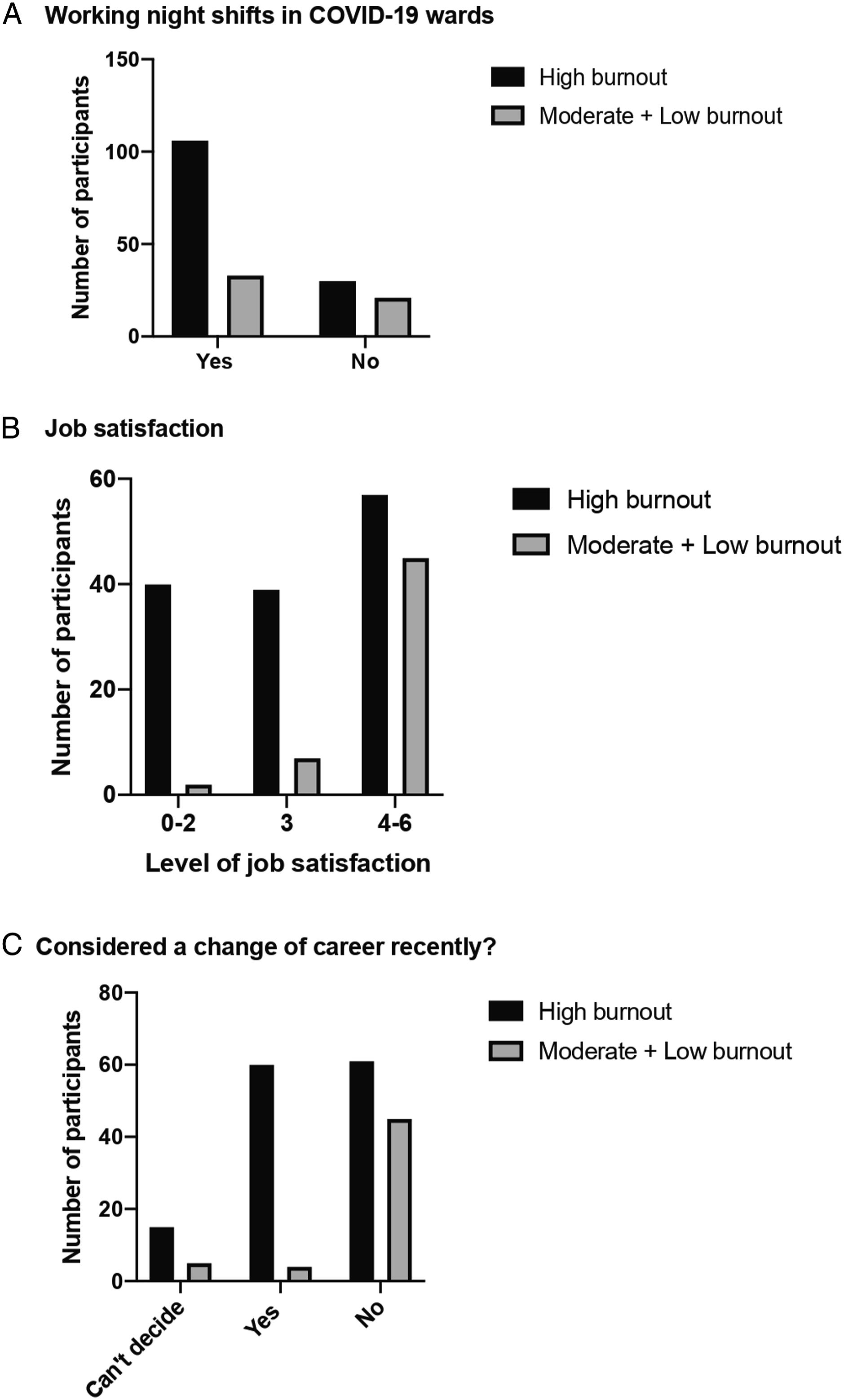
Discussion
Our study intended to identify the aftermath of the psychological stress, as indicated by the level of BO, endured by the HCP working in COVID-19 wards in Greece. Not surprisingly, the majority of the participants in our study are experiencing high levels of overall BO and emotional exhaustion that are associated with two common risk factors, night shifts and job dissatisfaction.
A systematic review investigating the burnout prevalence among HCP in COVID-19 wards, reported that most studies evaluating the mental health of those working in emergency departments, paramedic services and ICUs, showed higher levels of job-related stress, somatic symptoms, and BO. 16 Most studies in the review identified female gender as the most prominent risk factor for developing BO syndrome. Interestingly in our study no difference was found regarding gender. Other studies, not included in the aforementioned systematic review, report significantly higher BO prevalence compared with the pre-pandemic period, among nurses, those reporting thoughts/intention of changing careers and those not getting adequate sleep (due to overtime or night shifts).17,18 Our results regarding plans on changing careers and sleep/night shifts are in line with these reports, while the difference amongst professions was not demonstrated.
In Greece, as in all of Europe, we are presently experiencing the third “wave” of COVID-19 cases, fueled by the new variants. In the beginning of the pandemic in March 2020, the Greek government acted quite proactively and implemented some of the strictest measures in Europe. As a result, the spread of the disease was slowed down, protecting Greek citizens and the national healthcare system. 19 Sadly, the second surge of cases in November 2020 caused unbearable pressure on public health facilities despite the government-enforced lockdown. 20 Following a temporary decrease of cases, the third wave imploded in late January of 2021 with the surge this time centered around the wider area of the capital.
Recently published studies on Greek HCP’s mental health during the initial phase of the pandemic, clearly demonstrated high prevalence of symptoms of moderate/severe depression, anxiety and traumatic stress coupled with particularly high BO levels.21,22 In comparison with a previous study conducted by Pappa et al, 21 our findings show a higher percentage of high BO score in the EE subscale of the MBI-HSS questionnaire (63.7% vs 51.63%), while demonstrating a surprisingly lower percentage of high scores in the PA and DP subscales (18.4% vs 30.29% and 31.1% vs 66.45%, respectively). The higher levels of emotional exhaustion in our study might indicate the accumulation of the psychological and physiological strain on HCP working in COVID-19 units, as the SARS-CoV-2 pandemic is progressing. It can also be explained by the greater toll that the third wave of the outbreak is having on the national public healthcare system as opposed to the first, more “benign” wave. Another explanation could be the fact that only 87% of the participants in the first study were directly involved in the care of COVID-19 patients. The perplexing lower scores in PA and DE subgroups, could indicate the success of HCP in managing the emotional stress in the workplace in a healthy way, as both DE and PA correspond to coping. 9
Depersonalization is a coping mechanism that manifests as indifference towards patients and co-workers as an attempt to reduce the depletion of emotional energy that one is experiencing. The personal achievement score indicates the self-efficacy in adjusting to demanding situations and translates into positively using control as a method of coping. 23 In view of that, lower scores in DP and higher PA scores might signify the acquisition of the ability to manage the COVID-19 related stressors. Studies published in the pre-COVID-19 era concerning the BO prevalence in HCP in Greece, reported similar PA and DE scores to the study by Pappa et al.24,25 This finding may suggest that by facing an unprecedented, prolongedly stressful situation, such as the COVID-19 outbreak, HCP might build resilience and employ more preferable coping mechanisms.
Despite the indication of better management of the intensified mental strain during the pandemic, there are still major concerns regarding the high scores of BO in HCP found in our study. Scoring high in MBI-HSS and especially in the EE subscale has been associated with poorer quality of healthcare, reduction in patient safety due to medical errors and increased absenteeism.26,27 Unfortunately, BO syndrome in HCP has also been associated with high levels of anxiety and depression28,29 whereas multiple studies in various specialties link BO to physicians’ suicidality.30,31
As of April 2021, 16 vaccines against COVID-19 have been authorized by at least one national regulatory authority for public use. At the moment (June 2021), almost 2 billion vaccine doses have been administrated. 2 Alas, new variants of SARS CoV 2 are appearing globally, four of those being currently of concern [20I/501Y.V1(UK), 20H/501Y.V2 (South Africa), 20J/501Y.V3(Brazil), G/452R.V3(India)]. These variants were found to have increased transmissibility, to cause higher rates of severe disease and hospitalizations and to be connected with post-vaccine neutralization reductions. 32 It is evident that during the following months the strain on the public health care system will continue to mount. Subsequently, there is a profound need for continuous monitoring and evaluation of the BO levels of HCP especially during demanding times in healthcare. Besides, the notion of using effective techniques and methods for building resilience in times of intensified work-related stress in healthcare has been increasingly appearing in the literature in light of the COVID-19 pandemic.33,34
The study has some key limitations that should be acknowledged. In an effort to only use standardized questions, our survey only included a small number of additional questions besides those of the MBI-HSS, limiting our understanding of other potential risk factors. Additionally, the lack of data from a comparative group not working in COVID-19 units does not allow us to definitively connect COVID-19 with the high BO scores found in our study.
Conclusion
Our study highlighted that the majority of HCP working in COVID-19 wards in Greece is experiencing high levels of overall BO and emotional exhaustion. Work related factors that contribute to the BO are night shifts and job dissatisfaction.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
Data can be made available upon request.