
Abstract
A total of 95 patients with hand injuries were admitted to the orthopedics department within half a year of the COVID-19 outbreak. Data were collected between January 23, 2020 and July 23, 2020. Data such as patients' demographics, type of injury, location, side of lesions, mechanism of injury, injury site, and surgical management were collected and subsequently analyzed. On the one hand, the total number of emergency visits due to hand injury during the COVID-19 outbreak decreased by 37%, compared to the same period in the previous year. On the other hand, work resumption injuries increased by 40%. Injuries within the resumption period occurred predominantly at work (64.7%) and were significantly higher than the same period in 2019 (37.3%) (P < .001). Machine-related injuries were the most frequent injuries seen in our hospital (58.8%). The majority of cases were from cut injuries (82.4%), with fingers being the most common site of these injuries. Simple fractures and dislocations were also reported during the study. Most injuries were classified as either minor or moderate (90%) during the outbreak. However, during the resumption of work, major injuries were more prevalent (40%). The proportion of major injuries this year’s work resumption stage (40%) has almost doubled compared to the previous year (21.8%, P = .006). The resumption of work following the COVID-19 outbreak is a time of high-risk for hand injuries. The overall number of patients with hand injuries admitted into our department has decreased compared to the corresponding period last year. However, workplace injuries, particularly machine-related ones, considerably increased during the first six months after the COVID-19 outbreak. As a result, the proportion of major injuries drastically increased. Emergency and surgical health care providers should be aware of this pattern of hand injuries during this untypical time in order to effectively prepare and plan services.
Workplace injuries, in particular machine injuries, as well as the proportional of major injuries, increased significantly following the COVID-19 outbreak
This study attempts to highlight the patterns of hand injuries after the COVID-19 outbreak, the management, and the outcome of these injuries in our hospital.
We hope that this study may disseminate the prevention and management strategies of hand injuries during work resumption in other regions.
Background
In early December 2019, a series of pneumonia cases caused by a novel coronavirus emerged in Wuhan, Hubei Province, China. 1 This coronavirus was first named the 2019 novel coronavirus (2019-nCoV) and was afterward widely recognized worldwide. 2 Indeed, on January 30, 2020, the World Health Organization (WHO) declared this virus a public health emergency of international concern 3 and then officially named it the Coronavirus Disease-2019 (COVID-19) on February 11, 2020. 4 As expected, COVID-19 rapidly developed into a global pandemic that has affected hundreds of countries. Data show that as of November 5, 2021, 248,467,363 confirmed cases and 5,027,183 deaths were recorded worldwide. 5 China has effectively controlled the spread of this epidemic at the start of the outbreak and nonetheless remains vigilant as the situation worsens globally (http://cov.cpu.edu.cn/). On November 5 2021, COVID-19 has already claimed 5696 lives and infected 126,471 people on the Chinese mainland.
The state overall emergency response plan for public emergencies.
In light of these new circumstances, a change in the pattern of hand injuries has attracted attention. Therefore, we summarized the pattern and epidemiology of hand injuries during the COVID-19 outbreak and during the work resumption period as the pandemic subsides. Our dual hypothesis is that hand injuries are more severe and that industrial machine injuries consist of most of these injuries during the work resumption period. Herein, our study attempted to highlight the patterns of hand injuries, their management, and outcomes of these injuries in our hospital after the COVID-19 outbreak. As time passes, other countries have also launched economic recovery programs to mitigate unemployment and stabilize core industries. 12 On that account, we hope that this study may provide guidance for preventing and managing hand injuries in the resumption of work in other regions.
Methods
We present a retrospective study of 95 cases in a designated hospital. All cases were hand injuries registered and assessed in our hospital throughout the epidemic between January 23, 2020 (emergence of the outbreak) and July 23, 2020 (when urban work returned to normal 6 months later). The period between January 23, 2020 and February 9, 2020 was defined as the “outbreak phase” as factories began to re-open on February 10, 2020. On the other hand, the “resumption phase” was defined as the period between February 10, 2020 and July 23, 2020. Data were extracted and collected from databases of the emergency and orthopedics department. A descriptive analysis was then carried out. Data of interest included patient demographics (age and gender), profession, residential address, time and date, and treatment of the injury. The following variables were also collected for each hand injury: type of injury, injury site, side of the lesion, mechanism of injury, area where the injury occurred, surgical management, and outcome. Injuries were classified with the Modified Hand Injury Severity Score (MHISS). The Statistical Package for Social Sciences (SPSS) software (SPSS Statistics 17, for Windows, New York) was used for data analysis. We used the chi-square test, the Fisher exact test, and the Pearson test to assess the Relative Risk (RR) and P-value between groups. Differences with values of p < .05 were considered statistically significant.
Results
A total of 1357 hand-injury related emergency visits were recorded between January 23, 2020 and July 23, 2020, including 46 cases during the outbreak between January 23, 2020 and February 9, 2020, as well as 1311 cases over the resumption of the work period between February 10, 2020 and July 23, 2020. All the patients were tested negative for COVID-19. Over the same period last year, 73 cases of emergency visits associated with hand injuries were recorded between January 23, 2019 and February 9, 2019. Besides, 939 cases were recorded between February 10, 2019 and July 23, 2019. Results indicate that there were 37% fewer cases of emergency visits during the outbreak compared to the same period during the previous year and 40% more cases during the resumption of work than the same period during the previous year. Out of all patients reviewed, 95 (7%) patients were admitted to the hospital and treated in our department, including 10 (21.7%) during the outbreak phase and 85 (6.5%) during the resumption phase.
Hand injuries during the outbreak of pandemic compared with the same period of last year.

Note. MHISS=Modified Hand Injury Severity Score, RR=relative risk, #:P<.05.

Case 1. A 39-year-old female worker suffered a high-pressure injection injury of the left ring finger and palm by disinfectant liquid
Hand injuries during the work resumption of pandemic compared with the same period of last year.

Note. MHISS=Modified Hand Injury Severity Score, RR=relative risk, #:P<.05.
Special cases of hand injuries directly related to this pandemic.
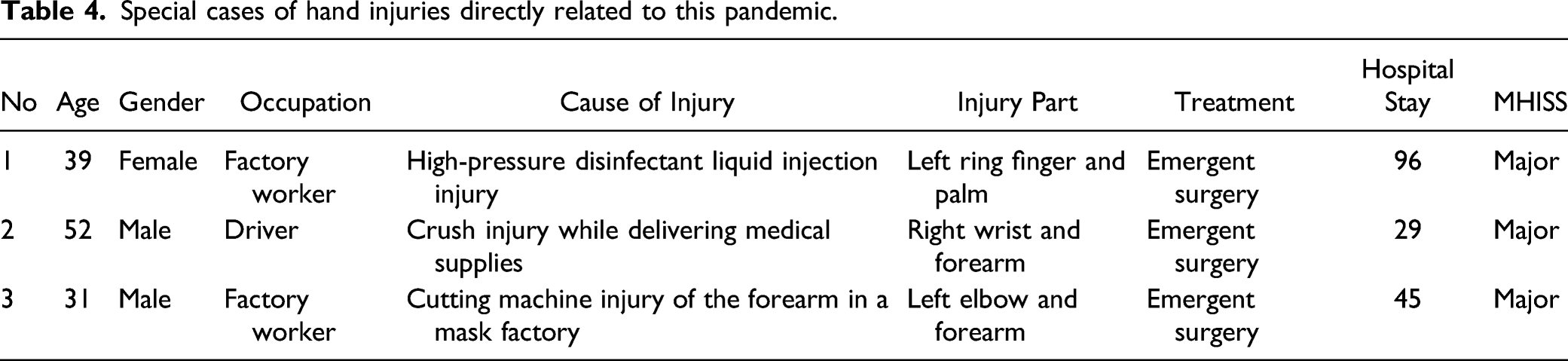

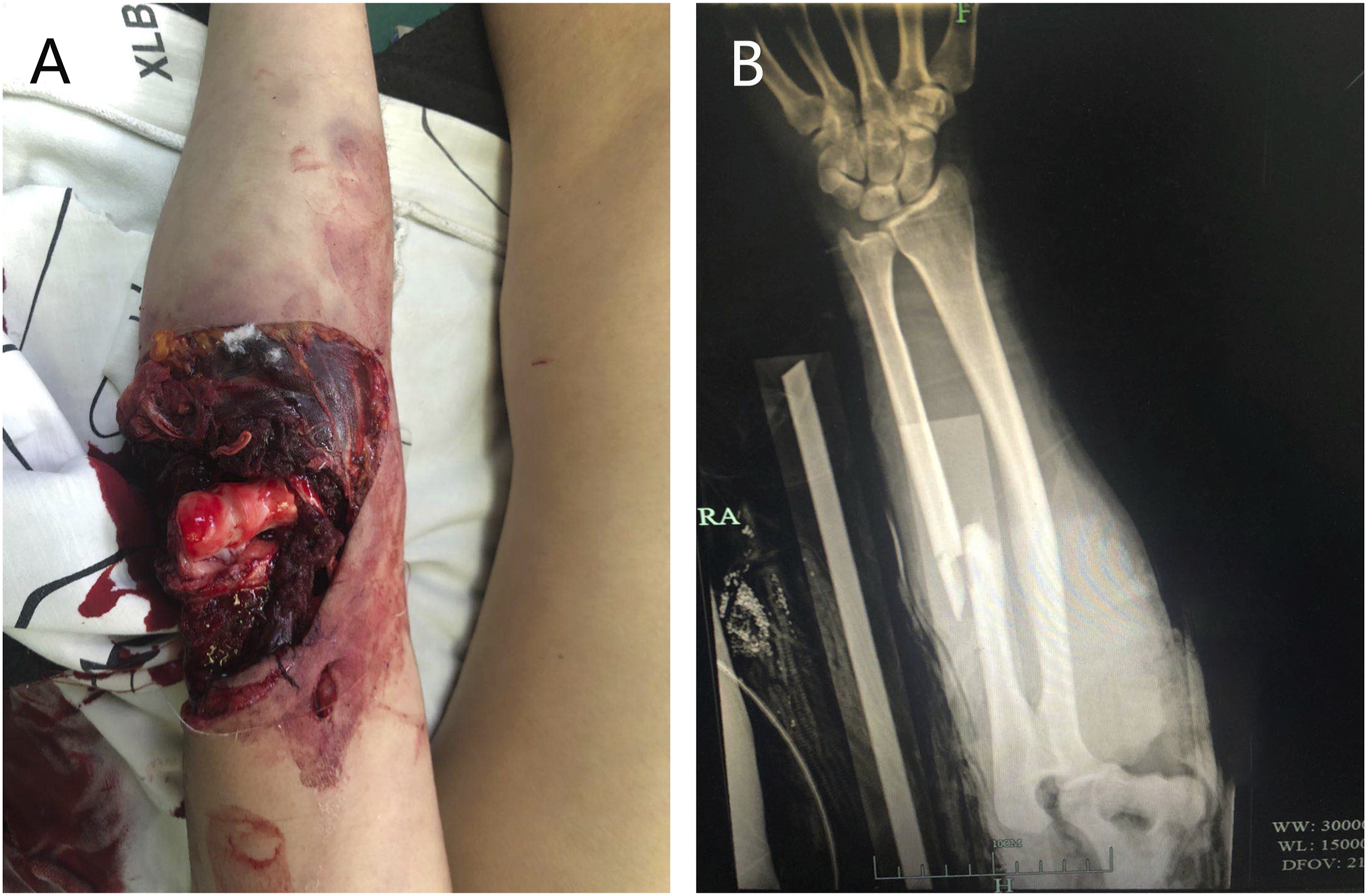
Case 3. A 31-year-old male worker suffered a forearm injury caused by a cutting machine in a mask factory
Case 2. A 52-year-old male driver suffered a crush injury while delivering medical supplies
Discussion
Our study has identified unique patterns of hand injuries during the outbreak and work resumption period following the outbreak. The special pattern of hand injuries during the COVID-19 have given us many clues.
First, social distancing and self-quarantine measures slowed the number of new cases in an attempt to mitigate a surge in demand for health care. 13 Some measures, such as telemedicine, were recommended to reduce hospital visits for some mild injuries.14-16 But patients with severe injuries require urgent treatment. As we reported, emergent upper-extremity injuries and operative cases didn't suffer a significant drop. The number of hand injuries even increased considerably after shelter-in-place orders in some similar studies.17-19 Domestic accidents accounted for most hand injuries during the outbreak period, inevitable as people stayed at home. This finding was similarly reported in other investigations.18-21
Second, with recovery after a long period of economic stagnation, workers successively returned to their workplaces. Local workers without a history of exposure to areas affected by the epidemic were allowed to return to work first. 9 High social demand after a prolonged shutdown has motivated workers to throw themselves into high-intensity work. Thus, workplace injuries, especially traumatic injuries in the manufacturing sector, swiftly increased during the work resumption period. Shortage of life supplies, especially medical supplies, led to an excessive workload borne by the workers who resumed work. It was one of the main reasons for the increased number of injuries encountered in the manufacturing sector.
Third, many enterprises have diverted their routine activities to produce masks and other medical supplies. As expected, hand injuries have increased dramatically for workers without experience in these sectors. Hand injuries in the manufacturing industry of medical supplies were special in this year. As illustrated in our study, the proportion of major injuries has also increased.
Fourth, the study group had a longer mean duration of hospitalization comparing to the control group. The longer duration of hospitalization could be due to the situation in which these injuries occurred during an atypical time when the medical services were slowed down. It added to the medical burden, leading to a strain on medical resources.
According to the clues above, the prevention of hand injuries in this special period mainly focused on three aspects: supervision of factories, educational campaigns of factories employees, and standardized treatment of hospitals. When arriving at hospital, patients were quickly sorted according to the degree of their hand injuries. Those with minor or moderate hand injuries were debrided and bandaged in the emergency department. Patients with major injuries were provided green channels to receive all of the preoperative tests in priority. Despite the necessity of ensuring practical examinations, the time required for emergency preoperative preparations was not significantly prolonged during the epidemic. As a result of efficient cooperation between various departments in our center, emergency patients during this special time received prompt treatment as always.
Hangzhou was the first city in China to launch a health QR code system to curb the spread of infection as it tentatively restarted production.22,23 Only patients with a green QR code and normal body temperature were allowed into the emergency department. Patients suspected of being infected were examined in a separate CT room, distinct from those used for afebrile patients. Statements with a consensus agreement from an international Delphi process supported a distinction of surgery between protocols involving patients with suspected COVID-19 and those perceived to be free from infection. 24 Serological tests, medical evaluation and preparation of the surgical plan were performed while awaiting the results of the COVID-19 test. As direct contact poses a high-risk for health care professionals performing wound care, surgery, and resuscitation,13,25 the appropriate use of personal protective equipment, strict disinfection and hand hygiene are required of surgeons.13,26 It is worth mentioning that a total of 105 patients with COVID-19 have been cured in our hospital. None of the staff has been infected, and SARS-Cov-2 RNA was not detected amongst objective sampling, including from the isolation wards. 27
On the global scale, there was also a surge in injuries resulting from high-risk behavior and lawlessness, suicidality, lack of usual social and physical resources, home improvement projects, and avoidance of health care facilities. 17 As a result of pandemic and economic stagnation, members of the public have also experienced an increase in psychological distresses.28,29 Research has suggested that anxiety, depression, and stress in workers may increase the risk of unintentional injuries during the resumption of work. 30 This is a time for solidarity and not fear; the COVID-19 outbreak is a test of solidarity in the political, financial, and scientific spheres, as stated by WHO Director-General Tedros Adhanom Ghebreyesus. 31 Thus, all doctors in our center have remained at their posts since the outbreak in a show of solidarity.
Conclusion
The resumption of work following the COVID-19 outbreak is a time of increased risk for hand injuries. The overall number of hand injury-related hospitalized cases has decreased compared to the corresponding period last year. However, domestic accidents increased during the outbreak period, while workplace injuries, particularly machine injuries, increased significantly over the six months following the COVID-19 outbreak. In addition, the proportion of major injuries markedly increased. Emergency and surgical service providers should be aware of this pattern of hand injuries throughout this unique time so that they can prepare and plan services accordingly.
Footnotes
Acknowledgments
I’d like to show my sincere gratitude to my colleague Hui Lu who gave me support in every step of this study. Also, I really appreciate the funding program for sponsoring our research. Besides, I want to thank my husband, Lawyer Hui Cai, for helping me with the figures and ethical principles.
Authors Contributions
Qianjun Jin conceived of the study Hui Lu and Haiying Zhou participated in the design of the studyQianjun Jin and Haiying Zhou drafted the manuscriptAll authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Zhejiang Provincial Natural Science Foundation of China (LY20H060007, LS21H060001) and Zhejiang Medicine and Hygiene Research Program (2022RC139).