
Abstract
Population aging is an economic and social challenge in most countries in the world as it generates higher dependency rates and increased demand for long-term care. Undertaking the care of older dependent adults can result in new opportunities for job creation. There is limited knowledge of the impact of dependent care and long-term care on employment. We examined this impact through a systematic review. Countries with conditional cash benefits show job creation, and countries with unconditional economic benefits reveal the development of a grey care market with high participation of migrant labor. Migrant employment in developed countries affects the development of the labor market in the countries of origin. The employment created to care for dependent persons is generally precarious. In conclusion, global aging will increase long-term care worker demand, but the variations in policies can determine what kind of employment is created.
Introduction
Global population aging is a challenge for welfare states, especially for long-term care systems (LTC). Since aging will significantly increase the absolute number of older people who are care dependent, demand for care and care cost will increase in the next decades.1,2 The world of work is also changing because of aging, among other factors, 3 and it is necessary to readjust the workforce to meet the needs of dependent people.
Developed countries have elaborated different measures and policies to satisfy growing care needs and to contain social and economic care costs. There are different ways to cluster countries based on LTC systems. On the one hand, focusing on the European welfare state classification—suitable for all developed countries, there are 3 care regimes. 4 First, the social democratic care regime provides universal access to care services for all people in need. Second, the liberal care regime is characterized by a developed care market in which services are purchased and the state provides care for people without resources and funds, outsourcing services. Third, the familistic care regime relies on family as caregivers for dependent relatives, with the state providing care in their absence. Countries adopt these three models to differing degrees. In other words, no country can be defined as practicing a purely social democratic, liberal, or family regime. On the other hand, focusing on public long-term care coverage for personal care, there are three broad country clusters: universal coverage within a single program, mixed systems, and means-tested safety-net schemes. 1 This classification is based on two criteria: the scope of entitlement to long-term care benefits and whether LTC coverage is through a single system or multiple benefits, services, and programs. Other classifications rely on characteristics related to governance and financing, supply of formal care services, cash benefits for the care of dependent persons, and the role of informal care or marketization of LTC. 5 However, despite the differences among LTC systems, countries are changing or developing their LTC systems in a similar direction: the search for consumer choice, moving away from residential care towards home care and community care, flexibility, financial sustainability and improving access to, and affordability of, care.1,5
Demographic changes imply a greater pressure on health and social public expenditure,6,7 but caring for dependent people can generate new employment opportunities. The demand for formal care is increasing as a result of aging societies, higher care dependency ratios, and changing family structures—increase in the number of single households, and the growing participation of women in the labor market.5,8 Projections on labor market evolution show that long-term care workers demand will increase in the decades to come. 9 According to the International Labor Organization (ILO), the employment needs are estimated at 4.2 formal long-term care workers per 100 individuals aged 65 years or above. 8 The employment created in this sector may not have similar working conditions in all countries; quantity and quality of job will depend on the policies applied. It is important to ensure good working conditions in LTC employment to create an attractive professional environment in the sector 10 and then improve care quality. The attractiveness of the formal care sector to potential workers is often undermined by negative perceptions related to poor working conditions, stressful working environments, lack of clearly defined career paths and lack of development opportunities, and quality of care is vital to maintaining and improving the quality of life of the elderly. 5
The literature has studied the LTC sector from different perspectives. Some studies have examined the implications of informal care for the job market11,12 and female supply,13-15 and others have studied whether employment affects informal care choice.16,17 Other works have examined the opportunity cost of informal care or caregiving in general,18-20 the features of LTC systems in different countries,21-23 or how to make care systems efficient, equitable and sustainable. 24
There is little evidence on the dynamics of the LTC workforce and consequences associated with aging and dependence in different care models. Thus, the aim of this paper is to analyze the impact of long-term care on employment creation in the care sector.
Method
This systematic review followed the guidelines of the PRISMA statement for reporting systematic reviews and meta-analyses. 25 A narrative synthesis to present the results has been used. 26 The graph was constructed using Gephi software. 27
The study used the definition of dependence provided by the Recommendation of the Committee of Ministers of the Council of the European Communities in 1998. 28 The Recommendation considered dependence as a state in which persons, because of lack or loss of physical, psychological, or intellectual autonomy, require significant assistance or help in carrying out their usual day-to-day activities.
Data Sources and Searches
Search Strategy.

Study Selection
Articles meeting the following requirements were included: (1) they were published in English; (2) they were an original article; and (3) they were focused on employment or long-term care.
Articles were excluded if: (i) they focused on informal care; (ii) they provided no information about labor force or markets, or workforce or employment in care sector; (iii) they focused on caregiving intensity or probability of being employed; and (iv) they focused on gender-related topics. Study design and empirical approach were not exclusion criteria. Given the wide variety of studies on dependence, it was necessary to take into account the results of the studies regardless of their design or empirical approach.
Quality of the Manuscripts
Methodological quality was assessed using three critical appraisal tools. One tool was used for the evaluation of cross-sectional studies, 29 the second was used for the evaluation of qualitative research, 30 and the third was used for the evaluation of mixed research (both quantitative and qualitative). 31 Two researchers (IP and RM) independently used the measurement tool. The checklists work with a different number of questions. Each component scores one point if the answer is “yes” or zero if the answer is “no,” “unclear,” or “not applicable/could nottell.” The cross-sectional study checklist comprises 8 questions, the qualitative research checklist consists of 10 questions, and the mixed research checklist has 13 questions. Any differences in the quality assessment of a particular study were resolved by consensus.
Data Extraction
The study selection and data extraction process comprised two phases. First, two researchers (IP and RM) screened all the records to eliminate any duplicates. Both researchers then independently reviewed the titles and abstracts of the 2217 records obtained. Finally, they selected the articles to be fully reviewed. The results were compared, and a third researcher (FE) was consulted to resolve any discrepancies in the inclusion criteria and so reach a consensus agreement.
Second, the two researchers (IP and RM) read all the articles obtained following the application of the inclusion and exclusion criteria. A full-text review of 55 articles was conducted. Of these, 41 were discarded by applying the exclusion criteria. The references of the 14 articles accepted were reviewed in case any relevant study had not appeared in the search process. The researchers found 4 studies in the secondary search. A total of 18 articles were finally included in the review.
Results
Brief Description of Included Articles
Given the wide range of topics involved in dependence, care, and employment, a narrative synthesis of the full-text articles was undertaken.
The selection process identified 2929 articles. After eliminating duplicates, 2217 remained. Only 18 met the inclusion and exclusion criteria—primary and secondary search. The flow diagram for the search procedure and study selection is shown below (Figure 1). Flow diagram.
Eleven of the studies included have a quantitative, observational, descriptive, and analytical design.23,32-41 The studies refer to the following countries or regions, in alphabetical order, Australia, Austria, Canada, Europe, France, Germany, Greece, Ireland, Italy, Japan, Korea, Luxembourg, Netherlands, Norway, Portugal, Sweden, United Kingdom, and United States of America. On various occasions, Spain, Greece, Italy, and Portugal are grouped together as southern European or Mediterranean countries.32,41,42
Six studies employ a mixed methodology, including quantitative information drawn from observational studies and qualitative information using different methodological tools in Austria, England, France, Germany, Ireland, Italy, the Netherlands, Norway, Spain, Sweden, Taiwan, and United Kingdom.42-47 One of these studies includes empirical research conducted using descriptive techniques and also based on the results of qualitative research comprising semi-structured recorded interviews, informal recorded interviews, unrecorded informal interviews, and non-participant observation of employees, employers, and care agencies in Madrid, London, and Stockholm. 47
One work 48 utilizes qualitative methodology and studies how migrant controls compromise migrant care workers’ exercise of choice and control over their employment, analyzing the findings of 56 in-depth interviews with migrant care workers from the United Kingdom. 49
Descriptive Summary of Included Studies (n = 18).

Narrative Synthesis of Results
The world population is aging and the need for care services has increased,37,42 while the LTC labor demand33,34,38 and the social and economic costs of care have risen. 41 Meanwhile, the need for elderly care services has increased, but the share of the population that is of working-age and can potentially provide these services is decreasing.35,38,42
Our review shows that in the US and EU, the care sector is characterized by low wages and bad working conditions.34,36,37,41,46,48 One study on the EU showed that outsourcing of services has encouraged the deterioration of working conditions. 47 Another work on Mediterranean countries added that the care service market is especially poorly regulated and the working conditions are considerably different from those of other markets. 32
These changes generated by aging have favored the reform or development of LTC systems.32,36,37,40,41,48 These reforms or developments, despite being applied in different countries, share certain characteristics: (i) intention of creating a care market,32,36,37,40,45,48 (ii) fostering user empowerment, giving individuals the capacity to choose between services and cash benefits—for example, cash benefit schemes allow families a “free choice” of care providers,36,37,40,41,47,48 (iii) promoting home care,36,37,40,41,48 or (iv) the promotion of cash benefits.23,36,37,39-41,47,48
In the US, EU, and other OECD countries, the introduction of cash benefits for the care of older adults has favored home care, affecting both the formal and informal care workforce—for example, attracting informal caregivers away from the formal labor market.37,39-41,47,48 In other words, cash benefits have promoted user empowerment, increasing the capacity to choose,36,37,40,41,47,48 and these benefits have encouraged the creation of a care market.36,37,40,41,48 The use of cash benefits was also used to contain care costs.23,37 However, promoting user choice not only affects users, but it can also have an impact on the care workforce,41,48 and payments for informal care can risk creating “incentive traps” that could attract informal caregivers away from the regular labor market. 39
This review has also found that care has been commodified.23,36,37,40-42,45,47,48 There are various points of view explaining the rise of commodification of care. First, the policy of cash benefits,36,37,48 and, second, the reliance on the private and not-for-profit sectors. 47 This latter perspective argues that this reliance has fueled the commodification of badly paid home care and that this commodification trend has accelerated the intervention of the private sector in the health and social care market, turning care provision into a large-scale international business, thus affecting care workforce conditions. Furthermore, a critical line on care system reforms states that, by separating funding from provision, the creation of a market has given rise to the commodification of care. 40 However, this critical line argues that what has actually happened is that this commodification has been accompanied by greater coverage and public regulation.
In addition, our results show that western EU welfare states are increasingly dependent on migrant labor to meet care needs and cover the demand for native labor.23,32,34,35,42,48 Migrant care workers are helping to contain the social and economic costs of care37,48 and have also relieved many families of care tasks. However, they have also partly crowded out formal care services. 38
Our findings suggest various factors might explain the rise in the reliance on migrant care workers. First, the development of cash benefits, especially when the allowance is unconditional—as in Germany, Austria, and other southern European countries—has encouraged the use of migrant care workers—mainly women—hired in the grey market, for the provision of home care.37,40-42,44,48 It is worth noting that the migrant and gender gap is not only common in EU; in the US, the workforce in the domestic service and care sectors mainly comprises women, and, furthermore, migrant women. 34 Additionally, in Italy, although benefit payments have been conditioned to hiring regulated caregivers in order to reduce the size of the informal market, the prevalence of cash transfers in a poorly regulated labor market with an extensive informal economy has favored a large supply of unregulated, and often undocumented, migrant care workers. 41 If we focus on southern European countries, our results show that the traditional and family-based care model—or familistic, where the burden of care falls on the family, mainly the female members, is shifting to a “migrant-in-the-family” care model.32,41,44,47 On the other hand, the use of migrant labor for care services can be explained by the difficulty of hiring and retaining national caregivers, and migrant workers may be convenient employees because they are even more vulnerable and, as a consequence, willing to accept poor employment conditions and low pay. 42 For example, in Taiwan, occupational segregation was reported between local, foreign institutional, and foreign home caregivers, the latter being the cheapest, most obedient, and most adaptable product in the market. 43
As previously mentioned, user choice has not only affected users. In this situation, the capacity for choice should also be extended to the migrant care workforce, which is compromised by immigration controls; the need to work—they do not choose a job in the care sector, and they need it; and the possibility of employers’ reporting negatively to immigration authorities if their employees want to change jobs. 48
Our results also show that the development of the grey care market is due to three factors. 36 First, being cheap, it is a cost-effective solution for families, as indicated by several studies.32,36,40,41,43,47 Second, the migrant care workforce earns more than in their country of origin because agreements with families tend to include full board, as indicated in other studies.32,36,41 Third, the grey market has reduced the pressure on social service demand. 37
Moreover, another consequence of the use of migrant labor to meet care demand is a partial undermining of the development of a formal care market,32,36-38 while it has also encouraged the commodification of care. 40
Discussion
To the best of our knowledge, this systematic review is the first to offer a synthesis of the scientific evidence provided by the studies available on the impact of dependence and long-term care on employment in the care sector. The wide thematic variety and heterogeneity of the studies necessitated determining the causal chain connecting the topics addressed in the studies with the aim of the review. Figure 2 shows a conceptual map depicting the interrelation between the different topics analyzed in the studies. Conceptual framework.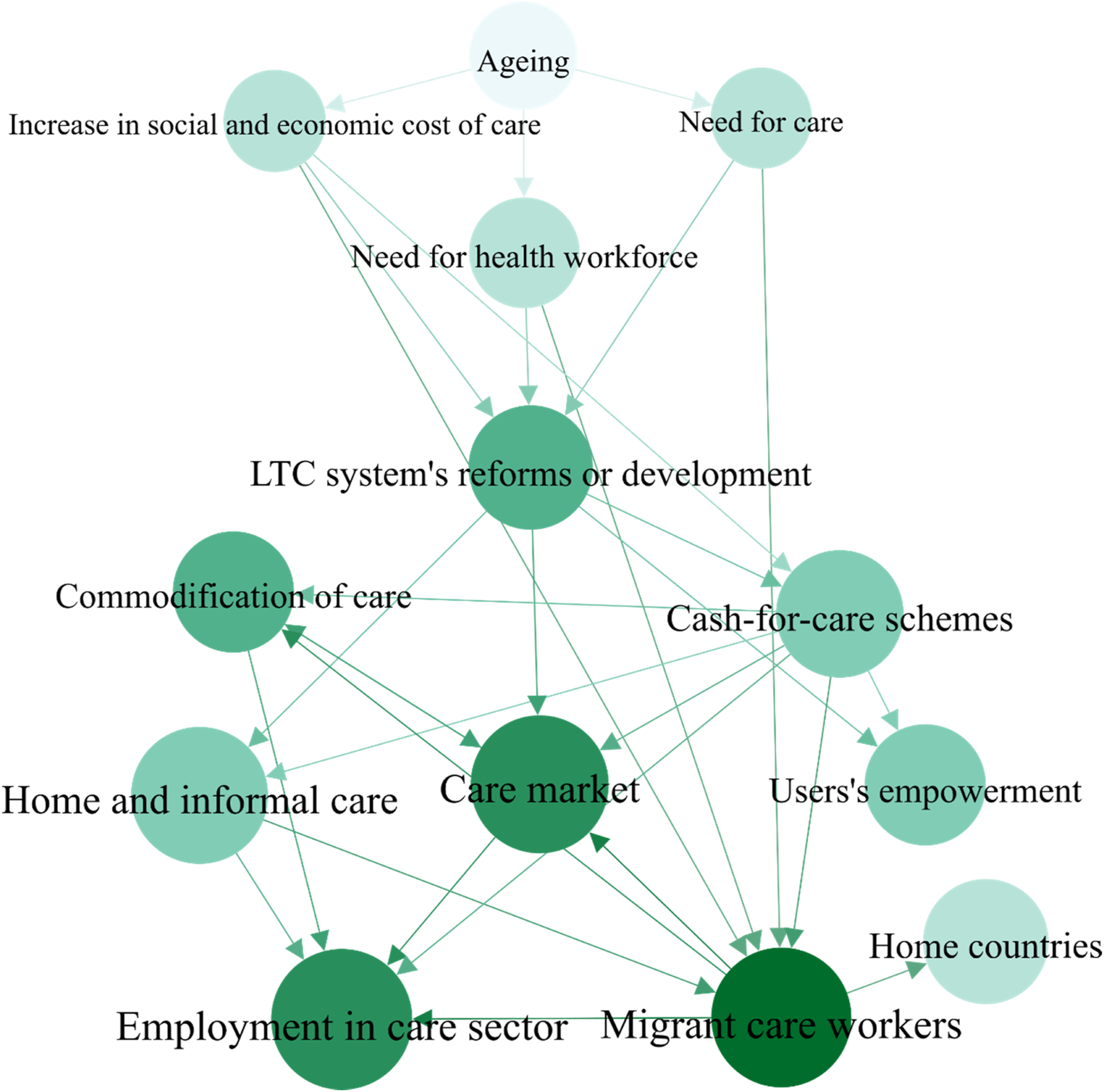
Due to global aging, LTC systems have had to be reformed, or developed wherever they were lacking, to confront the increase in demand for care, the need for labor, and the costs associated with care. Based on long-term care worker projections, the paid long-term workforce would need to grow to avoid serious future labor shortages.5,8,9 However, to date, the reforms proposed have encouraged the creation of a care market and the maintenance of home care, be it with formal or informal employment. The purpose of this was to contain care costs rather than to manage the labor care market.
One of the measures used is the introduction of cash benefits, the aim of which is to give families the financial power to choose how to spend the money, thus fostering competition in the sector. In countries where the cash benefit is conditioned to hiring personnel or services, formal employment has been created. However, as our results have shown, the main problem of this measure arises when the allowance is unconditional, that is, when proof of consumption is not required. In countries with an informal services market, families use this market due to the low cost and high flexibility of extensive migrant labor. 8 This has led to a crowding out of other, more costly alternatives. 32 Consequently, the first effect on employment in the care sector has been employment creation, albeit of poor quality, in countries with conditional cash allowances. The second effect, in countries with unconditional cash benefits and a grey economy, is dual in nature: an increase in the weight of migrant workers in the total provision of care and increased precariousness of labor in the care sector. However, the migrant care worker phenomenon is currently emerging in countries with well-developed formal services, as a result of cutbacks in the care sector. 50
The migrant care workforce, which is mainly women,23,51 has been a cheap and flexible solution for families. It has also enabled migrant care workers to earn more than they would in their own countries and has served to contain the pressure on the demand for caregivers.37,51 The long working hours to which migrant workers are exposed, together with the insecurity involved in immigrant status, undermines the ability of these caregivers to develop affective relationships with the people they care for. 48 Furthermore, female migrant care workers have been especially vulnerable to exploitative working conditions since domestic services are often paid under the table and in poor conditions.8,34 Consequently, the exploitation of migrant labor limits the quality of care as quality care is dependent on relationships of affection, not exploitation. 48 Thus, given the precarious situation in the care sector, the incorporation of migrant labor has not enhanced the pay and working conditions, but actually the contrary; the use of migrant labor has undermined the development of the formal care market.32,36,37 Furthermore, limiting the analysis of the effect of dependence and care on employment to a Eurocentric point of view significantly reduces the perspective of a global problem. Some countries of origin have specialized in “exporting” migrant care workers to specific destinations. 32 Remittances—money sent home—are a relatively stable source that often help to raise family income, may improve living conditions, and encourage economic development. 52 However, the migration of nurses, nursing assistants, and other long-term care workers has created a care deficit in the countries of origin. 34 In addition, this is important because the infrastructures in place in less developed countries are insufficient to meet this need. 2 The assignment of care to the private realm of the home, while generating job opportunities, however limited, for female migrants as domestic workers in developed countries, means they leave their own care responsibilities in the country of origin to their families. 48 In other words, while female migrant care workers serve as caregivers in richer countries, they create care needs which are covered by their partners, other relatives, or they may even use a domestic worker themselves—which at the same time is often an internal or an international migrant, and often another woman. 53 This phenomenon of a series of personal links between people across the globe, based on the paid or unpaid work of caring, is known as the “global care chain.8,54 Thus, in the target countries, employment in the domestic and care sector, albeit precarious, is being created, while in the countries of origin, the development of the job market is restricted since part of the active population is working in other countries.
The studies analyzed do not provide sufficient information to determine the limit of a care system in countries depending strongly and increasingly on migrant labor, with the exception of two studies suggesting that the sustainability of the system will depend on the time the countries of origin take to recover economically.32,34 Another perspective shows that large public investments in public services make the social care sector attractive for native employees and decreases the reliance on migrant care workers. 42 One interesting policy could be to protect migrant care workers by means of labor regulations, avoiding differences between native and foreign care workers. 43 Others policies to support caregivers could be to encourage leave from work, a flexible work schedule, or respite care, among others. 1 Hence, it is of great importance to ensure that both native and migrant care workers and care recipients have a decent life. In general, a large majority of long-term care workers feel that their work is useful, but many are not satisfied with their working conditions. 55
On other hand, better working conditions are necessary in order to guarantee the quality of care. As our review has shown, over the last few years, the commodification of care has favored growth in private service provision, which could create additional difficulties. As stated by the ILO, public provision of care services tends to improve the working conditions and pay of care workers, whereas unregulated private provision tends to worsen them, irrespective of the income level of the country. 8 Despite the many efforts to improve the quality of care—notably through accreditation systems and the constant refinement of standards—the quality of LTC still remains a problematic issue in European countries. 5
For this reason, it is necessary for LTC to be sustainable: it must be accessible, fair, and flexible. 24 This means that care policies must be designed with a mixture of freedom of choice of provider, state responsibility to provide care for families who are unable to obtain it themselves, and the development of an efficient private sector for those who wish to find another form of care. Care policies should consider different national contexts and the developmental stage of their care systems, and in this sense, from Southeast Asian countries to the US and EU, LTC systems are being reformed.55,56 Moreover, despite care systems being an expense, they can produce an economic return through the formalization of employment.
Limitations
This study has some limitations that need to be considered. The main limitation is a possible selection bias resulting from the databases consulted, the search strategy, and the exclusion of articles not published in English. Furthermore, despite having included grey literature, other similar studies or articles from non-indexed journals have likely not been detected. In addition, as the included studies are focused on specific regions, their findings are applicable to these regions. We added the tag “EU,” “US,” or other country/regional quotes to facilitate the reading and the interpretation. However, it must also be considered that the challenges, changes, and reforms in different long-term care national systems are frequently common. 55 Finally, the limitations and quality of the studies included could condition our conclusions. However, the main strength of this work is the use of a systematic and structured search methodology for the studies published, as well as a specific methodology for preparing the narrative synthesis.
Conclusions
This review shows that, due to global aging, LTC systems have had to be reformed, or developed wherever they were lacking, to confront the increase in demand for care, the need for long-term care workforce, and the costs associated with care. However, the main policies and reforms have encouraged the creation of a care market and the maintenance of home care, creating two kinds of employment. On the one hand, in countries with conditional cash allowances, formal employment has been created. On the other hand, in countries with unconditional cash allowances and an informal services market, there has been an increase in the weight of migrant workers in the total provision of care and increased precariousness of labor in the care sector.
The variations in policies may determine what kind of employment is created. Therefore, future care policies and reforms should address three main objectives. First, they must be designed with a mixture of freedom of provider choice, state responsibility to provide care for families in need, and the development of a private sector for those who want to find another kind of service. Second, they should take advantage of the economic return that formalization of employment can produce. Third, they must ensure that both native and migrant care workers and care recipients have decent living conditions.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been funded by the University of Castilla-La Mancha Research Group “Economy, Food, and Society.” (Project 2019- GRIN-27194.). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.