
Abstract
The purpose of this study was to determine whether weight bias exhibited by health care professionals (HCPs) impacts quality of health care provided to individuals with obesity. HCPs (n = 220; 88% female, 87% nurses) in the Midwest region of the United States were recruited to complete an online survey. In this within-subjects study design, participants completed the Attitudes Towards Obese Persons (ATOP) scale to assess weight bias and responded to 2 (1 person with obesity and 1 person without obesity) hypothetical patient scenarios to evaluate quality of care. A median split was calculated for ATOP scores to divide participants into high or low weight bias groups. Within these groups, thematic analysis was used to uncover themes in quality of care based on participants’ responses to each scenario. The analysis revealed that HCPs in the high weight bias group gave specific diet and exercise recommendations, offered health advice regarding weight loss, and used less teaching discourse when responding to the patient with obesity. In addition, in both weight bias groups, patients with obesity were started on pharmaceutical therapies sooner. The findings of this study suggest a need to educate HCPs on the importance of empathy and compassion when providing treatment to all patients, regardless of weight, to increase quality of care and ultimately improve patient outcomes.
Health care professionals exhibit weight biases and these biases may impact quality of care delivered to obese individuals.
This study provides evidence that there are notable disparities in quality of health care provided to patients with obesity compared with patients without obesity.
The findings of this study suggest a need to educate HCPs on the importance of empathy and compassion when providing treatment to all patients, regardless of weight, to increase quality of care and ultimately improve patient outcomes.
Introduction and Background
Weight bias, defined as negative attitudes or judgments toward people with obesity based on stereotypes, has been reported in a variety of environments including health care settings. 1 Weight bias can generate discrimination, which is a known barrier to health care and healthy lifestyle behaviors in other vulnerable populations such as HIV/AIDS patients. 2 People who feel stigmatized in health care settings, including people with obesity, report many barriers to seeking health care,3,4 thus perpetuating health disparities. If people with obesity do not feel comfortable or welcomed in a health care setting, they may not seek out health care and therefore not receive the treatment and counseling they need to improve their health status.
Health care professionals (HCPs), including physicians, nurses, dietitians, and psychologists, exhibit weight biases. 5 Furthermore, Miller et al found that 72% of surveyed medical students expressed weight bias when interacting with patients. 6 The negative attitude of HCPs toward obese patients may inadvertently affect quality of health care delivered to obese patients.
It has been suggested that there is a need to understand whether HCP weight biases affect quality of health care. 5 While it is established that many HCPs have weight biases,2,5-9 it is less understood whether this affects quality of health care provided. Studies show that HCPs perceive populations with obesity nonadherent to health recommendations, 10 show less respect, 11 and provide less health education compared with those without obesity. 12 Furthermore, physicians tend to build less rapport and create weaker relationships with patients with obesity compared with patients with normal weights. 13 While these negative quality of care outcomes have been recognized, they have not been connected to HCP weight bias. In fact, studies evaluating weight biases effect on quality of care have suggested that weight bias does not affect clinical recommendations, though overall, evidence is mixed.5,14,15 Understanding how quality of care is affected by negative attitudes toward obese people may provide insight on how to improve the health of this population. The purpose of this study was to evaluate whether HCPs in the Midwest region of the United States exhibit weight bias toward patients with obesity and to determine if, and how, weight bias affects quality of care.
Methods
Participant Recruitment and Data Collection
Prior to participant recruitment, this protocol was approved by the Illinois State University Institutional Review Board. Inclusion criteria were as follows: must be a HCP practicing in the Midwest region of the United States (Illinois, Indiana, Iowa, Kansas, Michigan, Minnesota, Missouri, Nebraska, North Dakota, Ohio, South Dakota and Wisconsin), be above the age of 18 years, and be able to read and write in English. Invitations to complete this online survey were distributed by professional practice directors to hospital employees on a voluntary basis. Participants provided informed consent by clicking “agree” on the informed consent form prior to accessing survey questions. Select Survey Software was utilized to administer the survey.
Demographic questions, including questions about race, age, self-reported height and weight, and education level, preceded quality of care and weight bias measurements. Respondent self-reported height and weight was used to calculate body mass index (BMI). Quality of care was measured by open-ended responses to hypothetical patient scenarios, which are validated tools used to evaluate quality of care.16,17 Each scenario contained information about a hypothetical patient’s height, weight, BMI, sex, and new diagnosis with hypercholesterolemia. Scenarios were identical with the exception of patient BMI and sex and were accompanied by a picture of a male or female with the BMI described in the scenario. HCPs received the male or female scenarios at random. The images of BMI categories have been previously validated to measure weight concepts 18 such as weight bias. Quality of care was measured by within-subjects analysis of how the HCP responded to the scenarios and whether he or she responded differently to patients of different weights. Therefore, each participant responded to a scenario involving a person of normal weight and a person with obesity that were identical in every way except for their weight and thus, BMI. The 20-item Attitudes Towards Obese Persons (ATOP) scale, (α = .72) a previously validated weight bias assessment tool with high internal consistency,19-22 was used to evaluate weight bias. The ATOP scale was developed for use in the general population and has been tested for theoretical clarity, content, structure, and convergent validity.19,21,22 In addition, this scale has been shown to be sensitive to change when targeted by an intervention. 23 Participants responded to patient scenarios before completing the ATOP scale questions. It was estimated that it would take participants less than 20 minutes to complete the survey. Participants who completed the survey had the opportunity to enter their name and contact information in a raffle for one of two $100 Amazon gift cards.
Data Analysis
Descriptive statistics were calculated to summarize participant demographic data using the Statistical Package for the Social Sciences (SPSS for Windows, version 21, SPSS, Inc, Chicago, Illinois). For the ATOP scale, a median split divided participants into “high weight bias” and “low weight bias” groups. Using a within-subjects design, responses to scenarios by weight bias groups were then coded to identify themes among the high and low weight bias groups using thematic analysis. The responses were read and coded individually by 2 researchers, a graduate student and a faculty advisor, after all data had been collected and incomplete responses were omitted. Each researcher coded and took notes related to the codes. After each researcher completed data analysis, the researchers met to discuss codes until consensus was reached. If there was disagreement about a code, each researcher revisited the data and it was discussed until agreement was reached. From this final coding scheme, the themes were developed.
Results
A total of 335 people accessed the survey, but due to incomplete responses, 135 were excluded from the final analysis. Incomplete response rate was similar regardless of the scenarios participants were exposed to. Researchers hypothesize incomplete responses were related to the length of the survey. Participants (n = 220) were mostly female (88%) nurses (87%) practicing in Illinois (99%) (Table 1). Most respondents were 26-35 years old (35.9%) and 50% had worked in health care for less than 10 years. The ATOP score of participants ranged from 35 to 117 (high weight bias to low weight bias, respectively) with a mean ATOP score of 73.18.
Characteristics of Health Care Professionals (n = 220).

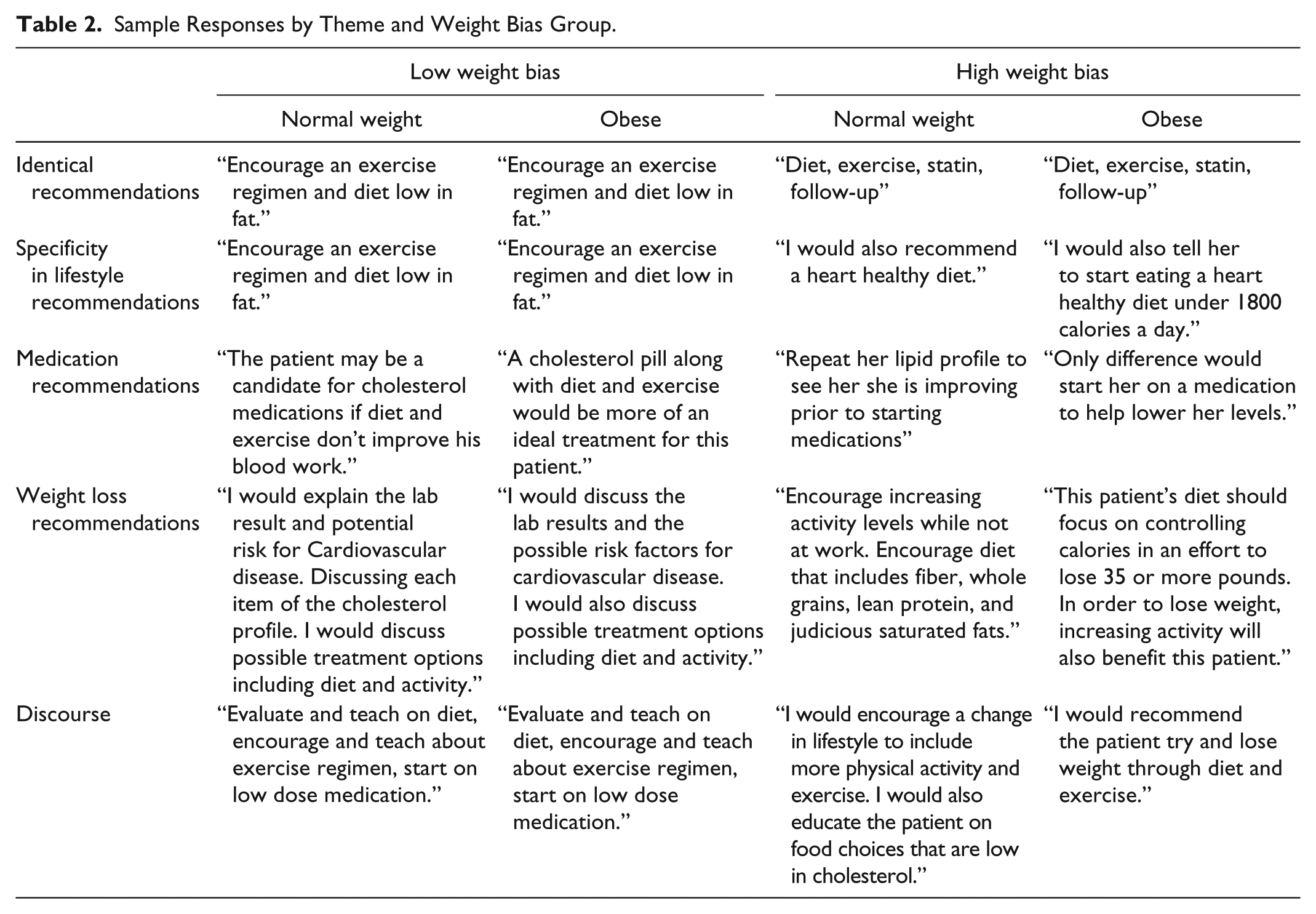
Overall, diet and exercise modifications and medications were recommended by high and low weight bias groups. When comparing the high versus low weight bias groups, a total of 5 major themes were identified: (1) identical recommendations, (2) specificity in lifestyle recommendations, (3) medication recommendations, (4) weight loss, and (5) discourse (Table 2).
Sample Responses by Theme and Weight Bias Group.
Identical Recommendations
For the first theme, it was found that, in both weight bias groups, identical recommendations were given by the health professionals. This means that if HCPs discussed diet and exercise with the normal weight patient, they also discussed these same topics with the patient with obesity. Furthermore, responding to both patients with “encourage an exercise routine and [a] diet low in fat” or “I would give this [obese] patient the same information as the previous [normal weight] patient” were coded as identical recommendations. Offering identical recommendations may indicate no difference in quality of care delivered to the obese versus normal weight patient.
Specificity in Lifestyle Recommendations
When recommendations differed between the patient of normal weight and the patient with obesity, the HCPs in the high weight bias category prescribed diet and exercise recommendations with more specificity for the patient with obesity. While HCPs in both weight bias groups used general terms such as “heart healthy diet,” “low fat/low cholesterol diet,” and “diet modifications” with all patients, “strict” and “drastic diet modifications” were recommended to patients with obesity. HCPs in the high weight bias group recommended, only to patients with obesity, “eating a heart healthy diet under 1800 calories a day,” or a “low carb, high protein diet.” Similarly, HCPs in the high weight bias group assumed the patient with a healthy BMI could “add some walking” or “increase her exercise” routine, whereas the patient with obesity should “start walking” or “begin an exercise program.” The low weight bias group tended to advise both patients to “increase physical activity level” or “become more active,” and not make assumptions about the patient’s current exercise habits. It was noted that HCPs in both weight bias groups encouraged “higher intensity workout regimen[s]” in the population with obesity, recommending “working out 3-4 times a week” or “30-60 minutes per day” versus the “2-3 times a week” or “30 minutes per day” deemed sufficient for the normal weight population.
Medication Recommendations
HCPs in both weight bias groups were likely to start patients with obesity on statin drugs immediately. In contrast, HCPs recommended statins to patients without obesity once lifestyle modifications proved ineffective. Though this happened in both weight bias groups, it was a more prominent theme in the high weight bias group. For instance, one HCP suggested that the normal weight patient “may be a candidate for cholesterol medication if diet and exercise don’t improve his blood work.” The same HCP suggested to the patient with obesity that “a cholesterol pill along with diet and exercise would be a more ideal treatment for this patient.”
Weight Loss
Patient weight was a more prominent theme found among HCPs in the high weight bias group counseling patients with obesity. In addition, lifestyle modifications were sometimes addressed in the context of weight loss, not for improving cholesterol levels. For instance, HCPs recommended that patients with obesity “needing to start exercising to lose weight,” “controlling calories in an effort to lose 35 or more pounds,” and needing a “diet and exercise regimen in order to lose his extra weight.” On the contrary, diet and exercise modifications in the healthier weight counterparts were aimed toward achieving healthy cholesterol levels.
Discourse
The type of discourse that high weight bias HCPs used in their responses was also a theme. The use of words that carry positive connotations related to patient-centered care, such as education and encourage, was more prominent in the responses of the person of normal weight. The fact that HCPs with high weight bias did not utilize these teaching words with patients with obesity may indicate a less friendly, nonempathetic provider-patient relationship, which may negatively impact quality of care.
Discussion and Conclusion
Overall, thematic analysis revealed that HCP responses to scenarios were similar regardless of weight bias; however, differences also emerged. It was a larger theme among HCPs with high weight bias to offer different recommendations to patients with obesity than HCPs with low weight bias. Differences included specific diet and exercise advice, emphasis on pharmaceutical intervention, prominence of lifestyle modifications aimed toward weight loss, and the use of less empathetic discourse. These contrasts may create a different health care experience for patients with obesity compared with patients without obesity, impacting quality of care.
The discourse theme noted in this study is consistent with past studies. Bertakis and Azari highlighted that HCPs spend less time giving patients with obesity health education compared with others. 12 While this study did not measure time, qualitatively, teaching discourse was not a theme in the HCPs with high weight bias when counseling patients with obesity and this deserves attention in future studies. If HCPs with high weight bias are limiting the teaching discourse with patients with obesity unknowingly, this may contribute to weaker practitioner-patient rapport, which women with obesity report being among the most important factors in health care settings. 4 Furthermore, education and encouragement are elements of patient-centered care which contributes to higher quality of care. Education and encouragement help increase patient self-efficacy, which, according to the Health Belief Model theory of behavior change, is necessary in promoting healthy lifestyle modifications 24 and achieving better health status.
The discourse may also suggest the possibility that HCPs express less empathy toward populations with obesity. Empathy and compassion allow patient-centered health care to succeed. 25 Positive provider-patient relationships have been shown to improve adherence to recommendations 26 such as diet and exercise modifications. Lown and colleagues found that physicians and patients consider compassionate health care to be very important (76% and 85% respectively), but less often see it practiced (58% and 53%, respectively). 25 However, as this study only evaluated online responses to hypothetical scenarios, it is unclear if these words would be used with patients or not. Instructing HCPs on the power of compassionate care may improve the health outcomes among the population with obesity by creating a more positive health environment and ultimately affecting quality of care.
Multiple sources identify the tendency of HCPs to focus on weight loss when addressing patients with obesity.5,8,12 While this does not necessarily indicate poor quality of care, discussing behavior modifications aimed toward weight loss ignores the actual questions presented by the patient. In this study, HCPs provided recommendations aimed toward weight loss and did not directly address cholesterol levels when counseling patients with obesity. Providing information regarding weight loss instead of “desired health outcomes” disobeys the Institute of Medicine’s definition of quality of care 27 and therefore, could be considered an indicator of poor quality of health care. In turn, it could be said that in this study, patients with obesity received lower quality of care.
The tendency of HCPs to more readily prescribe statins to patients with obesity may indicate that HCPs in both weight bias groups anticipated nonadherence to lifestyle recommendations. HCPs seemed willing to try diet and exercise modifications among nonobese patients and reevaluate the necessity of pharmaceutical intervention at a later date. On the contrary, participants seemed hesitant to recommend diet and exercise before beginning statins to patients with obesity. This may be attributed to a lack of confidence that patients with obesity would practice lifestyle modifications. This parallels past findings that higher patient BMI is associated with HCP perceived lower adherence to medication usage, 10 alluding to a degree of patient mistrust. This, in conjunction with absence of teaching discourse, empathy, and attention to patient concerns can further contribute to decreased quality of care delivered to patients with obesity.
Some of the strengths of this study include sample size and validity of data collection tools. The ATOP scale and use of scenarios are previously validated tools merited for measuring weight bias and quality of care respectively,16,17,20 and use of pictures to depict patient BMI further strengthened the study design by providing visual representation of the hypothetical patients. 18
While the within-subject design of the survey helped gather responses comparing how an individual reacted to the 2 scenarios, it also may have offered insight into the researchers’ hypotheses. If participants were able to identify aim of this study, it is possible that it affected responses to the scenarios. Because the sample consisted of mostly female nurses practicing in Illinois, conclusions may not be generalized. In addition, many participants who started the survey or consented to participate did not complete the survey. It is unknown why these participants did not complete the survey; therefore, these results are not generalizable to all HCPs. Furthermore, the survey was distributed online, eliminating possible information regarding body language and time spent on the survey. The data collection methods used did also not differentiate between implicit and explicit weight bias. Understanding whether HCPs were aware of their biases and if awareness of bias altered the expression of weight bias may have added further dimension to the findings. The data collection methods were also hypothetical. Even though responses to hypothetical scenarios are a valid method for evaluating quality of care, it is unknown how these practitioners would respond to actual patients with the given diagnosis and weight status. To address these shortcomings, future studies should attempt to observe interactions and/or investigate the patient’s perception of quality of care.
While the ATOP scale is a valid and reliable method to assess weight bias for the general public, this study did use a median split to categorize HCPs as “high weight bias” or “low weight bias.” This allowed the researchers to examine differences in scenario responses; however, weight bias is likely much more complex and varied than 2 categorical levels. Future studies could attempt to understand how varying quantitative measures of weight bias relate to responses to hypothetical scenarios.
Future research may benefit from comparing how different HCPs interact with patients of different weight categories. Furthermore, research is needed comparing HCP weight bias and quality of care in different settings, for example, outpatient versus inpatient, and in different geographical areas, such as urban versus rural communities. Because this research utilized hypothetical patients, research may benefit from analyzing face-to-face provider-patient interactions. More research evaluating methods of eliminating weight bias from the health field would be valuable in ensuring HCPs deliver consistent quality of care across the patient population.
Overall, this study provides evidence that there are notable disparities in quality of health care provided to patients with obesity compared with patients without obesity. While it was a prominent theme among the HCPs in the high weight bias group to treat patients with obesity differently, HCPs in the low weight bias group also provided different medication recommendations to this population. The findings of this study suggest a need to educate HCPs on the importance of empathy and compassion when providing treatment to all patients, regardless of weight, to increase quality of care and ultimately improve patient outcomes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.