
Abstract
This study evaluated the essential stroke care structure available in the two Tertiary Health Facilities in Rives State, Nigeria. This was a descriptive survey involving the Stroke Care Survey and Assessment Tool (checklist/questionnaire) developed by the World Stroke Organisation to obtain information about the available essential stroke care structure (facilities, equipment, personnel and management protocol) at the two tertiary health facilities (RSUTH & UPTH). The study gathered relevant information, which was summarised into tables and graphs using Microsoft Excel 2016. From the results, although facilities had A and E departments, dedicated stroke units (fixed or mobile) were unavailable, and there was no locally developed protocol to support rapid triage of stroke patients. The facilities and equipment were either unavailable or insufficient. Only one health facility (RSUTH) provided 24 hrs/7 days laboratory services. The workforces were a mix between regular clinical staff and some specialists. Tissue plasminogen activator (tPA) use was non-existent, though specialists were trained on its administration. There was no locally developed or adopted stroke-specific clinical guidelines. In conclusion, the structural services available for stroke care within the studied tertiary health facilities were poor, unavailable or grossly insufficient. The state facility (RSUTH) suffered the most in terms of unavailable national support and staff development.
An effective stroke care service requires a well-organised stroke unit (SU), which is an organised in-hospital facility that is entirely (or next to entirely) devoted to caring for patients with all types of strokes. Ideally, every tertiary hospital that manages stroke should have key components of a comprehensive stroke centre (CSC) as recommended by the brain attack coalition (BAC) and World Stroke Organisation (WSO).
It highlights the current state and preparedness of the health system in Nigeria with focus on stroke care in one of the cosmopolitan cities; Port Harcourt, Rivers State.
The research found that stroke care is grossly neglected. The health facilities lack a resilient health care system that incorporates national and state-level training programmes for managers of stroke, as the current health care system may eventually be overwhelmed by the rising cases. Also, it discovered that the hospitals lack community engagement plans and communication strategies to reduce hospital admissions, morbidity and mortality associated with stroke. There are no stroke management policies within the health system.
Introduction
The ultimate goal of public health is to improve the health and standard of living through the administration of various public health strategies and programmes 1 ; however, man is not without series of health challenges, one of such is ‘neuropathy'. Neurological diseases, which are nervous system disorders or diseases, form a significant portion of chronic and degenerative conditions with severe epidemiological impact.2,3 In 2005, Neurological disorders contributed to 10.9%, 6.7%, 8.7% and 4.5% of the global burden of disease in high, upper-middle, lower-middle and low-income countries, respectively. 4 The condition is not associated with any geographical location, however, its impact varies with developmental strides. For example out of the hundreds of millions of global populations affected by neurological disorders, over 6 million people die from stroke each year, and over 80% of the deaths occur in low and middle-income countries. 5 The report indicates a close association between development and certain neuropathies.6–10 There is evidence suggesting that neurological services and resources are disproportionately scarce, especially in low income and developing countries.11–13 There is also the factor of under-preparedness of the government and policy-makers to tackle the rising prevalence and associated disability and mortality resulting from the continued tolerance of the situation.14–16
The provision of quality healthcare services is a fundamental right of the citizen 17 and the responsibility of the government, especially in critical times.18–20 The clinical services available to stroke patients in Sub-Saharan Africa are grossly inadequate, 21 of which the Nigerian experience is not an exception.22,23 Compounding the shortfalls is the inadequate neurodiagnostic facilities and clinical specialists in most healthcare facilities across the country, 24 the few well-trained neurovascular clinicians often prefer to practice in developed countries than stay back to tolerate the inadequacies.25,26 Nigeria showed commitment to achieving better healthcare for the neuro-diseases populace,27,28 however, the progress and sustainability seems slow, which may be associated with the socio-economic-political dynamics of the country and its administrative agencies and bodies.20,29
In a standard health care setting, stroke care system includes three distinct types of facilities: acute stroke-ready hospital (ASRH); primary stroke centre (PSC) and comprehensive stroke centre.30–34 ASRHs are small facilities often located in isolated suburban or rural areas. 35 ASRHs are typically able to stabilize the condition of stroke patients, offer specific acute stroke procedures and arrange for patients to be transferred to the closest PSC or CSC hospital as determined by the patient’s health status and additional treatment indications.36,37 PSCs can treat majority of stroke patients with typical ischaemic strokes that do not need endovascular treatment, neurosurgery, or intensive care. 37
The 2 tertiary facilities in Rivers State; Rivers State University Teaching Hospital (RSUTH) 38 and University of Port Harcourt Teaching Hospitals (UPTH), 39 which are State and Federal-owned healthcare facilities, respectively, can be classified as academic medical centres that teach and train future medical professionals, conduct state-of-the-art research, care for the poor and uninsured and provide highly specialized clinical care to the most severely ill and injured patients. 40 A classical CSC has several characteristics of a tertiary health facility in most developed countries. The teaching hospitals in Rivers State, though mostly unstructured are designed to have a comprehensive stroke centre (CSC).
The comprehensive stroke centre (CSC) handles the most complex types of stroke cases – large ischaemic strokes, all types of haemorrhagic strokes, or multisystem involvement, as well as those who require surgical or endovascular interventions and ICU-level care.33,37 A major characteristic of the CSC is the ability to provide 24-hours specialized interventions such as availability of a stroke unit,41,42 neurological ICU staffed with intensivists,32,33,43,44 the ability to perform advanced neuroimaging techniques,37,43 the use of endovascular techniques to treat ischaemic and haemorrhagic strokes33,36,43; the ability to perform neurosurgical treatments such as carotid endarterectomy, carotid stenting, and hemicraniectomy 37 ; and a structured stroke management protocol or guideline. 37
The structural services of stroke care cover the physical and operational aspects within a health care setting, including the availability of a stroke unit, an accident and emergency department, a multidisciplinary team, stroke technicians, neuroimaging, stroke treatment and health care policy.32,33,43,44 Ideally, tertiary hospitals should have key components of a comprehensive stroke centre (CSC) as recommended by the brain attack coalition (BAC).
33
These key components include all seven-stroke care structure,
35
in terms of personnel with specific areas of expertise, specialized diagnostic and treatment techniques, facility infrastructure as well as other programmatic areas (Figure 1).
33
Structural dimensions of stroke care.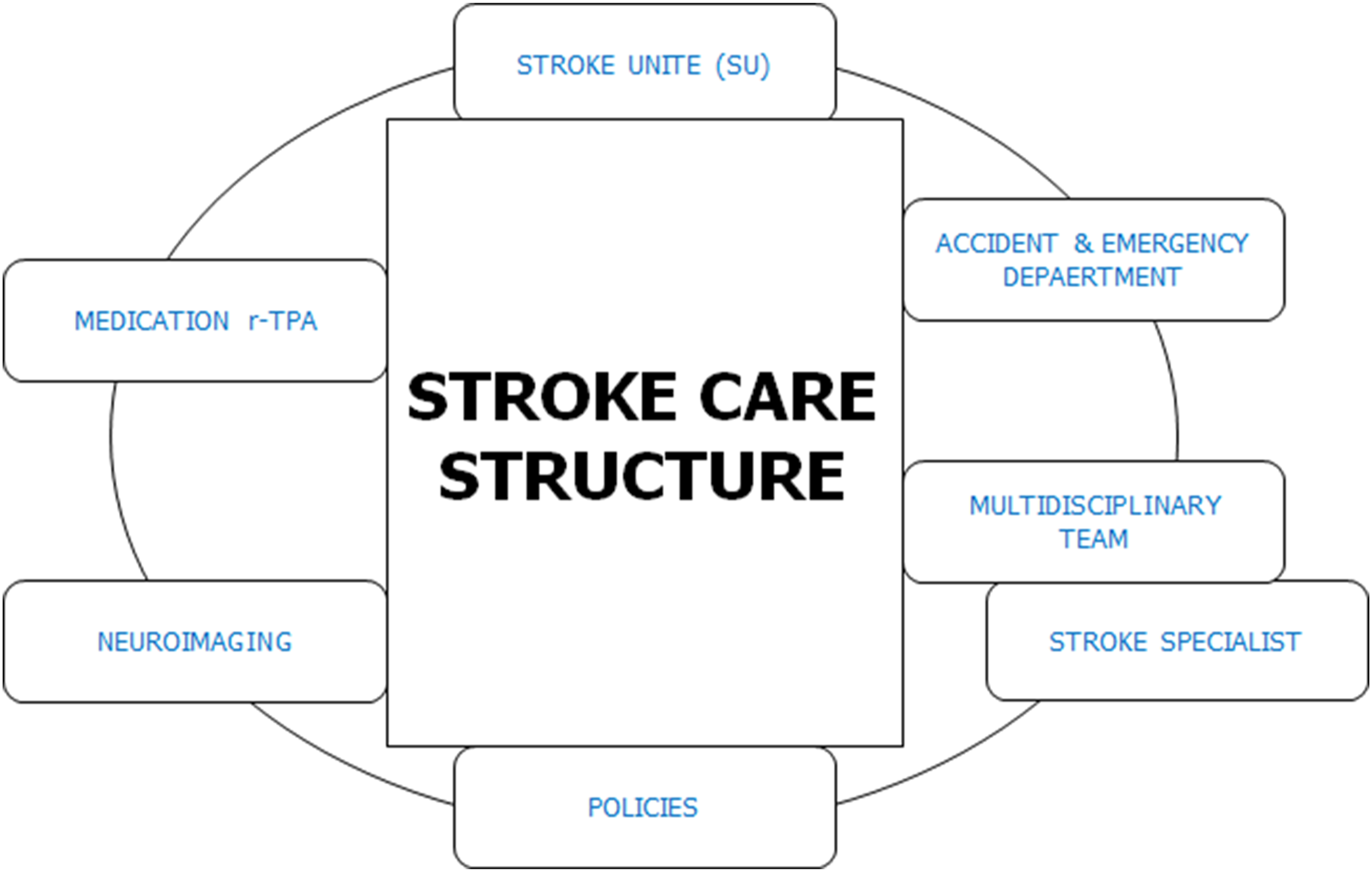
Without understanding the state of the healthcare facilities available for managing stroke, it would be difficult to access the preparedness for such highly prevalent disease. Based on this background, this study evaluated the structural capacity for stroke care in the 2 tertiary health facilities in Rivers State, Nigeria. This is done to provide insight into the current service available to stroke patient, as the findings are essential for re-strategizing, and improving health care for stroke patients.
Methods
Study Design
The study adopted a descriptive research design involving a survey conducted at the tertiary health facilities in Rivers State, with the aim of obtaining data on the current available structural stroke care services. In this research, structure is defined as the relatively stable characteristics of the health care providers, the tools and resources that are at their disposal, and the physical and organizational settings in which they work. The research was conducted from 10th November 2020 to 28th February 2021. The study followed the guidelines of Helsinki for the conduct of research. 45
Instrumentation and Data Collection
The study instrument used was a well-designed and structured Stroke Care Survey and Assessment Tool, developed by the World Stroke Organisation. 46 The checklist/questionnaire was expected to provide information about the structure of the facilities and highlight the current services in terms of qualified health personnel and equipment (such as diagnostic and operating tools).
The instrument has been shown to be validly and reliably utilised in affiliated nations to the World Stroke Organisation. 46 However, to ensure that the instrument (tools, processes and data) is ‘appropriate’ for our environment, three (3) validity tests were considered; construct, content validity and face validity. In ensuring that the three measures were achieved, expert opinion was obtained from various public health professionals who specialize in health systems.
A checklist was used to assess the availability of essential stroke care services, which includes: facilities, equipment, medication, stroke team and qualification, stroke services, and information management and communication systems. The study obtained information from observation and discussion with authorised unit personnel conversant with the operational methods.
Data Management and Analysis
The obtained data was managed and analysed in Microsoft Excel 2016. Tables and graphs were used to describe the results.
Results
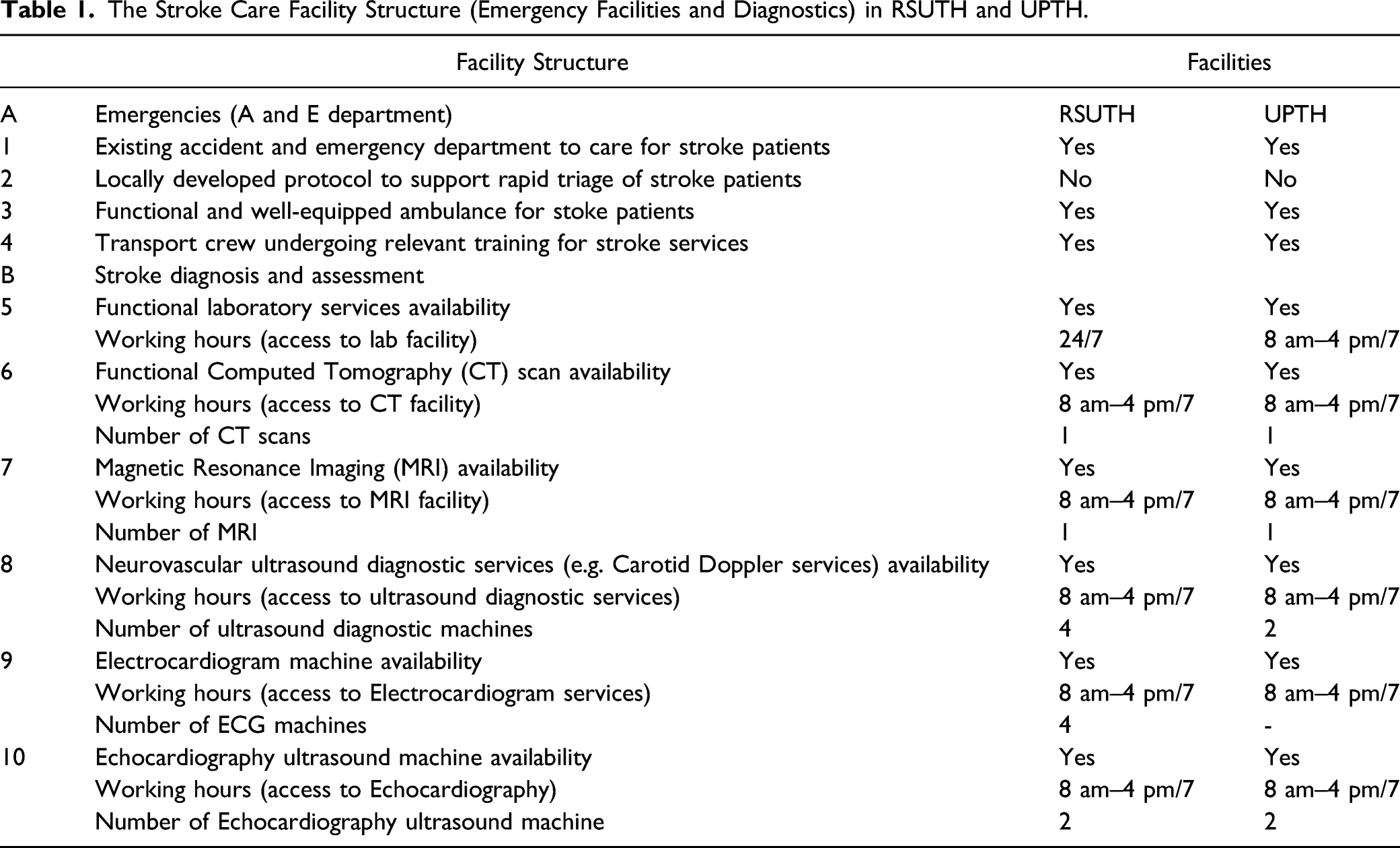
The Stroke Care Facility Structure (Emergency Facilities and Diagnostics) in RSUTH and UPTH.

The stroke care facility structure (human resource and workforce) in RSUTH and UPTH.
The Stroke Care Facility Structure (Interventions and Services and Health Policy Support) in RSUTH and UPTH.

The emergency stroke facilities and diagnostics available in the two studied health facilities is presented in Table 1, and the results found that for stroke emergencies, there are no locally developed protocol to support rapid triage of stroke patients. However, both facilities have existing accident and emergency department to care for stroke patients, functional and well-equipped ambulance for stoke patients and stroke services training (such as, FAST recognition) for transport crew.
The result for the stroke diagnostic and assessment facilities in Table 1 indicates that only one health facility (RSUTH) provides a 24 hrs/7 days laboratory services, while other services essential for stroke care such as Computed Tomography (CT) scan, Magnetic Resonance Imaging (MRI), Neurovascular ultrasound diagnostic services (e.g. Carotid doppler services), Electrocardiogram, Echocardiography ultrasounds were only available during normal work hours (8 am–4 pm) daily. However, the quantity per diagnostic equipment per facility varied as RSUTH had more neurovascular ultrasound diagnostic (4) and ECG machine (4) compared to UPTH (neurovascular ultrasound diagnostic; 1 and ECG; 0).
The facilities’ human resources and workforces as described in Figure 2 indicate that RSUTH have less manpower and healthcare workers compared to UPTH. For example, the number of neurosurgeons, neurologist, intensivist, clinical psychologist and speech psychologist in RSUTH are 1, 0, 0, 0 and 0, respectively, compared to UPTH that have 3 neurosurgeons, 2 neurologists, 29 intensivists, 4 clinical psychologists and 1 speech psychologist. Both facilities did not have occupational therapists.
The investigation of the availability of interventions and services available for stroke care in Table 2 indicated that the tertiary health facilities did not have specialized stroke unit for patients. However, they had specialised wards and monitoring unit, multidisciplinary team for stroke care. The facility stroke team had knowledge and application of tissue plasminogen activator (tPA) for acute ischaemic stroke care. However, tPA was not available for use in the facility. RSUTH reported that the major reason for the non-usage of tPA was the late presentation of patients, while UPTH reported the cost as well as late presentation of patients. Both facilities used aspirin for managing ischaemic stroke.
The inquiry into availability of health policy support for stroke management and staff development indicated that there was no stroke-specific clinical guideline for the hospital, but inquiry into the exact adopted guideline showed that both facilities did not have any. Neither RSUTH nor UPTH utilises any of the National stroke scale. Both facilities had an early discharge plan for patients, but RSUTH did not have any other stroke support policies such as professional staff development and quality improvement, local and national support for stroke care, stroke register/database in facility, community awareness program and stroke rehabilitative programmes. However, for UPTH, there was professional staff development and quality improvement policy, local and national support for stroke care, no stroke register/database in facility; but there was community awareness and rehabilitative programmes for stroke (Table 2).
Discussion
The Stroke Care Facility Structure
This study involved the survey of the 2 tertiary (teaching) hospitals; RSUTH and UPTH in Rivers State for their structural position in the management of stroke patients within their reach. Based on the recommendation of WSO, the seven areas were evaluated;
Emergencies
Because stroke is usually an emergency, the availability of emergency stroke care facilities forms an integral aspect of stroke management. In this study, we observed that the emergency stroke facilities and diagnostics available in the 2 studied health facilities were grossly inadequate as no facility had the Stroke Emergency Mobile (STEMO) ambulances. Although the facilities had existing accident and emergency department to care for stroke patients, but, the ambulance available for stroke patients were not well-equipped and stroke services training (such as, FAST recognition) for the transport crew (which were not registered paramedics professionals) were basic. The role of mobile stroke units and well-trained paramedics to handle stroke cases have been emphasised in several studies.47–54 In several studies, mobile stroke unit with trained personnel, and not regular ambulance significantly reduces the disability at 3 months for patients with acute ischaemic stroke.48,50,51,53,54 A mobile stroke unit is always well-equipped to manage a stroke patient and reduce the extent of neurological damage delays may cause. According to Wendt et al., 54 the triage of patients with cerebrovascular events to specialized hospitals can be improved by Stroke Emergency Mobile (STEMO) ambulances.
Stroke Diagnosis and Assessment
In this study, only the laboratory services of RSUTH operates on a 24 hrs/7 days basis, while other services essential for stroke care such as CT scan, MRI, Neurovascular ultrasound diagnostic services, electrocardiogram, echocardiography ultrasounds were only available during normal work hours (8 am to 4 pm) daily. The guideline for the organisation of stroke care facility at the CSC level require that facilities have artificial ventilators, echocardiography and carotid Doppler facility, neurosurgery units, MRI or angiography and rehabilitation facilities44,55; with a 24-hour operation. 56 In the current study, the quantity per diagnostic equipment per facility varied as RSUTH had more neurovascular ultrasound diagnostic (4) and ECG machine (4) compared to UPTH (neurovascular ultrasound diagnostic; 1 and ECG; 0). It will be very difficult to determine if the equipment in the tertiary facilities is sufficient to carter for the stroke population (crude prevalence of 8.51/1000 as at 2014) 57 in the South-South region.
Medical Team
The study observed that the quoted staff strength was the total number of available staff in the health facilities; thus, the dedicated stroke team would be a small group of staff. The study could not access the experience of the clinical and medical staff of the 2 health facilities. The group of medical professionals working as a unit is often referred to as a stroke Multi-Disciplinary Team which is often comprised of physiotherapists, occupational therapists, speech and language therapists, stroke physicians, nurses and other health workers with neurological training and periphery team members – dieticians, clinical psychologists and social workers with experience and training in stroke care.56,58,59 Studies emphasise the need for stroke specialists and professionals (stroke teams, competence, skill, awareness, confidence and experience in dealing with clinical situations) to ensure quality stroke care.60–63 According to Prasad et al., 56 the stroke team should be available 24 × 7 and a member of the team should be at patient bedside within 15 minutes of being called. In reality, with staff strength of both RSUTH, achieving Prasad et al.‘s suggestion is far beyond realistic.
Stroke Interventions and Services
Oral aspirin and intravenous tissue plasminogen activator (tPA) are the most utilised therapeutic intervention for stroke management.33,43,64–70 However, studies recommend an initial assessment of the stroke patients for fitness.67,71–73 In this study, only aspirin is considered for use in both health facilities. The use of tPA was non-existent, though they train their clinicians on its administration. The major reason why both hospitals did not consider the use of tPA were the cost of the drug and patients timing. These reasons are very valid as the market value of tPA is between $2200 and $2500.68,74,75 Empirical evidence also suggest that a stroke patient must be assessed and must qualify before tPA can be administered67,71-73,76; thus, when stroke patients report late to health facilities, the likelihood that the patient will qualify to be administered tPA is quite slim. On the other hand, treatment of haemorrhagic stroke normally requires surgery/clipping in most cases,33,77 and on some occasions the use of recombinant factor VII (rfvIIa).78-82 However, with few neurosurgeons present in both health facilities and the unavailability of rfvIIa, the possibility of timely intervention in haemorrhagic stroke is often not feasible.
Stroke Management Health Policy
A well-organised stroke management centre is expected to have a structured stroke management protocol or guideline that addresses stroke triage, inter-hospital transfer, intravenous thrombolysis protocol, intracerebral haemorrhage protocol, decompressive craniectomy protocol, acute stroke care protocol and TIA triage protocol.32,37,54,60 In this study, neither hospital had a stroke-specific clinical guideline neither did they adopt any guideline. The situation is worrisome because if there is a new neurologist, one wonders how he would fit into the system or handle case-specific emergencies. Studies found that compliance to stroke guidelines improves stroke outcomes.84-88
Power et al. recommends that facilities providing stroke care develop policies and guidelines for the facilities to ensure proper medical care is provided to patients. 72 Micieli et al. 87 in their study of guideline compliance and stroke outcome found that survival and treatment effectiveness were directly correlated with guideline compliance. It was surprising that RSUTH did not have any local or national support for stroke management, any stroke register and database, no community intervention programme for stroke. The study recognises the resilience of the stroke medical personnel that despite the poor support for programme development from the institution, they are still committed to the discharge of their responsibilities. Studies suggest that stroke intervention programme targeted at risk factors have evidently reduced stroke-associated mortality over the years.84,86,89,90 Therapeutic intervention to reduce blood pressure as assessed in clinical settings and widespread public health interventions in the general population appears to be the major determinant for reduction in the risk of stroke and stroke deaths.72,84-94
Conclusion
The structural services (emergency response, stroke diagnosis and assessment, specialised medical team, stroke intervention and services, and management health policy) available for stroke care within the studied health facilities were either poor, unavailable or grossly insufficient. The state-owned tertiary health facility (RSUTH) suffered the most from unavailable national support and staff development.
At the current state, the stroke facilities available at the 2 teaching hospitals shows high level of inadequacies, unpreparedness and underdevelopment to take up the challenges associated with managing the stroke cases within the study setting.
Recommendation
From the observed findings, the study recommends that: 1. There is an expedient need to develop national and state-level programmes to address the high stroke incidence leading to hospital admissions. 2. Hospitals need to develop community engagement plans and communication strategies to be able to reduce hospital admissions, morbidity and mortality associated with stroke. 3. There is need to develop a resilient health care system that will incorporate development of national and state-level training programmes for managers of stroke. 4. There is an expedient need to develop stroke management policies and guidelines to address stroke triage, inter-hospital transfer, intravenous thrombolysis protocol, intracerebral haemorrhage protocol, decompressive craniectomy protocol, acute stroke care protocol, or TIA triage protocol.
Study Limitation
The study recognises that some information was provided by employees of the health facility may not be accurate, which could have introduced some subjective bias. To reduce the level of bias, after interview with the heads of the various departments, information obtained were cross-checked with the head of hospital administration.
Suggestion for Future Research
The study suggests a comprehensive evaluation of the stroke care structure, process, and outcome in Nigeria tertiary (teaching) hospitals. This will provide a measurable index for the progress and the actions needed to improve the current system.
Supplemental Material
sj-pdf-1-inq-10.1177_00469580211067939 – Supplemental Material for Exploring the Essential Stroke Care Structures in Tertiary Healthcare Facilities in Rivers State, Nigeria
Supplemental Material, sj-pdf-1-inq-10.1177_00469580211067939 for Exploring the Essential Stroke Care Structures in Tertiary Healthcare Facilities in Rivers State, Nigeria by Osborne Ikechuckwu Osuegbu, Foluke Olukemi Adeniji, Golden Chukwuemaka Owhonda, Rogers Bariture Kanee, M Alblihed, Gaber El-Saber Batiha and Eric Osamudiamwen Aigbogun in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
sj-pdf-2-inq-10.1177_00469580211067939 – Supplemental Material for Exploring the Essential Stroke Care Structures in Tertiary Healthcare Facilities in Rivers State, Nigeria
Supplemental Material, sj-pdf-2-inq-10.1177_00469580211067939 for Exploring the Essential Stroke Care Structures in Tertiary Healthcare Facilities in Rivers State, Nigeria by Osborne Ikechuckwu Osuegbu, Foluke Olukemi Adeniji, Golden Chukwuemaka Owhonda, Rogers Bariture Kanee, M Alblihed, Gaber El-Saber Batiha and Eric Osamudiamwen Aigbogun in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgments
The authors acknowledge the co-operation of the Heads of the various units at Rivers State University Teaching Hospital and University of Port Harcourt Teaching Hospital for granting permission to obtain the requisite data for this work and the contributions of the Heads of Nurses and medical records staff at both facilities for their assistance in the collection of data and unlimited access to their facilities. The authors extend their appreciation to Taif University Researchers Supporting Program (project number: TURSP-2020/93), Taif University, Saudi Arabia.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical Approval
Ethical approval was obtained from the Institutional Ethical Committee of the University of Port Harcourt (Ref no: UPH/CEREMAD/REC/MM61/037), Rivers State University Teaching Hospital (Ref no: RSUTH/REC/2020037) and University of Port Harcourt Teaching Hospital (Ref no: UPTH/ADM/90/S.II/VOL.XI/848).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.