
Abstract
Chinese clinical pharmacists consider improving the quantity and quality of consultations to be an important task in providing better pharmaceutical care. To achieve this goal, we developed a clinical pharmacist consultation method using multidisciplinary individualized medication recommendations (MIMRs) and studied the effects of its implementation. A retrospective study of 812 clinical pharmacist-led consultations was conducted. In the pre-intervention group, medication advice was given based on the purpose of the consultation. In the post-intervention group, a consultation method using MIMRs was implemented, in which clinical pharmacists with specialties in anticoagulation, gastroenterology, and nutrition were asked to give individualized medication recommendations. Outcomes, including the effectiveness rate of consultations (ERC) and acceptance rate of consultations (ARC), were compared between the two groups using propensity score matching method. Patterns and numbers of consultations and individualized medication recommendations were also compared. The results showed that the ERC in the post-intervention group compared with the ERC in the pre-intervention group was 83.3% vs 74.0%, respectively (P < .05). Significant difference was also shown between the two groups in ARC (98.4% vs 92.2%, P < .05). The total number of consultations increased, as did the number of general consultations, multidisciplinary/difficult consultations, anti-infection consultations, and non–anti-infection consultations specifically. As a result, we proposed that the implementation of MIMRs can improve the effects of treatment and increase the number of consultations by pharmacists, which is worthy of further promotion to better serve physicians and patients.
Keywords
• Chinese clinical pharmacists consider consultation to be vital in demonstrating their professionalism and participation in medical treatment. However, few studies have proposed a new method to improve the quantity and quality of their consultation work.
• This is the first innovative method to improve the quality and quantity of consultations by clinical pharmacists using propensity score matching analysis. After implementation, the effects of treatment improved, and the number of consultations by pharmacists increased.
• Clinical pharmacists who specialize in rational drug use should actively focus on all the medications of patients to provide comprehensive pharmaceutical care and improve their influence among physicians and patients.
Introduction
In China, pilot studies on the Chinese clinical pharmacist system began in 2008. Then, regulations of the Administration of Pharmaceutical Affairs in Medical Institutions, 1 promulgated and implemented in 2011, further promoted the transformation of the roles of pharmacists and refined their responsibilities in clinical settings. In that same year, a pharmacist-led management method was introduced into the Antimicrobial Stewardship Program, which strengthened the status of clinical pharmacists in the treatment of infectious diseases. According to guidance documents and preliminary practices, Chinese clinical pharmaceutical care mainly included making medical ward rounds, reviewing medical orders, reviewing prescriptions, answering drug-related questions, monitoring therapeutic drugs, and reporting adverse drug reactions. 2 Among these responsibilities, consultation played a vital role in demonstrating the professionalism of pharmacists and their participation, the importance of which is pointed out in the “Notice on Strengthening Pharmacy Administration and Changing the Pattern of Pharmaceutical Care” issued in July 2017. 3 As a result, clinical pharmacists took the improvement of the quantity and quality of consultations as an important task in defining their ability in clinical work.
To improve their clinical recognition and value, most clinical pharmacists in different specialties chose anti-infection treatment as their main point of entry into clinical medication management, and the effect was remarkable. This effect was clearly reflected in the purpose and acceptance rate of clinical pharmacists’ consultations (CPCs) 4-7: More than 80% of the consultations centered on the rational use of antibiotics. The acceptance rate of consultations was more than 90%, and the effectiveness rate of consultations was close to 90%. However, in terms of the responsibilities of clinical pharmacists, clinical pharmacists should perform consultations in a way that includes comprehensive pharmacotherapy analysis and gives opinions on complete pharmacotherapy instead of solely on antimicrobial therapy. Currently, most clinical pharmacists in China give only targeted recommendations for the purpose of consultation (the majority of clinical pharmacists’ consultations are intended for anti-infection purposes) and will not give comprehensive and individualized medication suggestions. The main reasons for the status quo are that Chinese clinical pharmacists lack expertise, which results in limited recognition by physicians.8,9 In addition, the training system of Chinese clinical pharmacists needs robust improvement, and the reform of the training system seriously lags behind.10,11
Therefore, we propose a method for Chinese clinical pharmacists to improve their consultations. In this method, we integrated multidisciplinary individualized medication recommendations (MIMRs) into anti-infection consultations to provide comprehensive pharmaceutical care. The multi-disciplines involved include anticoagulation, gastroenterology, and nutrition, which means the clinical pharmacists majored in these three areas are asked to give individualized recommendations in anti-infection consultations. Why were these three areas selected? To date, clinical pharmacists have engaged in inpatient and outpatient anticoagulation management and achieved better outcomes than usual or physician-managed care alone.12-14 In addition, the impacts of interventions by clinical pharmacists targeting the inappropriate use of proton pump inhibitors (PPIs) are impressive, and the intervention methods vary, including reviewing inpatient orders, obtaining prescriptive authority, and rational drug use education for physicians.15-17 Regarding nutrition areas, studies have shown that skilled nutrition pharmacists could be qualified for order review and verification and prompt rational use between enteral feeding and parenteral nutrition. 18 This study was unique in that we not only put forward a new way of giving consultation recommendations but also promoted the management of anticoagulation, PPIs, and nutrition by giving MIMRs in clinical pharmacists’ consultations, and hoped to improve the overall prognosis of patients.
In 2019, we started this MIMRs consultation method at a tertiary teaching hospital in Shanghai, China. This study aims to determine the impact of this new method on the effectiveness rate of consultations (ERC), the acceptance rate of consultations (ARC) and the number of consultations by propensity score matching analysis.
Methods
A retrospective study was performed at Tongji University Affiliated East Hospital, which is a tertiary teaching hospital with 2000 beds. This hospital specialized in tumor clinical trials and the treatment of cardiovascular disease. In this study, CPCs requested by clinical departments in 2017–2018 and 2019–2020 were enrolled in the pre-intervention and post-intervention group. All consultations performed by clinical pharmacists were eligible for inclusion. The exclusion criteria were as follows: incomplete consultation records, consultation cases about the authorization for use of special grade antibiotics, and consultations with patients who died within 72 h of the consultation or who stopped treatment for other reasons.
In the pre-intervention period, upon receiving a consultation request from a clinical department, a qualified clinical pharmacist evaluated the current situation of the patient and proposed recommendations according to the purpose of the consultation, which was the traditional pharmacists’ consultation method (TPCM). For instance, in TPCM, anti-infection clinical pharmacists give recommendations directly when a consultation requesting the dosage adjustment of antibiotics is applied, without other medication suggestions related to the current situation of the patient.
In the post-intervention period, the following interventions were implemented. After comprehensively evaluating the situation of the patient, clinical pharmacists with specialties in anticoagulation, gastroenterology, and nutrition were asked to give MIMRs. These clinical pharmacists are all qualified pharmacists who have been trained for one year in different subspecialties and passed the national certification examination. In addition to giving consultation recommendations, they are also involved in working in different wards and giving medication monitoring. In addition to an anti-infection treatment consultation, recommendations were made relating to the consultation purpose, anticoagulation treatment, use of PPIs, and provision of nutrition support. After the consultation, follow-up monitoring recommendations were given. A set of evaluation criteria for rational drug use were formulated according to the latest guidelines, recommendations of experts, and previous pharmaceutical practices. Finally, the effectiveness rate of consultations and acceptance rate of consultations were assessed.
Evaluation Criteria and the Consultation Method of MIMRs
Anti-infection treatment consultation recommendations
The current anti-infection treatment or prevention effect was evaluated based on the current infection status of the patient. The main consultation method was under the guidance of anti-infection pharmacists, and the consultation pharmacist on duty provided treatment recommendations, including the drug name, dosage, frequency and route of administration, and course of treatment. The precautions and adverse events to be monitored were also considered.
Anticoagulant Consultation Recommendations
Clinical pharmacists who specialized in anticoagulation performed venous thromboembolism (VTE) risk assessments for each consultation patient, especially inpatient patients with a high risk of VTE. When clinical pharmacists make VTE risk assessments, they mainly refer to 2012 guidelines for antithrombotic treatment and thrombosis prevention of American College of Chest Physicians (ACCP ninth Edition).19-21 According to the guidelines above, the Caprini score scale 22 and Padua score scale23,24 are used for surgical patients and nonsurgical patients, respectively. The risk for hemorrhage was evaluated for patients needing anticoagulation prevention treatment and the corresponding bleeding risk factors were recorded.25,26 The hemorrhage risk assessment criterion for patients with atrial fibrillation (AF) and patients taking oral anticoagulants was the HAS-BLED score. 27 The stroke risk for AF patients was evaluated by the CHA2DS2-VASc score. 27 According to the scoring criteria above, patients were given individualized scores and consultation recommendations. If the risk for embolism was significantly higher than the risk for hemorrhage, anticoagulant medication was given. If the risks were equal, physical prevention advice or consultation with the Department of Rehabilitation was provided. For the treatment of VTE, suggestions were proposed following the guidelines of 2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism 28 and 2016 Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. 29 For patients at risk for hemorrhage or consultations aimed at the use of anticoagulant drugs, suggestions were given by pharmacists with a specialty in anticoagulants (Supplementary Table 1).
PPI Use Recommendations
The evaluation criteria for the rational use of PPIs are divided into two main parts: assessing the necessity for preventive medication and rationally implementing therapeutic medication. The evaluation criteria pertain to stress ulcer prophylaxis in the postoperative period, 30 stress-related mucosal disease in critically ill patients, risk factors and strategies to prevent stress-related bleeding in the intensive care unit, 31 stress ulcer prophylaxis in hospitalized patients not in intensive care units, 32 expert recommendations for stress ulcer prophylaxis (2018) 33 and expert consensus on the optimal application of PPIs. 34 Stressors should be recorded. If preventive measures were needed, recommended PPIs and dosages were given. If the current utilization was inappropriate, suggestions for improvement were made. In terms of consultations for the purpose of PPI use, pharmacists with a specialty in gastroenterology gave suggestions (Supplementary Table 2).
Nutrition Support Recommendations
Nutritional risk assessment was performed for patients who were highly suspected of needing nutritional support. The assessment standard was the Nutritional Risk Screening 2002 (NRS 2002). According to the risk assessment scores of patients, current dietary status, relevant guidelines and recommendations,35-37 and corresponding enteral/parenteral nutritional suggestions were given. The key principle was that enteral nutrition supplementation was given priority for patients who were unable to eat on their own. 38 Supplementary parenteral nutrition was given only when enteral nutrition was absolutely contraindicated or could not meet the target requirements of the patient. The compounding standard for parenteral nutrition is as follows: the energy supply is 25–30 kcal/(kg/d); the protein is 1.2–2 g/(kg/d); and the ratio of sugar to lipids and nonprotein calories to nitrogen is 5:5 and (100–200):1, respectively. For consultations centering on the implementation of nutrition support, pharmacists with a specialty in nutrition gave the recommendations. If necessary, the nutrition department is invited to assist in the consultation (Supplementary Table 3).
Follow-Up Monitoring Recommendations
The follow-up monitoring recommendations mainly include the changes in the following indicators after the implementation of the consultation recommendations. The indicators were as follows: liver and kidney function indices (creatinine clearance and serum transaminase activity, etc.), infection indices (WBC, PCT, CRP, etc.), coagulation indices (APTT, INR,D-dimer, etc.), whether the symptom of bleeding occurred or nutrition improved. In addition, the adverse reactions that may be caused by drugs proposed in the consultation recommendations were also recorded as monitoring recommendations (Supplementary Table 4).
Outcome Measurements
The primary endpoint was the effectiveness rate of consultations (ERC), which was defined as follows: 72 h after consultation, two off-duty pharmacists evaluated the effectiveness of the consultation, which was defined as one or more relevant disease symptoms or signs that had significantly improved or that laboratory tests showed had decreased by more than 30%. The main reference standard was the outcome evaluation of the condition for which the consultation had been requested. If medication suggestions were given for the purpose of prevention, positive signs of the patients were examined.
ERC = Effective consultations/(Effective consultations + Ineffective consultations) ×100%.
The secondary outcomes included acceptance rate of consultations (ARC) and the consultation numbers of post-intervention group, as compared to pre-intervention group. ARC was calculated according to the following method: (1) Not accepted: The physician rejected the consultation suggestions. (2) Partially accepted: the physician partially accepted the consultation suggestions. (3) Completely accepted: the physician completely accepted the consultation suggestions. Accepted consultations=completely accepted consultations+ partially accepted consultations.
ARC = Accepted consultations/Total consultations ×100%.
Data collection and statistical analysis
The data were recorded from the Electronic Medical Record System and collected manually, which were cross-checked by two independent pharmacists. Patient characteristics, including gender, age, liver function, kidney function, infection indices, underlying diseases, embolism risks, bleeding risks, gastrointestinal risk, and nutritional status, were documented by review of the medical chart.
IBM SPSS 25.0 software was used to perform statistical analyses. We employed the propensity score matching (PSM) approach to control the confounding bias between groups. Then logistic regression was used to estimate the propensity score value, which included gender, age, liver function, kidney function, infection indices, underlying diseases, embolism risks, bleeding risks, gastrointestinal risk, and nutritional status as variables related to the outcome. The matching method was 1:1 nearest neighbor matching. Standardized differences before and after PSM were calculated. The matching stopped once the variable fell between .0±.001, which means the variable reached an equilibrium. Continuous variables were presented as medians along with standard deviation and were tested by grouped t-test and Wilcoxon rank-sum test. The number of cases (percent) described categorically and the Chi-Square test or Wilcoxon rank-sum test was performed. P<.05 was considered statistically significant.
Results
A total of 934 consultation cases were selected for the study, of which 812 cases met the inclusion criteria. Among the 812 consultation cases, 364 cases were in the pre-intervention group, and 448 cases were in the post-intervention group. Figure 1 describes the procedure of case selection. Flow chart of the study.
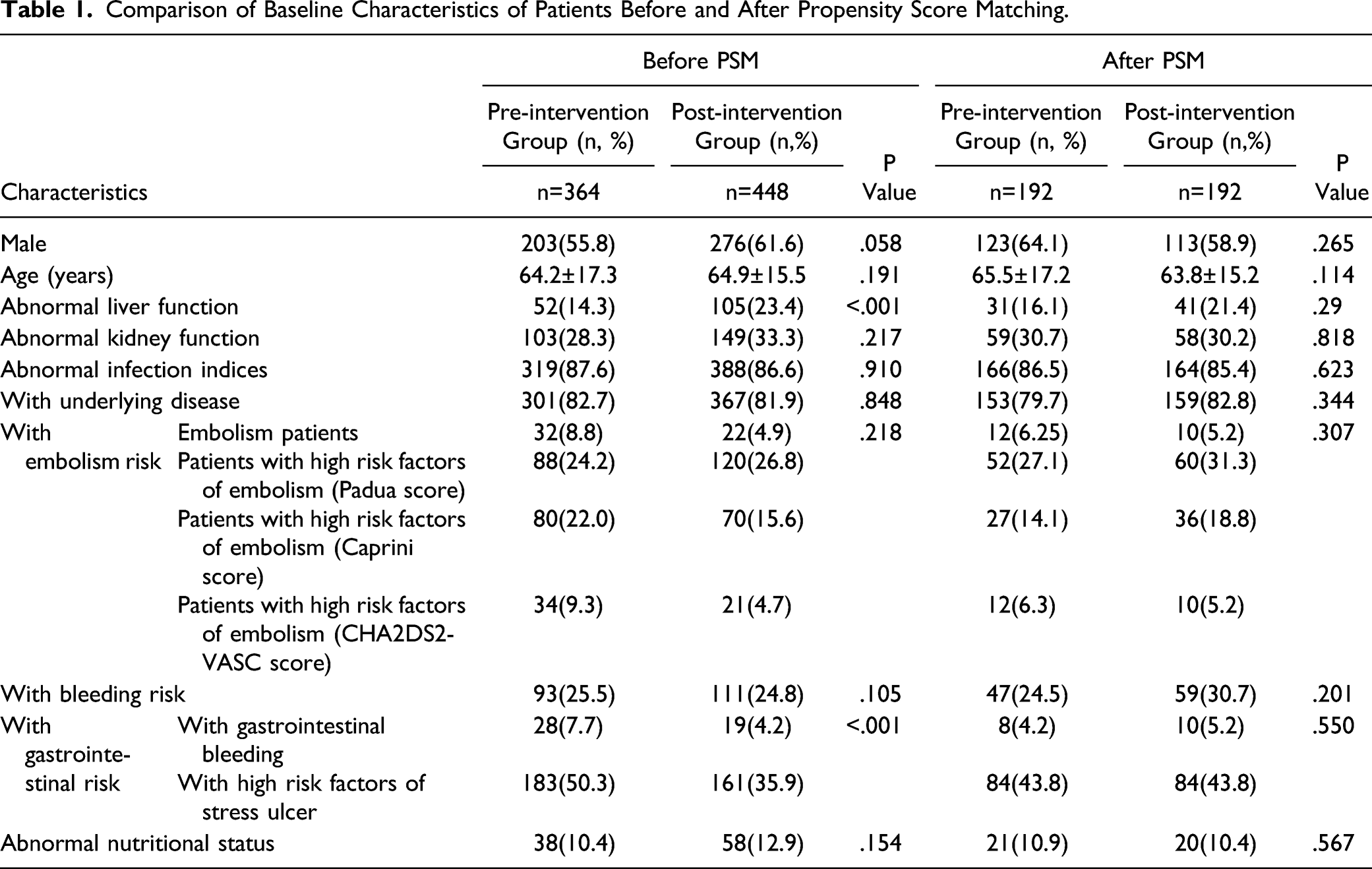
Comparison of Baseline Characteristics of Patients Before and After Propensity Score Matching.
Detailed information on the 812 consultation cases is shown in Figure 2. The number of general consultations (369 cases vs 345 cases), multidisciplinary/difficult consultations (79 cases vs 19 cases), anti-infection consultations (397 cases vs 322 cases) and non-anti-infection consultations (51 cases vs 42 cases) in the post-intervention group increased, as compared to the pre-intervention group. Clinical pharmacists’ consultation types and application departments.
Among non-anti-infection consultation cases, consultations on individualized medication regimens and adverse reactions accounted for the highest proportions, both of which were 27% (25 cases). A total of 15% (14 cases) were for anticoagulation consultations, while 17% (16 cases) were for nutritional consultations, as shown in Figure 3. The top three clinical departments requesting CPCs were the Department of Spinal Surgery (129 cases), the Department of Urology (113 cases), and the Central Intensive Care Unit (CICUs) (75 cases), as demonstrated in Figure 4. Purposes of non–anti-infection consultations. Distribution of included consultation cases requested by clinical departments (Top 20).

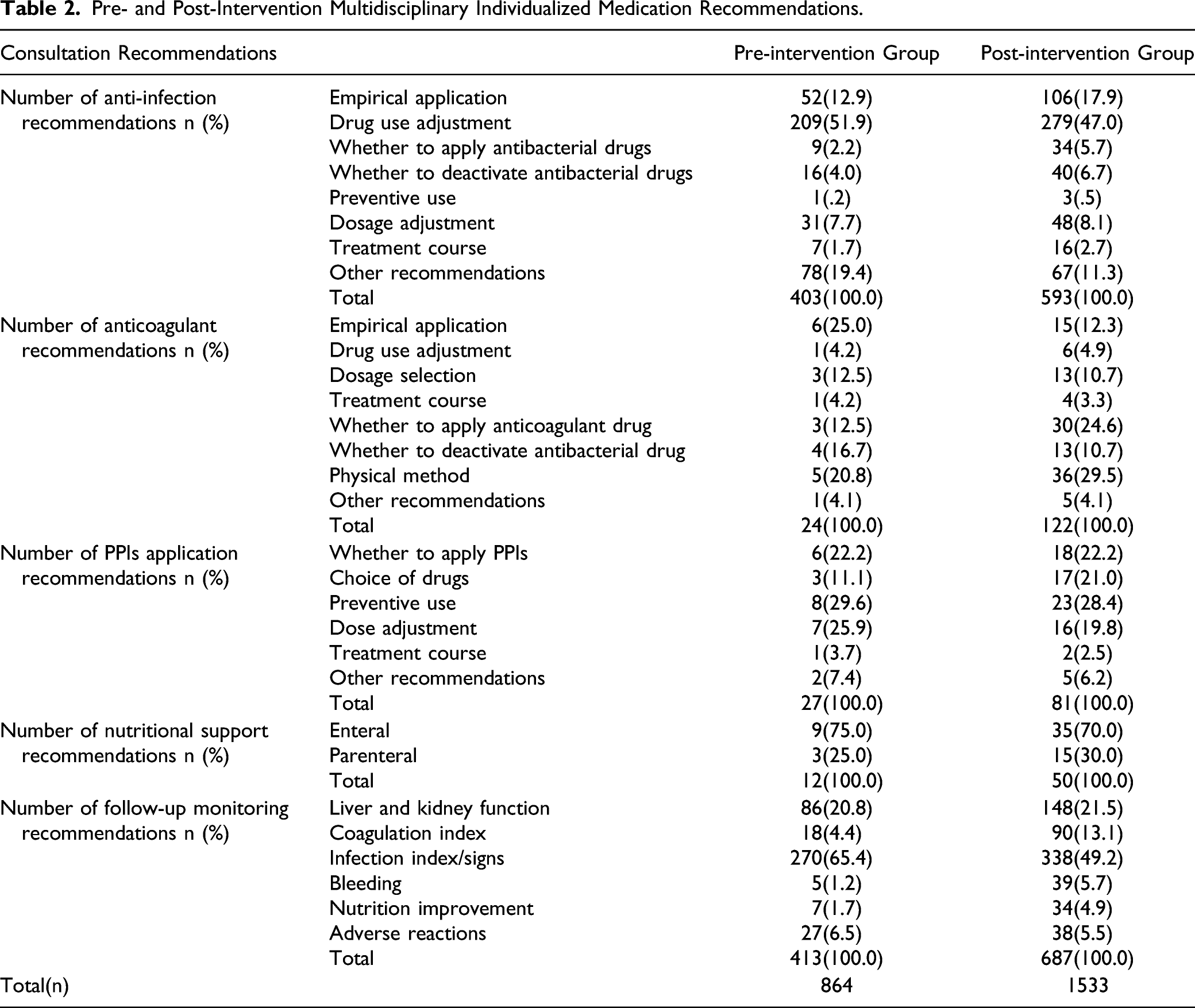
Pre- and Post-Intervention Multidisciplinary Individualized Medication Recommendations.
Effectiveness Rate and Acceptance Rate of the Consultations.

Discussion
In the Department of Spinal Surgery and Department of Urology, the characteristics of the patients were distinct. The patients tended to be elderly individuals, individuals with liver and kidney dysfunction, and individuals with multiple chronic diseases; thus, there was a greater need to adjust medication dosage and identify drug interactions. In addition, the number of patients with fever after surgery was large, and surgeons lacked experience using antibiotics. Consultations in intensive care units (ICUs) mainly included multidisciplinary/difficult cases. The main concern was the individualized medication requirements of patients with multidrug-resistant bacteria or rare pathogenic bacterial infections. To provide better pharmacy services for ICU patients, senior clinical pharmacists regularly held case discussions and literature reports in ICUs. This approach was what we took to meet the needs of physicians. According to some Chinese reports on the evaluation of pharmaceutical services by physicians,8,39 their demand for pharmaceutical services of clinical pharmacists focused mainly on the provision of drug information. From a global perspective, Clare Be´chet et al 40 found that pharmaceutical activities (e.g., teaching and supervision) are valued and sought by physicians. Gillespie U et al 41 reported that physicians thought that their own knowledge of drug therapy had improved because of the training and teaching by clinical pharmacists. Considering the situation above, we provided a learning and communication platform for physicians. The topics we shared included mainly high-quality anti-infection literature, the rational use of special grade antibiotics such as ceftazidime, avermectin, and polymyxin B, and individualized medication experience analyses, which were what physicians care about in our hospital.
The purpose of developing the method of MIMRs in our hospital was to create a multidisciplinary pharmacist consultation service. According to the data shown in Figure 3, the total number of non-anti-infection consultations in the pre- and post-intervention group accounts for 11.5% of the total consultation cases, which is equivalent to the average proportion of tertiary hospitals in other regions of China. 7 There is still a certain gap between the breadth of drug selection and the difficulty of consultations compared to national clinical pharmacy specialty hospitals. 42
The anticoagulant pharmacy services our hospital has carried out are embodied in pharmacy rounds and the support of physician–pharmacist joint anticoagulation outpatient clinics. The addition of anticoagulant recommendations to pharmacists’ consultations is another attempt at pharmaceutical intervention. First, during the intervention process, we found that for elderly patients with renal insufficiency, physicians are often confused about the choice of medication and dosage. Second, for nonsurgical patients, physicians tended to ignore whether they were at high risk of embolism, which led to inaccurate timing in the use of anticoagulant drugs. In addition, during the process of medication delivery, the risk for hemorrhage was easy to overlook, resulting in an increased risk of adverse consequences. Finally, balancing the risk for embolism and the risk for hemorrhage and carrying out physical prevention measures were also weak links. In response to all these difficulties, clinical pharmacists gave intervention measures in CPCs. After intervention, no consultation patients experienced embolism or hemorrhage due to unreasonable use of anticoagulants. At present, the participation of clinical pharmacists in anticoagulation work in China is still in the initial stages. The work focuses mainly on patient follow-ups and assisting doctors in patient education and management. In addition, current anticoagulant management norms and standardized anticoagulation evaluation systems are also in the exploratory stage. 43 However, some clinical pharmacists from global medical centers have launched pharmacist-led anticoagulation management with good outcomes and practical rules formulated. Pelletier R 44 developed a novel pharmacist-led venous thromboembolism (VTE) risk assessment program for the assessment of the risk of VTE in ambulatory patients with cancer. Alghadeeer S et al 45 found that patients followed in a pharmacist-led clinic had higher TTR levels than those followed in a physician-led clinic. We need to find our own way out to catch up with other countries.
PPIs are widely used in clinical practice. In the previous pre-prescription review and key drug-monitoring review, we found that physicians often used PPIs irrationally. Such uses included inappropriate timing of medication, unreasonable choice of dosage and dosage form, inappropriate use of the drugs, etc. After the implementation of the intervention, the recommendations we gave included mainly therapeutic and preventive dosages, the choice between oral and intravenous drip dosages and delivery forms, and the incidence of adverse reactions caused by drug interactions, all of which were generally welcomed and accepted by physicians. PPI abuse has grown over time not only in China but also in many other countries.46-49 As a result, a series of targeted measures by pharmacists has been implemented, and preliminary improvements have been achieved worldwide.50-53 The addition of PPI recommendations in CPCs is our attempt to contribute to this effort. With the continuous promotion of this method, we hope to further rationalize PPI use and reduce unnecessary drug expenditures.
In China, the work content of nutrition pharmacists overlaps with the work content of the Department of Nutrition, resulting in relatively slow progress. Nutritional pharmaceutical care in our hospital is still in its infancy, and the care does not match the needs brought about by the specialization of the hospital in tumors. In fact, in the face of the needs of the large number of tumor patients and the rapid development of new varieties of nutritional drugs on the market, oncologists need the support of nutrition pharmacists. At present, although the total number of nutrition consultations is small, we have basically instituted individualized nutritional score screening for each patient, which is related to the low prevalence of malnutrition. 54 Thus, we have taken the first step of nutritional screening at the pharmaceutical level. However, it is far from enough to give recommendations on enteral or parenteral nutrition based on screening scores. Guenter P et al 55 pointed out that errors may occur at every step of using parenteral nutrition; however, available help from outside is limited. Therefore, pharmacists should do something more. The next step is to sort out the classification of enteral and parenteral preparations in our hospital and to introduce energy density, sugar–fat ratio, preparation characteristics and pharmacoeconomic evaluations to physicians to let them know our expertise in nutrition support.
The ERC in the post-intervention group was significantly higher than the ERC in the pre-intervention group (83.3% vs 74.0%, P < .05) but lower than the ERC reported in the domestic literature. It was possibly attributed to our hospital being the leading phase I tumor clinical research center in China, which attracts a large number of patients with advanced malignant tumors. Consultation patients often have serious infections and multiple organ failure, which leads to poor prognoses and affects the ERC. The ARC of the post-intervention group was also significantly higher than that of the pre-intervention group (98.4% vs 92.2%, P < .05). Moreover, it was higher than what was reported in the domestic literature,8-10 probably due to frequent interactions with physicians and their general recognition of clinical pharmacists’ abilities.
Limitations
The limitations of this study are as follows: 1. ERC was not the most desirable outcome of interest in this study. In terms of this primary endpoint, we would have addressed ERC as the minimal response rate (MRR). However, when searching for relevant literature, we found that in the studies of Zhang JX et al5,56 on the effectiveness of clinical pharmacists’ consultations, the primary endpoint was effective response (complete or partial response). The endpoint was defined as partial or complete resolution of clinically significant signs/symptom improvement or resolution of computed tomography (CT) or magnetic resonance imaging (MRI) findings and on proven or negative culture results. The effective response rate (ERR) was the proportion of patients achieving an effective response to the total number of patients. In domestic evaluations of consultation studies of clinical pharmacists,57,58 the primary endpoint of patient prognosis was also evaluated by the effectiveness rate, which was defined as one or more of the symptoms, signs, and relevant laboratory examination indices of the patient significantly improving. As a result, we named ERC as the primary endpoint. In the future, more patient-centered outcomes (quality of life and survival) should be included instead of ERC alone. In the next step, we plan to perform a prospective study on the evaluation of this MIMRs method, and a standardized questionnaire to evaluate the quality of life of patients will be developed. 2. This study was a single-center study, with most of the patients being from the Pudong New Area of Shanghai, China. To further evaluate the impact of the new consultation method on patient outcomes, multicenter and large sample studies should be carried out.
Conclusions
This study is the first innovative method of CPCs to improve the quality and quantity of consultations by pharmacists in a clinical inpatient setting. After the implementation of this method, anticoagulation regimens, PPI use, nutrition therapy, and individualized follow-up monitoring recommendations were added to the consultation recommendations, which increased the number of consultations. Of note, ERC and ARC in the post-intervention group were significantly higher than those in the pre-intervention period and ARC continued to be higher than the average level in China. It reflected the value of clinical pharmacists in contributing to rational drug use and showed the advantage of using MIMRs to improve patient outcomes. We confirmed that CPCs using MIMRs will provide better support for physicians and patients and should be considered worthy of multicenter promotion.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580221081437 – Supplemental Material for Integrating Multidisciplinary Individualized Medication Recommendations Into the Traditional Pharmacists’ Consultation Method: A Retrospective Study Using Propensity Score Matching Analysis
Supplement Material, sj-pdf-1-inq-10.1177_00469580221081437 for Integrating Multidisciplinary Individualized Medication Recommendations Into the Traditional Pharmacists’ Consultation Method: A Retrospective Study Using Propensity Score Matching Analysis by Xiucong Fan, Danxia Chen, Siwei Bao, Rong Bai, Fang Fang, Xiaohui Dong, Yuyi Zhang, Xiaogang Zhang, Yabin Ma and Xiaobo Zhai in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgments
The authors wish to thank the staff of the Pharmacy Department and all the physicians and patients for supporting the study.
Author Contributions
XBZ and YBM conceived and designed this study. XCF wrote the manuscript. DXC participated in the modification of the manuscript. SWB, RB, and FF managed the data collection. XHD analyzed the data. YYZ and XGZ contributed to revisions to the manuscript. All authors reviewed and approved the final version.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Key Specialties Foundation of Clinical Pharmacy of Shanghai Municipal Health Commission in China, Grant/Award Number: SWLCYXZX-2018-001; Research on the Epidemiology of Severe Drug-induced Diseases of the Chinese Society of Toxicology, Grant/Award Number: CST2019CT304.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.