COVID-19 is an established challenge to the health care professionals (HCPs) having physical, emotional, and psychological repercussions. We determine the perceptions of Pakistani HCPs regarding the risks and deaths related to COVID-19. A cross-sectional study was conducted among HCPs throughout Pakistan from 16th February 2021 to 6th March 2021 by disseminating an online Google questionnaire via all possible social media platforms including WhatsApp, Facebook, Twitter, and emails. Out of total of 462 HCPs, 33.55% tested COVID-19 positive and 49.43% had received their first dose of COVID-19 vaccine. The proportion of HCPs worried about contracting COVID-19 was 46.97%. A total of 69.48% mentioned that doctors are at a higher risk of dying from COVID-19 infection compared to the general population. In a dichotomous analysis done for risk perception, 72.06% of doctors reported a high-risk perception of contracting COVID-19 in hospital settings. The main reasons identified to be associated with higher mortality amongst the HCPs, specifically doctors, included comorbidities (47.26%), working in high-risk wards (24.02%) and lack of adequate personal protective equipment (PPE) (28.72%). Using univariate and multivariate regression the HCPs tested positive rated two-fold high risk while performing professional duty during COVID-19 pandemic [unadjusted odds ratio (OR) (95% confidence interval (CI)): 2.23 (1.24–4.02), P = .007; adjusted OR (95% CI) 2.27 (1.22–4.19), P = .009]. In conclusion, Pakistani HCPs have significant COVID–19-related concerns and anxieties. The doctors perceived to be at a higher risk of dying with COVID-19, due to a variety of personal and professional reasons.
COVID-19 posing some key challenges to the health care professionals (HCPs) including emotional and psychological distress.
How Does Your Research Contribute to the Field?
The views and experiences of the frontline HCPs in Pakistan about working through the pandemic had not been documented or its evidence published. To the best of our knowledge, this will be the first survey conducted in Pakistan.
What Are Your Research’s Implications Toward Theory, Practice, or Policy?
Need key steps and measures to be implemented to help the frontline health workers to relieve their anxieties regarding contracting COVID-19.
Introduction
The healthcare system around the world had been severely affected by the global outbreak of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) which caused COVID-19. In addition to the risk of workplace infection acquisition, management of this pandemic is posing a lot of challenges to the workforces in the department of healthcare.1 According to the reports, almost 3400 health care professionals (HCPs) acquired the infection in the two months following the reporting of the first case of COVID-19 in China. This picture was even grimmer in Europe and Italy where proportions greater than those of China were reported to be affected.2
When HCPs are infected, it is not only they who suffer serious morbidity and mortality but there are also high chances of transmission of infection to their close contacts, as well as to their patients and other colleagues. This can result in a shortage of staff at health care facilities at a time when there is already an increased workload and demand for healthcare services. In a study conducted in Wuhan immediately after the beginning of this pandemic, 138 patients were analyzed and it was revealed that 41% of the patients acquired the infection through hospitals.3 Health care professionals had also been seen to undergo significant emotional and psychological trauma associated with deaths of fellow HCPs from the hospital-acquired COVID-19.4
During pandemic, globally, HCPs are concerned about the insufficient availability of personal protective equipment. This made them anxious and results in inefficiency on the part of HCPs.1 It had also been seen in different countries specifically England that mortality from COVID-19 is greater in certain ethnic groups like Blacks and Asians. This caused increased concern among such ethnic groups in the general population as well as the HCPs.5 In a study conducted in NHS, 119 deaths from COVID-19 among the NHS staff were analyzed and it was seen that more people from minority groups other than White British and specifically of BAME origin, suffered mortality. In this study, doctors and dentists had a death rate of 94%, nurses 71%, and support workers had a mortality of 56%. These disparities have called for survey to look for as to why certain groups are at a higher risk of morbidity and mortality.6
In Pakistan, as of 14th September 2021, a total of 17 866 HCPs were infected while 17 301 (95.58%) have recovered and 565 active cases. A total of 169 deaths were reported among which 103 (61%) were doctors, 5 (3%) nurses, and 61 (36%) paramedic staff.7 The views and experiences of the frontline HCPs in Pakistan about working through the pandemic had not been documented or its evidence published. This study aimed to collect and analyze the views and experiences of Pakistani HCPs regarding the risks and deaths from the workplace related to COVID-19 and particularly among doctors working during the response to the pandemic.
Methods
During the response to COVID-19, we conducted a cross-sectional study among HCPs working in Pakistan. The study protocol was approved by the Khyber College of Dentistry Ethics Review Board (No17/ADR/KCD). We adopted the study questionnaire of Parveen Ali et al conducted by the School of Health Sciences, University of Sheffield, in the UK.8 The questionnaire was adapted to the local context and finalized by peer review of Public Health Department and Social Sciences-Khyber Medical University Peshawar, Khyber Pakhtunkhwa, Pakistan before it was implemented.
The survey was conducted from 16th February to 6th March 2021. The HCPs aging 20 or older with a valid Ex-PMDC/PMC license for Doctors, PNC registration for Nurses and Medical Faculty Registration/Government Personal Number for Paramedics were inclusion criteria to join the survey and were working in Pakistan during the pandemic emergency. Those who did not have valid registration and not meeting the criteria were excluded.
The Google online self-reported questionnaire was circulated using various social media platforms including WhatsApp, Twitter, Facebook, and email groups. The details collected were divided into 4 parts. (1) Demographic details of the HCPs, (2) COVID-19 risk perception of HCPs, (3) Perception about deaths in all HCPs and (4) COVID-19 risk perception and death particularly related to doctors.
Statistical analysis was performed using STATA 14. All the Continuous variables are presented as mean ± SD and categorical variables as percentages or proportions. Furthermore, categorical variables were analyzed through the Chi-square test. Binary logistic regression is used for multivariate analyses to explore independent predictors for a response and the results are presented as odds ratio (OR) with 95% confidence intervals (CI). A P-value less than .05 was chosen as the cut-off for the statistical significance of the test.
Results
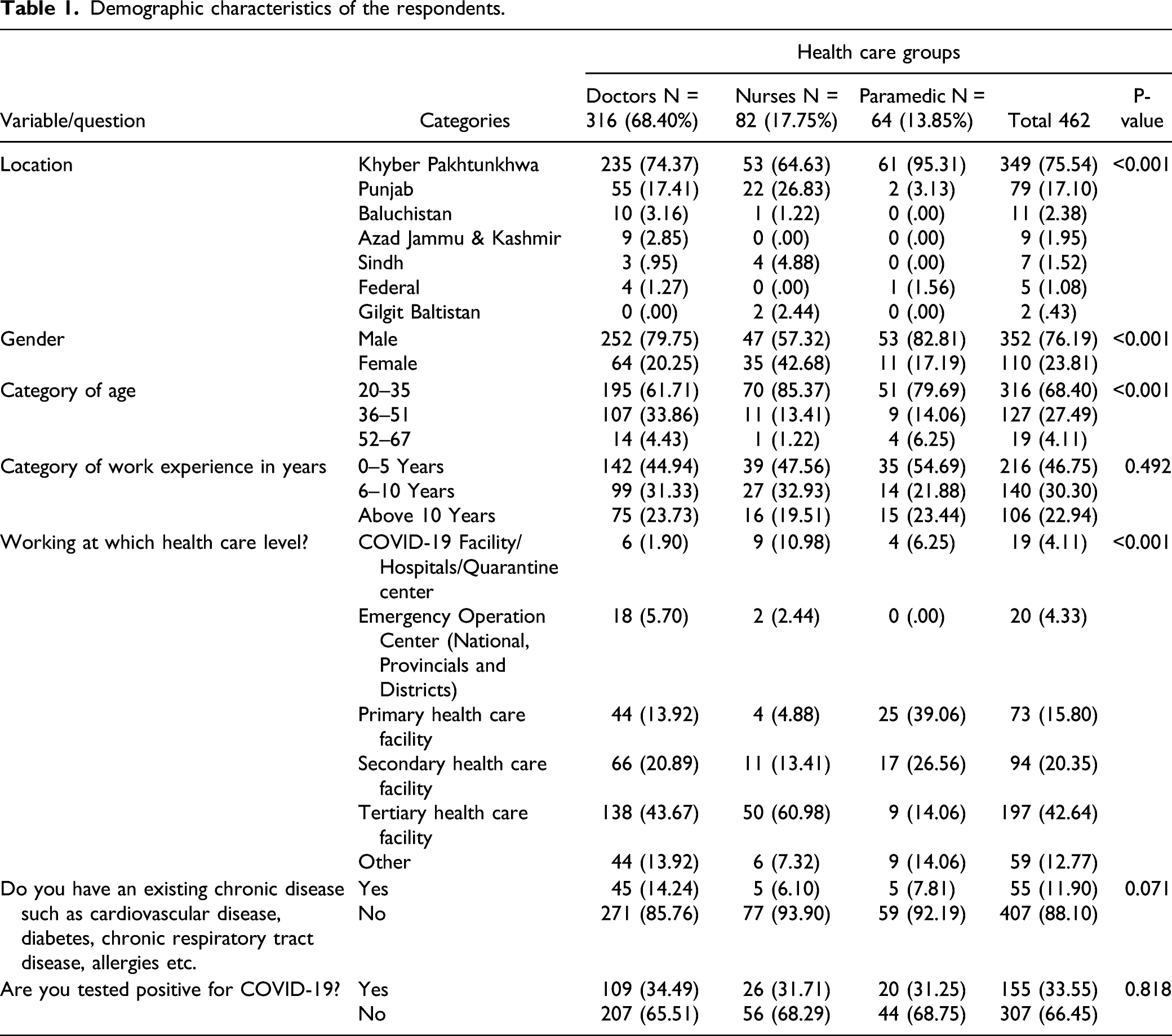
In total, 462 HCPs responded to our survey. Of these, 316 (68.40%) were doctors, 82 (17.75%) were nurses, and 64 (13.85%) were paramedical staff. The respondents were predominantly males (n = 352; 76.19%).Most of the respondents (n = 197; 42.64%) were working in the tertiary care hospitals followed by the secondary care hospitals (n = 94; 20.35%) and primary care hospitals (n = 73; 15.80%). The proportion of HCPs working at emergency operation centers was 4.3% (20).Around one-third HCPs (n = 155; 33.55%) were tested COVID-19 positive in our study. Further details on the respondent’s characteristics are provided in Table 1.
Demographic characteristics of the respondents.
Variable/question
Categories
Health care groups
Doctors N = 316 (68.40%)
Nurses N = 82 (17.75%)
Paramedic N = 64 (13.85%)
Total 462
P-value
Location
Khyber Pakhtunkhwa
235 (74.37)
53 (64.63)
61 (95.31)
349 (75.54)
<0.001
Punjab
55 (17.41)
22 (26.83)
2 (3.13)
79 (17.10)
Baluchistan
10 (3.16)
1 (1.22)
0 (.00)
11 (2.38)
Azad Jammu & Kashmir
9 (2.85)
0 (.00)
0 (.00)
9 (1.95)
Sindh
3 (.95)
4 (4.88)
0 (.00)
7 (1.52)
Federal
4 (1.27)
0 (.00)
1 (1.56)
5 (1.08)
Gilgit Baltistan
0 (.00)
2 (2.44)
0 (.00)
2 (.43)
Gender
Male
252 (79.75)
47 (57.32)
53 (82.81)
352 (76.19)
<0.001
Female
64 (20.25)
35 (42.68)
11 (17.19)
110 (23.81)
Category of age
20–35
195 (61.71)
70 (85.37)
51 (79.69)
316 (68.40)
<0.001
36–51
107 (33.86)
11 (13.41)
9 (14.06)
127 (27.49)
52–67
14 (4.43)
1 (1.22)
4 (6.25)
19 (4.11)
Category of work experience in years
0–5 Years
142 (44.94)
39 (47.56)
35 (54.69)
216 (46.75)
0.492
6–10 Years
99 (31.33)
27 (32.93)
14 (21.88)
140 (30.30)
Above 10 Years
75 (23.73)
16 (19.51)
15 (23.44)
106 (22.94)
Working at which health care level?
COVID-19 Facility/Hospitals/Quarantine center
6 (1.90)
9 (10.98)
4 (6.25)
19 (4.11)
<0.001
Emergency Operation Center (National, Provincials and Districts)
18 (5.70)
2 (2.44)
0 (.00)
20 (4.33)
Primary health care facility
44 (13.92)
4 (4.88)
25 (39.06)
73 (15.80)
Secondary health care facility
66 (20.89)
11 (13.41)
17 (26.56)
94 (20.35)
Tertiary health care facility
138 (43.67)
50 (60.98)
9 (14.06)
197 (42.64)
Other
44 (13.92)
6 (7.32)
9 (14.06)
59 (12.77)
Do you have an existing chronic disease such as cardiovascular disease, diabetes, chronic respiratory tract disease, allergies etc.
Yes
45 (14.24)
5 (6.10)
5 (7.81)
55 (11.90)
0.071
No
271 (85.76)
77 (93.90)
59 (92.19)
407 (88.10)
Are you tested positive for COVID-19?
Yes
109 (34.49)
26 (31.71)
20 (31.25)
155 (33.55)
0.818
No
207 (65.51)
56 (68.29)
44 (68.75)
307 (66.45)
Table 2 summarizes the perceptions of HCPs about COVID-19 related risks and deaths. When asked if they had received the first dose of COVID-19 vaccine, freely available by the Government; about half (n = 229; 49.57%) had not received yet while 3.03% (n = 14) refused to get vaccinated. Nearly half of HCPs (n = 217; 46.97%) were worried about being infected with COVID-19 and another 41.9% (194) of the HCPs expressed their concerns about the presence of COVID-19 affecting their ability to care for the patients negatively. The risks related to COVID-19 were raised with concerned supervisors by 43.72% of the HCPs and another 21.86% raised concerns about the non-availability of adequate Personal Protective Equipment (PPE). More than half 53.2%5 (246) of the HCPs refused to work without adequate PPE provision, while 22.29% (103) were afraid that refusing to work without adequate PPE may affect their relationship with the employer. Nearly two-third, 285 (61.69%) were of opinion that HCPs contracted COVID-19 most commonly at hospitals/workPlace. While two-third, that is, 334 (72.29%) respondents identified lack of adequate PPE as a contributing factor to HCPs deaths. Approximately 32.9% of the HCPs were in favor of timely investigations of COVID–19-related deaths among HCPs, while another 24.7% showed concerns over the government’s response toward providing some compensation to the families of the deceased HCPs. The majority (76.84%) of the respondents perceived the health care setting as high risk for COVID-19 infection. The mean perceived risk score of HCPs contracting COVID-19 outside the work environment was 5.2 (2.5). Totally, 134 (29.00%) of the respondents believe it as high risk and 118 (25.54) perceived it low risk at all. Approximately 69% of the HCPs were worried about the news of COVID–19-related HCPs deaths in Pakistan. When asked about identifying the places or situations during which HCPs have more chances of contracting COVID-19, the most common response was emergency units (47.84%) followed by hospital wards, Outpatient Departments, Operation theatures, workplace offices (20.56%), and Intensive Care Unit (ICU) Wards (5.41%).Among the different cadres of frontline HCPs, doctors were believed to be at the highest risk of COVID-19 infection (82%), while 69.5% believed that doctors were also at a higher risk of dying of the infection which they attributed mostly to comorbidities (49.6%) followed by to lack of adequate PPE and infection prevention training (27.49%) and working in high-risk wards (22.9%) (Table 3).
Perceptions about COVID–19-related risks and death among health care professionals.
Questions
Categories
Health care groups
Doctors N = 316 (68.40%)
Nurses N = 82 (17.75%)
Paramedic N = 64 (13.85%)
Total 462
P-value
Had you received COVID-19 vaccine 1st dose freely available by Government?
No
148 (46.84)
34 (41.46)
47 (73.44)
229 (49.57)
<0.001
Yes
80 (25.32)
19 (23.17)
1 (1.56)
100 (21.65)
It’s still not available at my work place
44 (13.92)
5 (6.10)
11 (17.19)
60 (12.99)
I am waiting for my turn
37 (11.71)
17 (20.73)
5 (7.81)
59 (12.77)
I refused to take it
7 (2.22)
7 (8.54)
0 (.00)
14 (3.03)
If you have been worried about getting infected from COVID-19, does it affect your ability to care for your patients?
Yes
157 (49.68)
34 (41.46)
26 (40.63)
217 (46.97)
0.441
No
124 (39.24)
38 (46.34)
32 (50.00)
194 (41.99)
I Prefer not to answer
35 (11.08)
10 (12.20)
6 (9.38)
51 (11.04)
If you have been worried about your health due to COVID-19, have you raised this with your head of department/DHO/MS/DMS/Health manager?
Yes
148 (46.84)
36 (43.90)
18 (28.13)
202 (43.72)
0.068
Sometimes
99 (31.33)
24 (29.27)
24 (37.50)
147 (31.82)
Never
69 (21.84)
22 (26.83)
22 (34.38)
113 (24.46)
Do you have concerns about non-availability of adequate personal protective equipment (PPE)?
Yes, but my concerns have been addressed
121 (38.29)
42 (51.22)
30 (46.88)
193 (41.77)
0.001
Yes and my concerns remain unaddressed
134 (42.41)
21 (25.61)
13 (20.31)
168 (36.36)
No, I don’t have any concerns about provision of PPE
61 (19.30)
19 (23.17)
21 (32.81)
101 (21.86)
Can you say “no,” if you are asked to work without adequate PPE?
Yes
161 (50.95)
49 (59.76)
36 (56.25)
246 (53.25)
0.264
No, as it may affect my relationship with employer
74 (23.42)
13 (15.85)
16 (25.00)
103 (22.29)
No, as I fear losing my job
66 (20.89)
13 (15.85)
11 (17.19)
90 (19.48)
No, I prefer to resign and quit from job
15 (4.75)
7 (8.54)
1 (1.56)
23 (4.98)
Where do you think health care professionals are infected with COVID-19?
Mostly at hospitals/Work place
207 (65.51)
42 (51.22)
36 (56.25)
285 (61.69)
0.025
Mostly outside hospitals
8 (2.53)
2 (2.44)
5 (7.81)
15 (3.25)
Both of the above
101 (31.96)
38 (46.34)
23 (35.94)
162 (35.06)
Do you think lack of adequate PPE may have been a contributing factor to health care professionals deaths?
Yes
237 (75.00)
62 (75.61)
35 (54.69)
334 (72.29)
0.014
I Am not sure
56 (17.72)
12 (14.63)
21 (32.81)
89 (19.26)
No
23 (7.28)
8 (9.76)
8 (12.50)
39 (8.44)
Do you think that government should initiate enquiry into deaths of health care professionals due to COVID-19 in a timely manner?
We are demanding enquiries and compensation but not addressed by government
118 (37.34)
25 (30.49)
9 (14.06)
152 (32.90)
<0.001
I don’t know
81 (25.63)
11 (13.41)
23 (35.94)
115 (24.89)
No any positive steps taken from government
69 (21.84)
32 (39.02)
13 (20.31)
114 (24.68)
Yes, it is already in process
48 (15.19)
14 (17.07)
19 (29.69)
81 (17.53)
Questions
Categories
Health care groups
Doctors N = 316 (68.40%)
Nurses N = 82 (17.75%)
Paramedic N= 64 (13.85%)
Total 462
P-value
What is yours risk perception of COVID-19 during professional duty in the next 30 days?
Low risk
10 (3.16)
6 (7.32)
15 (23.44)
31 (6.71)
<0.001
Medium risk
43 (13.61)
21 (25.61)
12 (18.75)
76 (16.45)
High risk
263 (83.23)
55 (67.07)
37 (57.81)
355 (76.84)
What is yours risk perception of COVID-19 during personal life in the next 30 days?
Low risk
80 (25.32)
19 (23.17)
19 (29.69)
118 (25.54)
0.004
Medium risk
160 (50.63)
30 (36.59)
20 (31.25)
210 (45.45)
High risk
76 (24.05)
33 (40.24)
25 (39.06)
134 (29.00)
Have you been worried about NEWS of COVID-19 related deaths in health care professionals Pakistan?
Less worried
24 (7.59)
14 (17.07)
13 (20.31)
51 (11.04)
0.001
Much worried
56 (17.72)
17 (20.73)
18 (28.13)
91 (19.70)
Very much worried
236 (74.68)
51 (62.20)
33 (51.56)
320 (69.26)
Can you identify the places or situations during which you have more chances of getting COVID-19?
Emergency
161 (50.95)
37 (45.12)
23 (35.94)
221 (47.84)
<0.001
Ward, Outpatient Department, Operation theature, and working place offices
73 (23.10)
10 (12.20)
12 (18.75)
95 (20.56)
Contact with suspected COVID-19 case
47 (14.87)
15 (18.29)
19 (29.69)
81 (17.53)
Taking history of confirmed COVID-19 case
26 (8.23)
5 (6.10)
9 (14.06)
40 (8.66)
Intensive Care Unit while ward
9 (2.85)
15 (18.29)
1 (1.56)
25 (5.41)
COVID-19 risk perceptions related to doctors among health care professionals.
Questions
Categories
Health care groups
Doctors N = 316 (68.40%)
Nurses N = 82 (17.75%)
Paramedic N = 64 (13.85%)
Total 462
P-value
Among health care professionals, in your opinion where do doctors get mostly infected with COVID-19 ?
Doctors more likely infected with COVID-19 at hospital/Work place
278 (87.97)
44 (53.66)
45 (70.31)
367 (79.44)
<0.001
Doctors are infected with COVID-19 same as non-doctors
9 (2.85)
22 (26.83)
13 (20.31)
44 (9.52)
Doctors are doing long shift duties
24 (7.59)
10 (12.20)
2 (3.13)
36 (7.79)
Doctors more likely to infected with COVID-19 outside hospital
5 (1.58)
6 (7.32)
4 (6.25)
15 (3.25)
Among health care professionals, do you think doctors are at a higher risk of being infected with COVID-19?
Yes
296 (93.67)
37 (45.12)
46 (71.88)
379 (82.03)
<0.001
No
14 (4.43)
37 (45.12)
14 (21.88)
65 (14.07)
I don’t Know
6 (1.90)
8 (9.76)
4 (6.25)
18 (3.90)
Among health care professionals, do you think doctors are at higher risk of dying with COVID-19?
Yes
252 (79.75)
32 (39.02)
37 (57.81)
321 (69.48)
<0.001
No
29 (9.18)
40 (48.78)
14 (21.88)
83 (17.97)
I dont Know
35 (11.08)
10 (12.20)
13 (20.31)
58 (12.55)
Among health care professionals, what do you think is the reason for increase doctors deaths?
Comorbidities (diabeties, hypertension, asthma etc) in doctors
159 (50.32)
39 (47.56)
31 (48.44)
229 (49.57)
0.062
Doctors are working in high risk wards/ICUs
78 (24.68)
11 (13.41)
17 (26.56)
106 (22.94)
Lack of adequate PPE & trianing for doctors
79 (25.00)
32 (39.02)
16 (25.00)
127 (27.49)
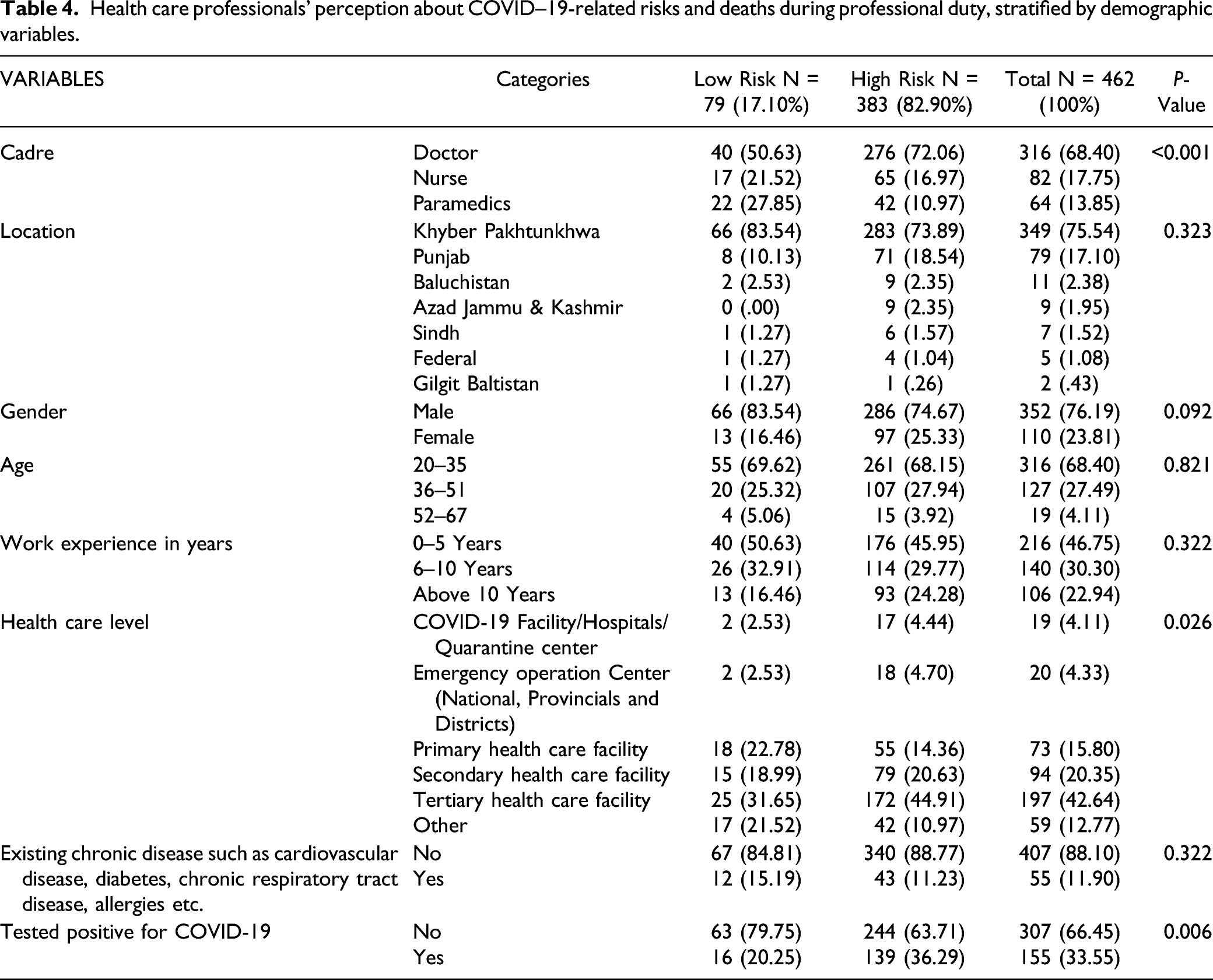
Data-specific COVID–19-related risk perception, among HCPs, during professional duty hours, was collected on a scale of 0–10 where 0 meant “No risk” while 10 meant “highest risk.” The mean perceived risk score of HCPs contracting COVID-19 in the health care setting was 7.9 (2.4). The overall risk score was stratified into two categories: low risk (0–5 score) and high risk (6–10 score). More than two-third of doctors (72.06%) reported a high-risk of contracting COVID-19 while performing professional duty, while the proportion of nurses and paramedics concerned about being infected during duty hours was low (16.97% and 10.97%, respectively). The concern was highest amongst the males (74.7%), those aged 20–35 years (68%), and working in a tertiary care setting (44.9%) (Table 4).
Health care professionals’ perception about COVID–19-related risks and deaths during professional duty, stratified by demographic variables.
VARIABLES
Categories
Low Risk N = 79 (17.10%)
High Risk N = 383 (82.90%)
Total N = 462 (100%)
P-Value
Cadre
Doctor
40 (50.63)
276 (72.06)
316 (68.40)
<0.001
Nurse
17 (21.52)
65 (16.97)
82 (17.75)
Paramedics
22 (27.85)
42 (10.97)
64 (13.85)
Location
Khyber Pakhtunkhwa
66 (83.54)
283 (73.89)
349 (75.54)
0.323
Punjab
8 (10.13)
71 (18.54)
79 (17.10)
Baluchistan
2 (2.53)
9 (2.35)
11 (2.38)
Azad Jammu & Kashmir
0 (.00)
9 (2.35)
9 (1.95)
Sindh
1 (1.27)
6 (1.57)
7 (1.52)
Federal
1 (1.27)
4 (1.04)
5 (1.08)
Gilgit Baltistan
1 (1.27)
1 (.26)
2 (.43)
Gender
Male
66 (83.54)
286 (74.67)
352 (76.19)
0.092
Female
13 (16.46)
97 (25.33)
110 (23.81)
Age
20–35
55 (69.62)
261 (68.15)
316 (68.40)
0.821
36–51
20 (25.32)
107 (27.94)
127 (27.49)
52–67
4 (5.06)
15 (3.92)
19 (4.11)
Work experience in years
0–5 Years
40 (50.63)
176 (45.95)
216 (46.75)
0.322
6–10 Years
26 (32.91)
114 (29.77)
140 (30.30)
Above 10 Years
13 (16.46)
93 (24.28)
106 (22.94)
Health care level
COVID-19 Facility/Hospitals/Quarantine center
2 (2.53)
17 (4.44)
19 (4.11)
0.026
Emergency operation Center (National, Provincials and Districts)
2 (2.53)
18 (4.70)
20 (4.33)
Primary health care facility
18 (22.78)
55 (14.36)
73 (15.80)
Secondary health care facility
15 (18.99)
79 (20.63)
94 (20.35)
Tertiary health care facility
25 (31.65)
172 (44.91)
197 (42.64)
Other
17 (21.52)
42 (10.97)
59 (12.77)
Existing chronic disease such as cardiovascular disease, diabetes, chronic respiratory tract disease, allergies etc.
No
67 (84.81)
340 (88.77)
407 (88.10)
0.322
Yes
12 (15.19)
43 (11.23)
55 (11.90)
Tested positive for COVID-19
No
63 (79.75)
244 (63.71)
307 (66.45)
0.006
Yes
16 (20.25)
139 (36.29)
155 (33.55)
The COVID–19-related risk perception was high amongst only 11.2% of HCPs with comorbidities, whereas 36.3% of those previously infected with COVID-19 had a high risk perception of being infected during professional duty. Nearly half (47.52%) of those who had not received first dose COVID-19 vaccine reported high professional duty–related COVID-19 risk. Totally, 153 (39.95%) with high-risk perception worried that COVID-19 affects the ability to care for patients. The association between demographic characteristics and the COVID–19-related risk perception was further explored using univariate and multivariate logistic regression analysis. The outcome was risk perception, classified either as high risk or low risk, and the results are presented as OR (95%CI). HCPs tested positive rated high risk while performing professional duty during COVID-19 pandemic [unadjusted OR 2.23, 95% CI 1.24–4.02, P = .007; adjusted OR 2.27, 95% CI 1.22–4.19, P = .009. The details are given in Table 03. The odds of high COVID–19-related risk perceptions were significantly higher in doctors compared to nurses and paramedics in both unadjusted and adjusted analysis (P < .05). Similar results were obtained for those HCPs who tested positive for COVID-19 previously. Adjusted analysis showed males were more concerned about COVID–19-related risks than females (P = .04). On the contrary, age, work experience, level of health care facility and presence of any comorbidity was not associated with the perception level of COVID-19 related risk in both unadjusted and adjusted analysis (all P > .05) (Table 5)
Association of health care professional’s perception about COVID–19-related risks and deaths with different demographic variables (N = 462).
Characteristics
Univariate analysis
Multivariate analysis
OR (95% CI)
P-value
OR (95% CI)
P-value
Are you
Doctor
Reference
Reference
Nurse
.55 (.298–1.0)
.06
.33 (.16–.68)
0.003
Paramedics
.27 (.15–.51)
.001
267 (.13–.54)
0.001
Gender
Male
Reference
Reference
Female
1.73 (.91–3.2)
.09
2.01 (1.01–4.19)
0.04
Age
20–35
Reference
Reference
36–51
1.10 (.63–1.93)
.723
.48 (.24–1.25)
0.15
52-67
.79 (.253–2.47)
.686
.40 (.09–1.76)
0.22
Work experience
0-5 Years
Reference
Reference
6–10 Years
.97 (.56–1.6)
.94
.99 (.52–1.87)
0.97
Above 10 Years
1.62 (.82–3.19)
.15
2.4 (.89–6.63)
0.08
Health care level
COVID-19 Facility/Hospitals/Quarantine center
Reference
Reference
EOC (National, Provincial & Districts)
1.059 (.134–8.38)
.95
.54 (.06–4.7)
0.58
Primary health care facility
.35 (.076–1.70)
.19
.30 (.60–1.50)
0.15
Secondary health care facility
.62 (.129–2.96)
.54
.41 (.08–2.13)
0.29
Tertiary health care facility
.80 (.17–3.70)
.78
.48 (.09–2.30)
0.36
Other
.27 (.058–1.30)
.10
.15 (.03–.79)
0.02
Co-morbidities
No
Reference
Reference
Yes
.71 (.35–1.4)
.332
.72 (.32–1.6)
0.43
Tested positive
No
Reference
Reference
Yes
2.23 (1.24–4.02)
.007
2.27 (1.22–4.19)
0.009
Discussion
Our study aims to determine the perception and experiences of Pakistani HCPs regarding the risks and deaths related to COVID-19 and particularly among doctors working during the response to the pandemic. Our study results showed that 33.55% tested COVID-19 positive and nearly half of them received their first dose of the COVID-19 vaccine. The proportion of HCPs worried about contracting COVID-19 was 46.97%. A total of 69.48% mentioned that doctors are at a higher risk of dying from COVID-19 infection. In a dichotomous analysis done for risk perception, more than three quarters of doctors reported a high-risk perception of contracting COVID-19. The main reasons identified to be associated with higher mortality included comorbidities, working in high-risk wards and lack of adequate personal protective equipment. The HCPs who tested positive previously reported a two-fold higher risk of contracting COVID-19 while performing professional duty
It was observed in a study that HCPs had prominent apprehensions regarding deaths from COVID-19. During the outbreaks of the SARS coronavirus as well as in H1N1 influenza outbreak, it was reported that the HCPs feel anxious, vulnerable, and distressed.9,10 Likewise, in China, the HCPs who delivered care to the COVID-19 patients were reportedly symptomatic of psychological stress.11 Among the factors contributing to the psychological distress of HCPs, the most notable included fear that they would pass the infection to their families and close contacts. On the other hand, a recent survey in England identified moderate levels of emotional exhaustion, low levels of depersonalization, and high levels of personal achievement. These results, coupled with the positive financial impact by the majority of doctors and the increased workload, create an environment of mixed positive and negative consequences. This probably indicates the resilience of junior and middle-grade doctors, who, despite the increased workload and adverse effects of the pandemic, reported high levels of personal achievement. Based on our analysis, we feel that there is a need to advise the HCPs about measures to deal with mental distress associated with COVID-19.10,12 In our study, it was found that most of the respondents 61.69% feel that hospitals/workplaces were the source of infection. A very less proportion of 3.25% thinks that infections might have been acquired by the HCPs from outside of workplaces. A study conducted elaborates that only 3% of the respondents were found to be thinking that the HCPs could have acquired the infection from outside of their workplace. The researcher of the study suggested that COVID-19 should be considered as a ‘work-related disease and also an occupational hazard for HCPs.13 Data obtained from China suggests that the availability and usage of proper PPE with rigorous enforcement of SOPs can prevent HCPs from becoming infected with coronavirus and protect against the subsequent risk of death.14 In our survey, the majority of the participants 72.29%, showed concerns about the non-availability of PPE. A survey conducted by the Royal College of Nursing in Scotland reported similar findings showing concerns about PPE availability by 69% of the respondents.15 Another recent survey by British Medical Association also suggested that nearly half of the doctors have obtained their own.16 Although the HCPs may perceive the PPE to be inadequate when it is available in sufficient quantity. However, there is criticism on the guidelines provided by Public Health England about PPE regarding them as inadequate in terms of availabilities for HCPs.17 While it may be desirable to get the “best possible” PPE, supply issues are not infrequent during pandemics.18 In our study, about two-thirds, 69.48%, of respondents thought that among HCPs, doctors who were performing their duties during a response to a pandemic are at higher risk of mortality from COVID-19. This may be due to the weak health care system in Pakistan and the inability of the health care workers to cope with the intense burden of the pandemic.19 The infection control practices and availability of PPE are also poor in most of the hospitals.20
In this study, those HCPs who were tested positive perceived performing professional duty during the COVID-19 pandemic as a high risk for contracting the COVID-19 and being affected by its associated complications including mortality. The possible reasons for this perception, other than the common exposure to COVID-19 patients, may be higher fatigue levels and a less secure working environment.21 Other studies from the developed and developing countries support that Health Care workers who were positive suffered greatly from stress, anxiety, and considered themselves at high risk of COVID-19 and associated risks.19,22,23 In our study, likewise, about half of the doctors attributed mortality to comorbid conditions such as diabetes, hypertension, and asthma, while one-third attributed it to insufficient availability of PPE. Similar findings have been reported in studies where the COVID–19-related mortality is reported to be associated with comorbid health conditions.24,25 Although our participants working in the wards/ICUs rated these places as high-risk workplaces, the literature showed that working in the intensive care unit was not associated with increased risk of infection possibly due to protection afforded by high levels of PPEs and a decrease in infectivity that occurs in the later stages of illness although among critically ill patients.26,27 To the best of our knowledge, this study about the perceptions of HCPs and particularly doctors in Pakistan about risks and deaths associated with COVID-19 is the first survey conducted in Pakistan. Although this survey has a fair sample size, it represents only a small proportion of Pakistani HCPs and a selection bias cannot be excluded. The majority of the respondents 74.37% were residents of Khyber Pakhtunkhwa province and 68.40% were doctors among HCPs. This may in itself represent the worried group keen to voice their concerns. Furthermore, data were collected from those who had access to social media. Although our data were derived from HCPs in Pakistan, we believe it is also relevant to other countries with a diverse population of HCPs.
Conclusion
The study highlighted the worries of HCPs in Pakistan and the potential impact of such concerns. Such information can help in understanding the worries of HCPs and therefore designing and delivering interventions to address those worries. We believe the results of our work will be helpful in the development of policies and strategies related to the risk perception of COVID–19-related deaths in Pakistan as well as in other countries.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Before collecting data, the purpose of the study was explained and informed written consent was obtained from the study participants. Confidentiality of the subject’s information is assured. The ethical approval was taken from the Ethical review committee of the Khyber College of Dentistry Peshawar Pakistan.
ORCID iD
Farhad A. Khattak
References
1.
NguyenLHDrewDAGrahamMS, et al.Risk of COVID-19 among front-line health-care workers and the general community: A prospective cohort study. Lancet Public Heal. 2020;5(9):e475-83.
2.
ZhanMQinYXueXZhuS. Death from Covid-19 of 23 health care workers in China. N Engl J Med. 2020;382(23):2267-2268.
3.
WangDHuBHuC, et al.Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. J Am Med Assoc. 2020;323(11):1061-1069.
4.
BrooksSKDunnRAmlôtRRubinGJGreenbergN. A systematic, thematic review of social and occupational factors associated with psychological outcomes in healthcare employees during an infectious disease outbreak. J Occup Environ Med. 2018;60(3):248-257.
5.
KhuntiKSinghAKPareekMHanifW. Is ethnicity linked to incidence or outcomes of covid-19?BMJ. 2020;369:m1548.
6.
KursumovicELennaneSCookTM. Deaths in healthcare workers due to COVID‐19: The need for robust data and analysis. Anaesthesia. 2020;75(8):989-992.
7.
Covidgovpk. COVID-19 health advisory platform by ministry of national health services regulations and coordination dial 1166 health helpline CHAT BOT. Guidelines Prevention Facilities Public Service Message Home/Pakistan Cases Details Punjab COVID-19 Health Advisory [Internet. Lahore, Punjab: Covidgovpk; 2020:1-4.
8.
AliPAdamZWestJPareekMRazaMIqbalJ. Perceptions of COVID-19-related risk and mortality among ethnically diverse healthcare professionals in the UK. Ethn Health. 2021;26(1):1-10.
9.
ChongM-YWangW-CHsiehW-C, et al.Psychological impact of severe acute respiratory syndrome on health workers in a tertiary hospital. Br J Psychiatry. 2004;185(2):127-133.
10.
GouliaPMantasCDimitroulaDMantisDHyphantisT. General hospital staff worries, perceived sufficiency of information and associated psychological distress during the A/H1N1 influenza pandemic. BMC Infect Dis. 2010;10:322.
11.
LaiJMaSWangY, et al.Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open. 2020;3(3):e203976.
12.
ShaukatNAliDMRazzakJ. Physical and mental health impacts of COVID-19 on healthcare workers: A scoping review. Int J Emerg Med. 2020;13(1):40.
13.
GodderisLBooneABakusicJ. COVID-19: A new work-related disease threatening healthcare workers. Occup Med (Chic Ill). 2020;70(5):315-316.
14.
ZhuNZhangDWangW, et al.A novel coronavirus from patients with pneumonia in China, 2019. N Engl J Med. 2020;382(8):727.
15.
WoodEKingRSenekM, et al.UK advanced practice nurses’ experiences of the COVID-19 pandemic: A mixed-methods cross-sectional study. BMJ Open. 2021;11(3):e044139.
16.
IacobucciG. Covid-19: Doctors still at “considerable risk” from lack of PPE, BMA warns. BMJ. 2020;368:m1316.
17.
ThomasJPSrinivasanAWickramarachchiCSDhesiPKHungYMKamathAV. Evaluating the national PPE guidance for NHS healthcare workers during the COVID-19 pandemic. Clin Med. 2020;20(3):242-247.
18.
RanneyMLGriffethVJhaAK. Critical supply shortages — the need for ventilators and personal protective equipment during the Covid-19 pandemic. N Engl J Med. 2020;382(18):e41.
19.
AminFSharifSSaeedRDurraniNJilaniD. COVID-19 pandemic- knowledge, perception, anxiety and depression among frontline doctors of Pakistan. BMC Psychiatr. 2020;20(1):459.
20.
HakimMKhattakFAMuhammadS, et al.Access and use experience of personal protective equipment among frontline healthcare workers in Pakistan during the COVID-19 emergency: A cross-sectional study. Heal Secur. 2020;19(2):140-149.
21.
MahmoodQKJafreeSRJalilANadirSMHFischerF. Anxiety amongst physicians during COVID-19: Cross-sectional study in Pakistan. BMC Publ Health. 2021;21(1):118.
22.
MrklasKShalabyRHrabokM, et al.Prevalence of perceived stress, anxiety, depression, and obsessive-compulsive symptoms in health care workers and other workers in Alberta during the COVID-19 pandemic: Cross-sectional survey. JMIR Ment Heal. 2020;7(9):e22408.
23.
CroxsonCHDAshdownHFHobbsFDR. GPs’ perceptions of workload in England: A qualitative interview study. Br J Gen Pract. 2017;67(655):e138-e147.
24.
AbayomiAOsibogunAKanma-OkaforO, et al.Morbidity and mortality outcomes of COVID-19 patients with and without hypertension in Lagos, Nigeria: A retrospective cohort study. Glob Heal Res Policy. 2021;6(1):26.
25.
EjazHAlsrhaniAZafarA, et al.COVID-19 and comorbidities: Deleterious impact on infected patients. J Infect Public Health. 2020;13(12):1833-1839.
26.
KarlssonUFraenkelC-J. Covid-19: Risks to healthcare workers and their families. BMJ. 2020;371:m3944.
27.
van KampenJJAvan de VijverDAMCFraaijPLA, et al.Duration and key determinants of infectious virus shedding in hospitalized patients with coronavirus disease-2019 (COVID-19). Nat Commun. 2021;12: 267. https://doi.org/10.1038/s41467-020-20568-4.