
Abstract
Purpose
The impact of a hospital formulary was evaluated to provide a guide for the establishment of local formularies to optimize patient care and healthcare costs.
Methods
A formulary was introduced by formulary pharmacists of the Toda Medical Group for suggesting recommended medicines to physicians based on the medication history. Patients who were hospitalized in the rehabilitation ward of the Niiza Hospital and prescribed medicines according to the formulary introduced between April 2017 and March 2018 were included and followed-up for six months.
Results
Of the 183 patients screened, 154 patients were enrolled as the formulary’s introduction patients (76 males/78 females, median age 78 years); 92% of these patients received formulary-proposed prescriptions at the specified timepoints; and 19 patients re-consulted at the Niiza Hospital after discharge and continued the same formulary medicines. The proposed acceptance rate by physicians was 100%. Most changes suggested introduced generic formulations. The doses were equivalent for all pharmacological classes with the exception of medicines that interfere with the renin–angiotensin system, which fell from 10.7 to 7.2 mg (P< .0001). Overall daily medication costs fell at discharge compared to admission (38.5 vs. 94.6 yen per patient, respectively, P< .0001). This was valid for all pharmacological classes except for calcium channel blockers.
Conclusion
Hospital formulary-prescribed medications continued after discharge and promoted significant decreases in costs associated with outpatient prescriptions. Introducing a hospital formulary provides a basis for the introduction of local formularies and contributes to the reduction of local healthcare costs.
Formularies, which are guidelines for effective, safe, and the economical use of medicines, are considered a tool for the appropriate use of medication. Hospital formulary-prescribed medicines were continued after discharge, and can contribute to the reduction of local healthcare costs in countries with universal healthcare coverage and in countries that plan to introduce local formularies by similar approaches. This study validates a strategy to standardize medication prescription based on the local needs of the community and could decrease the burden on the national healthcare system while also providing improved patient care.HighlightsWhat Do We Already Know About This Topic?
How Does Your Research Contribute to the Field?
What Are Your Research’s Implications Towards Theory, Practice, or Policy?
Introduction
Formularies are guidelines for the effective, safe, economical, and appropriate use of medications. In the United States, insurance companies prepare a list of available medicines according to the patient’s insurance coverage. 1 In Europe, formulary systems are linked to guidelines, protocols, and treatment pathways based on the best available evidence, including patient outcomes and pharmacoeconomic assessments.2-5
In Japan, the universal health insurance system allows free prescription of approved medicines according to the patient’s insurance plan. Japan’s medical system covers all citizens with public medical insurance and allows them to freely choose their medical institutions. 6 It is based on a social insurance system, while public funds are used to maintain universal health coverage. France is a country that has an insurance system similar to that of Japan.7,8 In the United Kingdom, outpatient co-payment is free of charge in principle, which is different from Japan. 7 Sweden has also introduced a tax-based public health insurance service, 9 and the amount of co-payment for outpatients is decided independently by the local government. The U.S. insurance system is limited to public healthcare, with Medicare provided by the federal government for seniors 65 and older and the disabled, and Medicaid provided by state governments for those with low incomes. The only way for working-age people to obtain medical coverage is to purchase medical insurance from private insurance companies.
Considering cost optimization with the appropriate use of medicines, Japan falls behind other countries with formularies. As Japanese patients sometimes request cost-conscious medications, a formulary has been established in each hospital. France, which has a social security system similar to Japan’s, has established a hospital formulary. 5 In countries that have a tax system, such as the United Kingdom or Sweden, national formularies or local formularies have been introduced. Local formularies are also more advanced in the U.S., where hospitals cooperate with each other to set the same formulary. 10 In countries with national and local formularies, a national or local government system is used to coordinate the setting of the amount. The impetus in Europe and the United States is toward the creation of national formularies, similar to a universal healthcare system. 1 Such Japanese universal healthcare system formularies are useful for the development of the medical industry.
In Japan, the expectation of formularies had been noted since 2000 in research studies funded by the Ministry of Health, Labor and Welfare. 11 In 2017, a paper on the formulary system was published. 12 After that, reports continued to demonstrate that hospital formularies showed positive effects toward the appropriate use of drugs and a decrease in the number of adverse drug reactions.13-17 Regional collaboration of formularies is also expected to reduce drug costs. Although local formularies began in some regions in 2019, a study discussing their impact on regional healthcare published in 2021 also shows expectations for their introduction. 18
In Japan, hospitals are available for providing both inpatient care and outpatient prescriptions. Hospitals are classified according to the scale of their functions. Small- or medium-sized hospitals or clinics are often in charge of local medical care. Some chronic care hospitals have a community-based integrated care ward, which comprehensively ensures the provision of healthcare, nursing care, prevention, housing, and livelihood support to care for patients when they are discharged. Other hospitals have a rehabilitation ward for care after the acute phase. The Niiza Hospital has both of these facilities.
Patients are often discharged from acute-care hospitals to their homes via chronic care hospitals in Japan. 19 Depending on the medicines available at each hospital, it is sometimes necessary for a patient to change medications to other agents of the same class. Furthermore, when patients visit local clinics after discharge, clinic physicians can freely choose medications from among those that are approved in Japan. However, long-term treatment should be aimed at providing seamless medical care with a view to ensure treatment continuity. 20 To achieve seamless, safe, effective, and economical community-based medical care, with only minor changes in the medicines taken after each hospital transfer, it is important to introduce common formularies optimized for the community (local formulary) and to provide community-based medical care.
Here, the impact of introducing a hospital-based formulary (hospital formulary) on Japan’s universal health insurance system was evaluated. The medications prescribed after hospital discharges were investigated by clarifying the impact of the hospital formulary on outpatient prescriptions and treatment cost. This study is expected to provide a model for the establishment of local formularies in Japan.
Materials and Methods
This retrospective cohort study focused on hospitalized patients who were admitted to the convalescent rehabilitation ward of the Niiza Hospital.
Setting
Japan’s total population is 125.3 million as of 2021. 21 Total hospital beds per 1000 population is 12.8, which is the highest among Organisation for Economic Co-operation and Development countries. 22 In 2021, Japan had a total of 963 309 general hospital beds and 291 651 convalescent hospital beds. 23 Of those, the number of beds located among the four capital city prefectures are 213 489 and 57 966 beds, respectively. 23 Toda Medical Group (TMG) operates mainly in the four capital cities, and accounts for 3816 beds (1.8%) and 1170 beds (2%), respectively. 24
Formulary System
Figure 1 comprises a schematic of the system for constructing the formulary introduced by the TMG. Among 350 TMG pharmacists, those with experience in medicine information, infectious diseases, psychiatry, and community medicine, among others, were recruited to form a 10-member team to operate the formulary (formulary pharmacists). These formulary pharmacists created a draft list of medications. After the draft was approved by the Pharmaceutical Affairs Council of each hospital, the formulary was introduced. The Pharmaceutical Affairs Council consists of the hospital director, the chairman of the Pharmaceutical Affairs Review Committee (a physician), eight other physicians, the administrative director, the head of the nursing department, one head pharmacist, and two clerks in Niiza Hospital. Formulary pharmacists conducted systematic reviews or used the Cochrane Database of Systematic Reviews (CDSR) to collect comprehensive information, which was then used to objectively evaluate medicines and to create priorities for medication adoptions.
25
Thereafter, pharmacists at each TMG hospital introduced the system based on the formulary drafts Hospital formularies and social network of the Toda Medical Group (TMG) in Japan. The Formulary Team of the Toda Medical Group Pharmaceutical Department conducts a systematic review of each medicine’s effect, sets equivalent doses, ranks recommendations, and prepares a draft of a formulary that can be applied at the TMG hospitals. Based on the draft formularies, each hospital constructs formularies according to the patient population of the hospital. As patients move from acute-care hospitals to chronic care hospitals, medicines used may change due to alterations in the patient’s conditions. It is possible to implement a standardized treatment by using the same draft formularies. As physicians choose medicines based on the hospital formulary, it is expected that this will lead to the establishment of a local formulary in the future.
Based on the formulary, the pharmacists of each TMG hospital could propose alternative medicines to physicians in cases when different medications had been previously prescribed to patients. In the Japanese healthcare system, patients can visit any medical institution of their choice. If the pharmacists decide that a change in medication is necessary, the pharmacist proposes a formulary medicine and indicates an equivalent dose to the physician. Then, the proposed medicines are confirmed by the physician, and the physicians prescribe the medicines. After the approval of the proposal, the pharmacists and nurses coordinate to monitor the patient’s condition during hospitalization (mean duration 90 days) 12 and share the information with the medical community upon discharge.
Data Source
The authors used the data on the medicines used at the time of admission for hospitalized patients who were admitted to the convalescent rehabilitation ward of the Niiza Hospital between April 2017 and March 2018. Outpatient prescription data from April 2017 to March 2019 was utilized as follow-up data Data points when medications were identified during data source creation and study period. The following points were identified: (1) At the time of hospitalization, alternative medicines were proposed for local prescriptions, (2) Whenever there were prescription changes, (3) At hospital discharge, (4) At return visits after discharge.
Cohort Study
Patients hospitalized in the rehabilitation ward and prescribed medicines from the introduced formularies were selected for participation in this study. Those patients whose medications were changed based on the formularies were selected and, among them, those whose prescriptions remained unchanged at the time of discharge were defined as the formulary’s introductory patients (n = 154). The patients who returned to our hospital for outpatient visits within six months of receiving a prescription based on the formulary and those who continued to take the formulary-specified medications were defined as the formulary’s continuation patients Flowchart of the study participant selection and evaluation timepoints.
Variables
The generic names and daily doses of medications were obtained. The formulary classes (recommended medications) that had been introduced in the Niiza Hospital until March 2017 included angiotensin-converting enzyme inhibitors/angiotensin 2 receptor blockers (of the renin–angiotensin system [RAS]s; enalapril; or telmisartan if enalapril was not tolerated), proton pump inhibitors (PPIs; lansoprazole), xanthine oxidoreductase inhibitors (XORis; allopurinol; or febuxostat if allopurinol was not tolerated), 3-hydroxy-3-methylglutaryl-coenzyme A reductase inhibitors (HMG-COA reductase inhibitors; atorvastatin), calcium channel blockers (CCBs; amlodipine or nifedipine extended-release tablets [twice-daily formulation]), and an α-glucosidase inhibitor (AGI; voglibose).
Statistical Analysis
Dose equivalence of the medications that were proposed as substitutes by the hospital formulary.

aFormulary-recommended medicines in each region.
bOff-label dosage in Japan.
Medication costs were calculated based on the following factors: the Japanese National Health Insurance (NHI) price of the medications taken at the time of hospital admission, medicines listed at discharge, and those prescribed at the revisit to the Niiza Hospital after discharge. The total daily medication costs were defined as the sum of the 753 prescriptions taken by the patients (n=154). In fixed-dose combinations of RAS and CCBs, RAS cost was derived by calculating the NHI price of the combination medicine minus the lowest NHI price of the CCB generics. The data were converted at the currency rate of 104.76 JPY to $1.00 (October 23, 2020) and listed along with the value in Japanese yen. The Wilcoxon signed-rank test was used to compare the dosages and medication costs. The significance level was set at P<.05. In this study, we did not conduct a comparative analysis between the formulary introduction group and the non-introduction group, because we assumed an imbalance between the number of two groups based on previous studies and because it is difficult to secure the number of patients to conduct a non-inferiority study.
Results
Of the 183 admitted patients, 154 (76 males/78 females, median age 78 years [25th and 75th percentile: 69, 85], median length of stay 89 days [64, 159]) were eligible for registration in the formularies and their medications were prescribed according to the formulary
Of the 154 cases (324 prescriptions), 297 (92%) and 27 (8%) prescriptions were formulary-prescribed at the time when alternative medicines were proposed or when new medicines were introduced during hospitalization, respectively. The proposal acceptance rate by physicians was 100%. None of the proposed medications was switched during hospitalization. Of the 154 patients prescribed formulary-recommended medicines during hospitalization, 19 patients re-consulted at the Niiza Hospital within six months, and the others followed-up at other local hospitals or clinics. The formulary-recommended medications prescribed to these 19 patients continued being used.
Number of patients and doses taken at the time of admission and at discharge.

aDose converted by the recommended medicine for each region (including the cases that received no medicines); SD standard deviation.
The changes of dose equivalents for formulary medicines from hospitalization to discharge are shown in Table 2. For RAS, the dose of the enalapril equivalent changed from (mean ± standard deviation) 10.7 ± 5.0 to 7.2 ± 2.6 mg (P < .001). For the other pharmacological classes, there was no significant change in dose equivalents. For HMG-CoA reductase inhibitors, the doses of the atorvastatin equivalent were 7.8 ± 3.9 and 7.0 ± 3.2 mg (P = .124), respectively, on hospitalization and discharge. For CCBs, the doses of the amlodipine equivalent were 5.7 ± 3.1 and 5.4 ± 3.0 mg (P = .442). For XORis, the doses of the allopurinol equivalent were 73.3 ± 62.3 and 96.7 ± 48.1 mg (P = 0. 086). For PPIs, the doses of the lansoprazole equivalent were 15.9 ± 7.0 and 15.2 ± 3.6 mg (P = .408). For the AGI, the doses of the voglibose equivalent were .5 ± .2 and .6 ± .1 mg (P = .317).
Comparison of the total daily medication costs (n = 154 753 records).
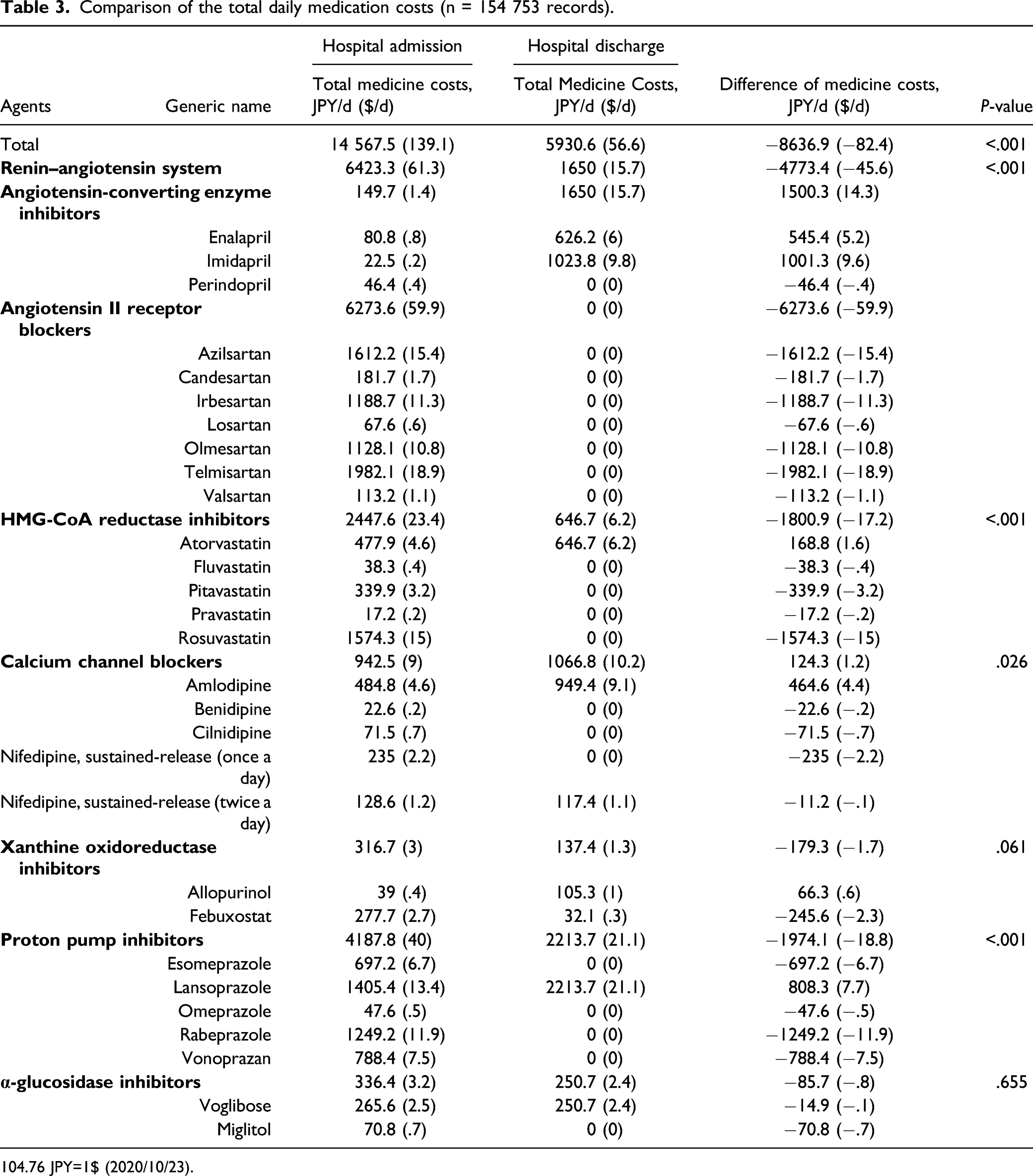
104.76 JPY=1$ (2020/10/23).
Discussion
We found that 89% (17/19) of patients continued to take medicines that were recommended based on the hospital formulary in cases wherein the patients revisited the same hospital. The maintenance rate of hospital formulary-recommended medication was 80%. 12 The adherence to the hospital formulary was therefore maintained when patients revisited the same hospital after discharge.
Here, the prescriptions for a proportion of patients who visited the same hospital were examined. Even in cases when the patients were discharged from the hospital and visited another hospital, when the patients were seen again one year later, and there was no change in the prescription contents; that is, the same medicines continued to be prescribed. If there was no change in the patient’s condition and there was no need to change the prescription, then, as expected, the prescription that was proposed or changed based on the hospital formulary was maintained. The authors consider that the introduction of formularies in hospitals can be a precursor to the introduction of local formularies.
The introduction of the hospital formulary had an impact on outpatient prescriptions. As conversion of healthcare systems is difficult, integrating the method of introducing formularies in each country will be necessary. In countries with a tax system, such as the United Kingdom and Sweden, the ability of the national and local governments to determine the amount of co-payments for outpatients may have made the establishment of national or local formularies possible. In contrast, local formularies are available in the U.S., which has an insurance system limited to public healthcare. Hospitals cooperate with each other to set the same formulary. 10 The limitation in hospital-to-hospital formulary seems that it is assumed that non-participating hospitals will not follow the formulary. The reason why local formularies have been partially introduced even in such environments is that local physician decision-makers have been able to coordinate and modify their opinions with panel members. There are many medical institutions in Japan that provide outpatient as well as inpatient care. Introducing this system in hospitals will bring us one step closer to a local formulary in the future. France, a country with a similar medical system to Japan, has already introduced a hospital formulary. The two countries have also introduced a family doctor system. Based on the examples of countries that have successfully implemented local formularies, there needs to be a common consensus in the local districts. Local formularies will need to be coordinated and explained to the community, especially to family doctors, with the understanding that they can be modified if opinion of the doctors differs from recommendation of the Hospital formulary.
For the hospital formulary, the rate of prescription changes in response to pharmacists' suggestions was 100% in this study. Japan has a universal health insurance system, which means that all approved medicines can be prescribed. 40 The high approval rate for evidence-based prescribing by physicians 40 implies that they approve the evidence-based suggestions made by pharmacists. This strategy has the potential to reduce the prescribing burden on physicians. In addition, 92% of the formulary medicines introduced were based on the identification of medicines available locally. The timing of suggestions for the appropriate use of medicines was important to introduce formulary medicines. Under these circumstances, all proposals based on the hospital formulary were approved and the medicines were switched after verifying the medications were available locally, indicating the hospital formulary was well managed.
Pharmacists are expected to take responsibility for the pharmacotherapy of patients for whom the prescription is proposed. Though a means of ensuring the appropriate use of medications, currently in Japan, it is not compulsory to apply a formulary for patient prescription. Here, medicines other than those recommended by the formulary were not prescribed during hospitalization when the condition of the patient remained unchanged. In cases where the patient’s medication upon admission was identified, the appropriateness of the formulary medication proposal was determined while considering the patient’s condition. If the prescription changed based on the formulary, then the patient was informed. Moreover, the pharmacist and nurse collaborated to monitor the patient for the effectiveness and safety of the prescribed medicines. When the patient consulted a local physician after discharge, all medication changes were noted in the discharge summary. Such a continuous approach was required in recovery and rehabilitation hospitals as well as in community-based integrated care hospitals.
Treatment according to the hospital formulary was proposed and approved for patients who could be introduced to the formulary-prescribed medications, mainly at the time of identification of medication history. The maximum dose of RAS in Japan, especially angiotensin-converting enzyme inhibitors, is lower than that approved in Europe and the United States. For example, in the case of enalapril, a dose of 10 mg per day is often prescribed. A 10 mg dose of enalapril, not 20 mg, 28 is prescribed instead of telmisartan 80 mg. ARBs and CCBs are often selected for the treatment of hypertension in Japan, and a fixed-dose combination of ACEIs and CCBs is not marketed. 41 In Japan, diuretics are not commonly prescribed as an antihypertensive medication in order to avoid the adverse drug reaction of dehydration and are not actively selected in our hospital because the median age of the patient population is 77 years and many older patients are admitted. 12 A reduction of the maximum RAS dose was proposed to conform to the indication of hypertension for preventing adverse drug reactions such as dry cough in hospitalized patients. This may explain why the RAS dosage decreased from an average of 10.7 mg of enalapril equivalent at the time of admission to 7.2 mg at the time of discharge. The same trend was found in a previous study, which showed that there was no change in blood pressure even when the proposed doses were converted for older patients. 12 We found the dosages of CCBs were appropriately proposed, as the dosage of alternative medicines for blood pressure control were not increased. With regard to XORis, febuxostat, a new medicine that was not frequently recommended by the formulary, was selected for a patient whose uric acid level could not be controlled with allopurinol 50 mg due to renal dysfunction. This was a case of targeted administration because of reduced renal function.
The cost of medications was reduced by 56.1 yen per patient per day, which translates to an annual cost reduction of 20 476.5 yen. As the medicines brought to the hospital are those used locally, it is likely that medication costs will decrease by introducing the formulary in local hospitals. Medication use optimization in Japan has not been adequately directed toward reducing medical costs. The recent increases in antibody-based medicines and total medical costs due to an aging Japanese population have imposed pressure on the medical care system, though the equal provision of a basic level of medical treatment to all patients in the nation still occurs and is an advantage of the system. 42 Therefore, the concept of appropriate use of medicines to reduce the costs borne by patients and the insurer should be widely disseminated, even if the medication cost may seem small at the individual medical practitioner level. Overall, in this study, the medication costs were decreased for all pharmacological classes. Though XORi costs showed a trend to decrease, we could not demonstrate statistical significance due to the use of the expensive medicine, febuxostat. The analysis showed that the total medicine cost of XORis did not increase but decreased, as allopurinol is recommended as the standard in the formulary. This indicates the formulary did not necessarily narrow the choice of medical treatment for physicians and patients, and the medicine cost was distributed appropriately regardless of pharmacological class.
There are two limitations to this study. First, few patients returned to our hospital after discharge, and it should be noted that we were not able to track all the formulary’s continuation patients. This study included patients who were introduced to the formulary in our hospital and attended our outpatient clinic (with different physicians and no restriction to prescribe from the hospital formulary). Though it was not possible to substantially track the discharged patients from our hospital who subsequently consulted at other hospitals or clinics, there were several cases where the patients did revisit our hospital and their medications had not changed, demonstrating that when hospital formularies are used, indicated medications and dosages of inpatients are often maintained by local outpatients. Therefore, a hospital formulary may help reduce medication costs in the community. Secondly, this study includes drug cost reduction partially based on the stability of the disease. The hospital formulary introduction rate was 80% in the previous study, 12 and the comparison between the formulary introduction and non-formulary introduction could not be verified because the distribution of cases was assumed to be unbalanced and the number of cases was less than the required number. We expect to collect sufficient data that integrates analyzable hospital data and regional data, and will aim to show the reduction of medication costs by switching the equivalent amount of medicines through a formulary system.
Conclusion
The development of hospital formularies influences outpatient prescribing, suggesting that collaboration among hospitals or in-hospital formularies may be an effective strategy to expand local formularies. As the number of newly approved medicines and medication costs are increasing worldwide, the introduction of formularies is just one of the necessary tools to provide appropriate pharmaceutical care to patients and facilitate better pharmacotherapy with minimized medical costs. Introducing a hospital formulary can contribute to the reduction of local healthcare costs in countries with universal healthcare coverage and in countries that plan to introduce local formularies.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580221087876 – Supplemental Material for Influence of Hospital Formularies on Outpatient Prescribing Practices: Analysis of the Introduction of a Local Formulary: A Single-Center, 2-Year Follow-Up, Retrospective Cohort Study of a Local Formulary in Japan
Supplemental Material, sj-pdf-1-inq-10.1177_00469580221087876 for Influence of Hospital Formularies on Outpatient Prescribing Practices: Analysis of the Introduction of a Local Formulary: A Single-Center, 2-Year Follow-Up, Retrospective Cohort Study of a Local Formulary in Japan by Norihito Kanai, PhD, Masazumi Ando, Momoko Shimodate, Yoshiko Miyazaki, PhD, and Toshio Saito in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgments
The authors would like to thank Mr. Itaru Jinbo for their editorial support, which included proofreading and formatting this manuscript. The authors would like to also thank Mr. Yoshito Suzuki, Mr. Takafumi Hashimoto, Ms. Kie Imai, Mr. Yasushi Otani, and Ms. Natsumi Kumada for their efforts in introducing and operating the formulary in the hospital.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
The study was approved by the Ethics Committee of the Niiza Hospital and was undertaken in compliance with the principles evinced in the Declaration of Helsinki. Patient informed consent was not required by the ethics committee.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.