
Abstract
People with dementia who live in care homes often depend on care home staff for help with eating and drinking. It is essential that care home staff have the skills and support they need to provide good care at mealtimes. Good mealtime care may improve quality of life for residents, and reduce hospital admissions. The aim of this systematic review was to identify good practice in mealtime care for people with dementia living in care homes, by focusing on carer-resident interactions at mealtimes. Robust systematic review methods were followed. Seven databases were searched: AgeLine, BNI, CENTRAL, CINAHL, MEDLINE, PsycINFO and Web of Science. Titles, abstracts, and full texts were screened independently by two reviewers, and study quality was assessed with Joanna Briggs Institute tools. Narrative synthesis was used to analyse quantitative and qualitative evidence in parallel. Data were interrogated to identify thematic categories of carer-resident interaction. The synthesis process was undertaken by one reviewer, and discussed throughout with other reviewers for cross-checking. After title/abstract and full-text screening, 18 studies were included. Some studies assessed mealtime care interventions, others investigated factors contributing to oral intake, whilst others explored the mealtime experience. The synthesis identified four categories of carer-resident interaction important to mealtime care: Social connection, Tailored care, Empowering the resident, and Responding to food refusal. Each of the categories has echoes in related literature, and provides promising directions for future research. They merit further consideration, as new interventions are developed to improve mealtime care for this population.
Introduction
Dementia describes a set of symptoms including concentration and memory problems, changes in mood and behaviour and problems with communication and reasoning (Alzheimer’s Society, 2014). It is an increasingly prevalent condition; by 2025, there are expected to be one million people with dementia in the United Kingdom (Department of Health (UK), 2015).
Swallowing difficulties (dysphagia) may occur in people with dementia due to impaired physiology (such as a delayed swallow reflex) and/or due to behavioural issues (such as eating and drinking too quickly) (Alagiakrishnan et al., 2013). This can result in pulmonary aspiration (entry of food/drink into the larynx and lower respiratory tract), which in turn can lead directly to asphyxiation or pneumonia (Torres et al., 2013).
Mealtime difficulties in people with dementia are not limited to dysphagia; other problems at mealtimes are prevalent (Kai et al., 2015). These include difficulty recognising food and drink (Amella, 2002), problems using cutlery (Social Care Institute for Excellence, 2015) and changes in appetite and preferences (Ikeda et al., 2002). Such difficulties have potentially serious consequences. Inadequate oral intake may result in undernutrition and dehydration and therefore reduced quality of life, more frequent hospital admissions and increased risk of morbidity and mortality (Abbott et al., 2013).
In addition, eating and drinking are fundamental human activities, with significant social and emotional associations (Brush & Calkins, 2008; Burges Watson et al., 2018). The psychosocial aspect of mealtimes is important and may impact on food intake and quality of life (Fetherstonhaugh et al., 2019; Keller, 2016). Difficulties at mealtimes can lead to anxiety, depression and isolation (Ney et al., 2009). For all these reasons, mealtime difficulties can be distressing for people with dementia and for those who provide their care (Pasman et al., 2003).
Mealtime difficulties are particularly prevalent among people with dementia in long-term care settings (Prince et al., 2014). In the United Kingdom, United States and Australia, it has been estimated that more than half of all care home residents have dementia (Alzheimer’s Society, 2014; Australian Institute of Health and Welfare, 2012; Harris-Kojetin et al., 2016). In care homes, it is staff who provide personal care to people with dementia – including at mealtimes. Typically, this is staff in a carer role (whether named as carer, care assistant, certified nursing assistant, auxiliary, care aide, and so on, depending on country). Qualified nursing staff may also provide this personal care at mealtimes. Through their interaction with residents, care home staff are responsible for facilitating oral intake which is safe, adequate and enjoyable (Health Education England, 2015). They may do this by providing physical assistance with eating/drinking (Abdelhamid et al., 2016; Mann et al., 2019). They may also do this through prompting and supervision at mealtimes and responding to signs of dysphagia to minimise risk of aspiration. For the purposes of this study, we will refer to all activity of this kind as ‘mealtime care’.
Good mealtime care for people with dementia living in care homes can improve their quality of life (Evans et al., 2009), provide greater reassurance for their families (Alzheimer’s Society, 2013; Hanson et al., 2013) and may reduce hospital admissions (Richardson, 2015). However, evidence has shown that the quality of mealtime care for this population is variable (Aselage et al., 2011). The aim of this systematic review is to identify good practice in mealtime care for people with dementia living in care homes, by focusing on carer–resident interactions at mealtimes.
Methods
Registration of the review
The protocol for this review was registered on PROSPERO (CRD42018114533).
Eligibility criteria
The following eligibility criteria were used for study selection: The population was people with dementia living in care homes. Dementia could be of any type and stage. If a study included participants with various clinical diagnoses, it was necessary for the majority of participants to have dementia and for data on those participants to be presented separately from those with other diagnoses. The phenomenon of interest was mealtime care. Mealtime care was defined as ‘interactions occurring between care staff and residents at mealtimes, which may promote safe, adequate and/or enjoyable oral intake’. Activities outside of the direct control of care staff were excluded (e.g. recommendation of percutaneous endoscopic gastrostomy tube, oral nutritional supplements and specialist training programmes targeted at people with dementia, such as Montessori, and spaced retrieval therapy). Studies focusing on assessment of mealtime difficulties were also excluded. The publication types were peer-reviewed primary studies of any research design (quantitative, qualitative or mixed methods). For practical reasons, sources unavailable in English were excluded from the review. There was no limitation on the date of studies, to capture as many studies as possible which met the eligibility criteria.
Search strategy
Seven databases were chosen to provide comprehensive and relevant multidisciplinary coverage: AgeLine, BNI, CENTRAL, CINAHL, MEDLINE, PsycINFO and Web of Science. Search strings suitable for each database were devised; these comprised the categories ‘dementia’, ‘mealtimes’ and ‘care’ and used both free-text and index terms. Thesaurus headings were translated as appropriate between databases. An example search strategy, for MEDLINE, is presented in Supplemental Appendix A. Databases were searched from inception to May 2020.
Results were downloaded into EndNote©. Titles and abstracts of retrieved studies were screened independently by two reviewers, using the online tool Rayyan (http://rayyan.qcri.org). Any discrepancies were resolved via discussion. Full texts of remaining studies were then screened independently by two reviewers. Again, discrepancies were resolved via discussion, with recourse to a third reviewer as needed. Reasons for exclusion were noted.
In addition to the database search, studies were sought by other means. Relevant non-indexed journals were hand-searched, from inception to present. These were the Journal of Nursing Home Research, the Journal of Aging and Long-Term Care and the Journal of Long-Term Care. Reference lists of related systematic reviews were searched. Experts in the field were contacted for recommendations.
Data extraction
Separate data extraction forms were designed for quantitative and qualitative studies, with fields chosen to capture all necessary information. Data were extracted on study characteristics, outcomes and results. For qualitative studies, verbatim reports of findings were extracted. One reviewer carried out data extraction, and a second reviewer checked the data against the original papers to ensure there were no erroneous or missing data.
Critical appraisal
Peer-reviewed critical appraisal tools published by the Joanna Briggs Institute (JBI) were used to critically appraise the studies (Aromataris & Munn, 2017). The tools used were as follows: Checklist for Analytical Cross Sectional Studies, Checklist for Quasi-Experimental Studies, Checklist for Randomised Controlled Trials and Checklist for Qualitative Research. Two reviewers critically appraised all studies independently. Discrepancies were resolved via discussion, with recourse to a third reviewer as needed.
Data synthesis
A convergent synthesis design was used: quantitative and qualitative evidence was collected and analysed in parallel (Hong et al., 2017). Integration occurred at the level of the extracted data so that studies were analysed using the same synthesis method. The chosen method of analysis was Narrative Synthesis (Popay et al., 2006). In order to construct a common rubric for synthesis of quantitative and qualitative data, a textual summary of results was produced for each study. Verbatim extracts from the study reports were used, including principle findings. Data were interrogated to identify thematic categories of carer–resident interaction. Principles of constant comparative method were used (Glaser, 1965), which involved reading and re-reading data to search for emerging categories (Burnard et al., 2008). The synthesis process was undertaken by one reviewer, with regular discussion with other reviewers in order to cross-check the analysis.
Results
The initial database search retrieved 5729 articles. Reference management software was used to remove duplicates, leaving 3268 articles. Title/abstract screening resulted in 680 articles. Of these, 526 were excluded because they were ineligible due to language, availability, publication type or because of duplication undetected by the software. The remaining 154 articles were full-text screened, with 136 excluded at this stage (see Supplemental Appendix B for a full list of these articles and reasons for exclusion). This left 18 articles which reported eligible studies. Hand searches and other lines of enquiry did not yield any additional eligible studies (see Figure 1 for a PRISMA flow diagram summarising the study selection process) (Moher et al., 2009). PRISMA flow diagram of study selection process.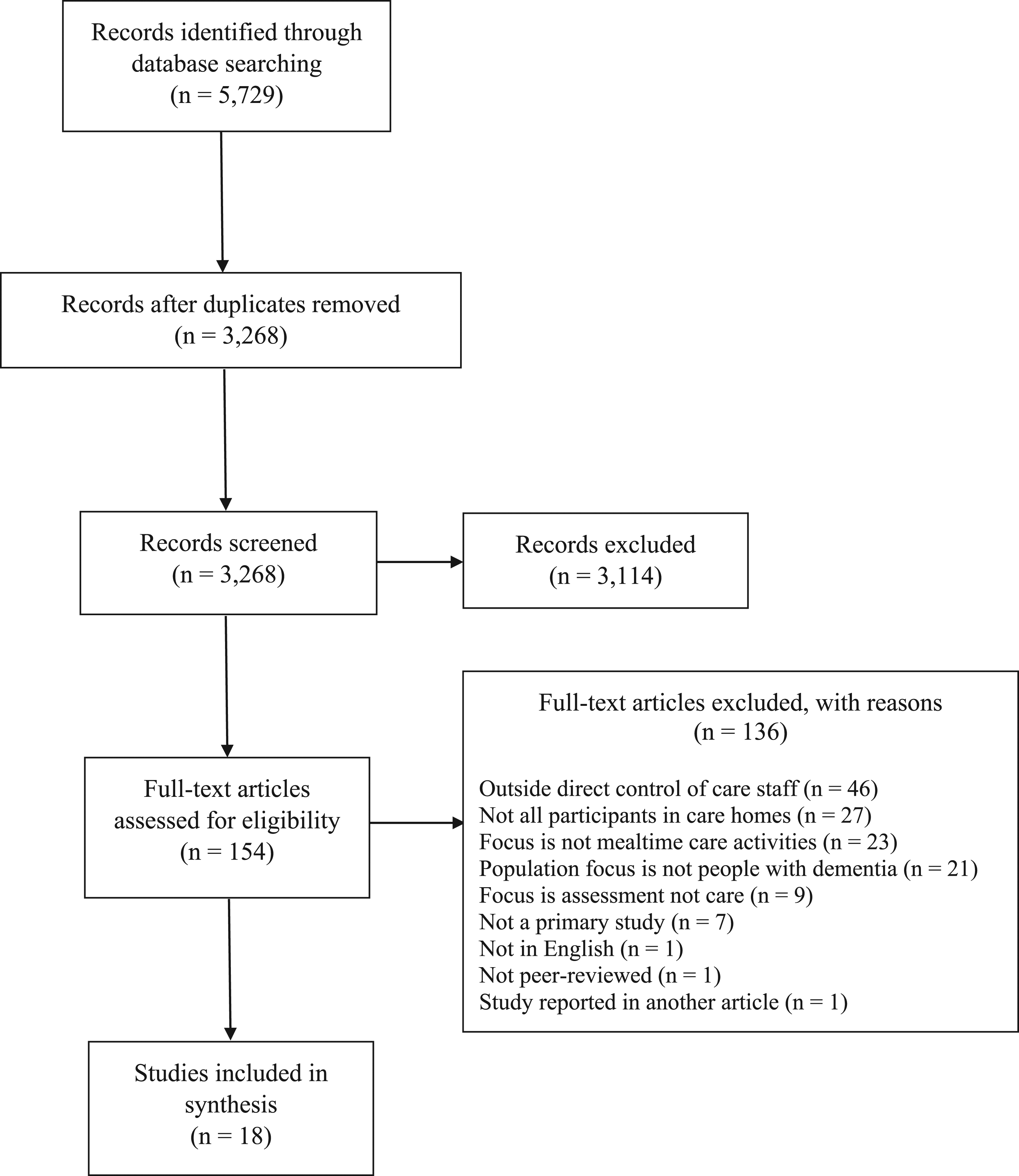
Study characteristics
Study characteristics.
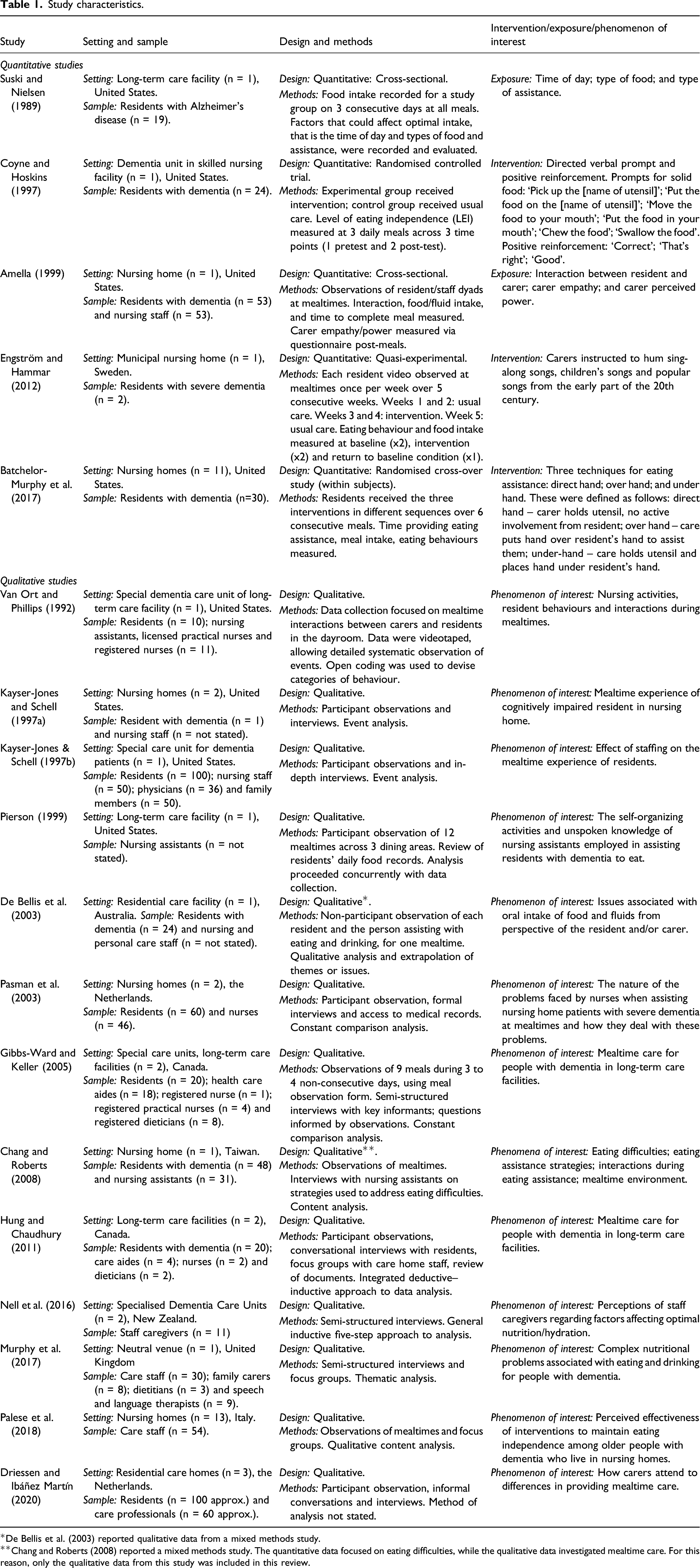
*De Bellis et al. (2003) reported qualitative data from a mixed methods study.
**Chang and Roberts (2008) reported a mixed methods study. The quantitative data focused on eating difficulties, while the qualitative data investigated mealtime care. For this reason, only the qualitative data from this study was included in this review.
The studies were varied in design. Two studies were randomised controlled trials (Batchelor-Murphy et al., 2017; Coyne & Hoskins, 1997); one was a quasi-experimental study (Engström & Hammar, 2012); two were cross-sectional studies (Amella, 1999; Suski & Nielsen, 1989). Eleven studies were qualitative. Of these, nine included observation of mealtimes in their data collection (Driessen & Ibáñez Martín, 2020; Gibbs-Ward & Keller, 2005; Hung & Chaudhury, 2011; Kayser-Jones & Schell, 1997a, 1997b; Palese et al., 2018; Pasman et al., 2003; Pierson, 1999; Van Ort & Phillips, 1992) and two used focus groups and/or interviews only (Murphy et al., 2017; Nell et al., 2016). Two studies used mixed methods: Chang and Roberts (2008) and De Bellis et al. (2003). Both of these conducted cross-sectional studies and collected qualitative data. De Bellis et al. (2003) reported only the qualitative data. In Chang and Roberts (2008), the quantitative data focused on residents’ eating difficulty, while the qualitative data investigated mealtime care – for this reason, only the qualitative data from this study were included here. Thus, these two studies are bracketed with the qualitative studies in the review.
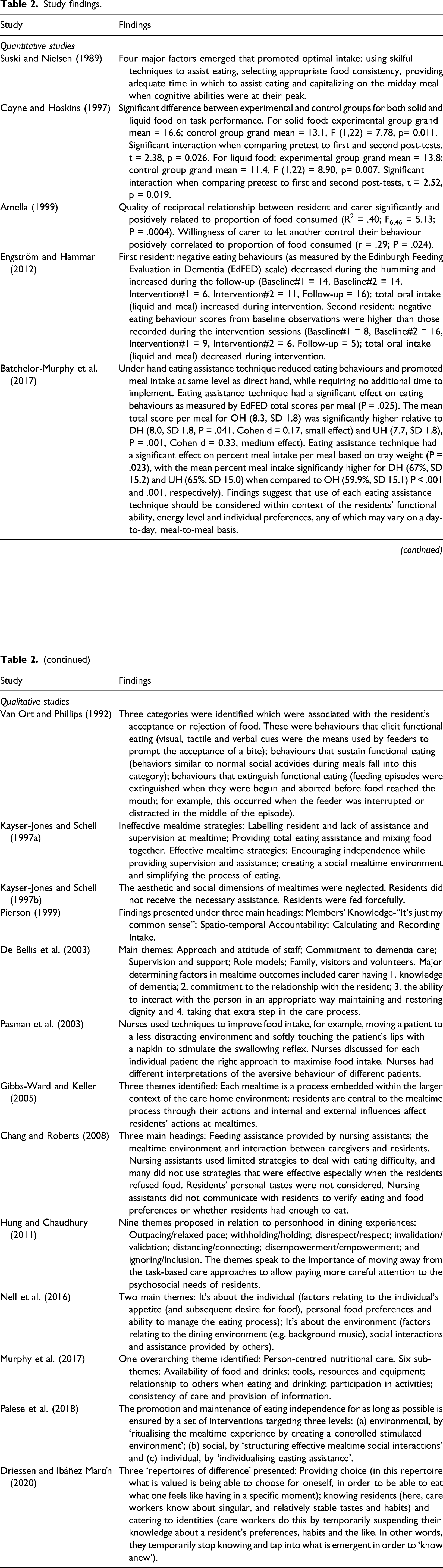
The three experimental/quasi-experimental studies assessed the effectiveness of a care staff intervention at mealtimes. Batchelor-Murphy et al. (2017) compared three techniques for eating assistance (direct hand, over hand and under hand), by using the Edinburgh Feeding Evaluation in Dementia scale to assess eating and eating assistance behaviours. Coyne and Hoskins (1997) assessed the efficacy of directed verbal prompts and positive reinforcement, using their own Level of Eating Independence scale. Engström and Hammar (2012) assessed the effect of carers humming during mealtimes, measuring the amount of food/liquid consumed in grams.
The two cross-sectional studies investigated the association between quantity of oral intake and possible influencing factors. Amella (1999) used weight to measure proportion of food consumed and assessed the influence on this of interaction between resident and carer, carer empathy and carers’ level of perceived power (these were measured using, respectively, the Interaction Behaviour Measure, the Interpersonal Reactivity Index and the Fundamental Interpersonal Relations Orientation – Behavior). Suski and Nielsen (1989) used researcher rating of proportion of meal consumed as the outcome measure, in considering the impact of time of day, type of food and technique for eating assistance.
The 13 studies reporting qualitative data explored mealtimes from various perspectives. De Bellis et al. (2003), Kayser-Jones and Schell (1997b), Nell et al. (2016), Palese et al. (2018), Pasman et al. (2003), and Pierson (1999) investigated care staff’s perceptions of, and approaches to, mealtime care. Gibbs-Ward and Keller (2005) and Murphy et al. (2017) used qualitative data to develop a conceptual understanding of mealtime care. Kayser-Jones and Schell (1997a) and Van Ort and Phillips (1992) described and analysed carer strategies to assist residents at mealtimes. Hung and Chaudhury (2011) explored the concept of personhood (see Kitwood, 1997) in the context of mealtimes, with particular reference to the influence of care staff activity. Chang and Roberts (2008) investigated mealtime difficulties, carer strategies and mealtime environment. Driessen and Ibáñez Martín (2020) considered how mealtime care is tailored to address differences in residents.
Study quality
Detailed results of the critical appraisal are presented in Supplementary Tables A (quantitative studies) and B (qualitative studies) with the online version of this article. The methodological quality of included studies was varied. The highest-scoring quantitative study (Batchelor-Murphy et al., 2017) was rated Yes for all applicable criteria, except for one criterion which was rated Unclear. The lowest-scoring quantitative study (Engström & Hammar, 2012) was rated No for three applicable criteria. The other quantitative studies were all rated No for one applicable criterion. The failed criteria were different in each case and included the following: ‘Were the outcomes measured in a valid and reliable way?’; ‘were confounding factors identified?’ and ‘were treatment groups similar at baseline?’ The highest-scoring qualitative study (Gibbs-Ward & Keller, 2005) met all criteria. The lowest-scoring qualitative study (Chang & Roberts, 2008) was rated No for three criteria and Unclear for six others. The other qualitative studies achieved a range of scores in between. The most common failed criterion amongst the qualitative studies was ‘is the influence of the researcher on the research, and vice versa, addressed?’ The impact of study quality on the review synthesis is discussed in more detail below.
Synthesis of study findings
Study findings.
Thematic categories of carer–resident interaction.
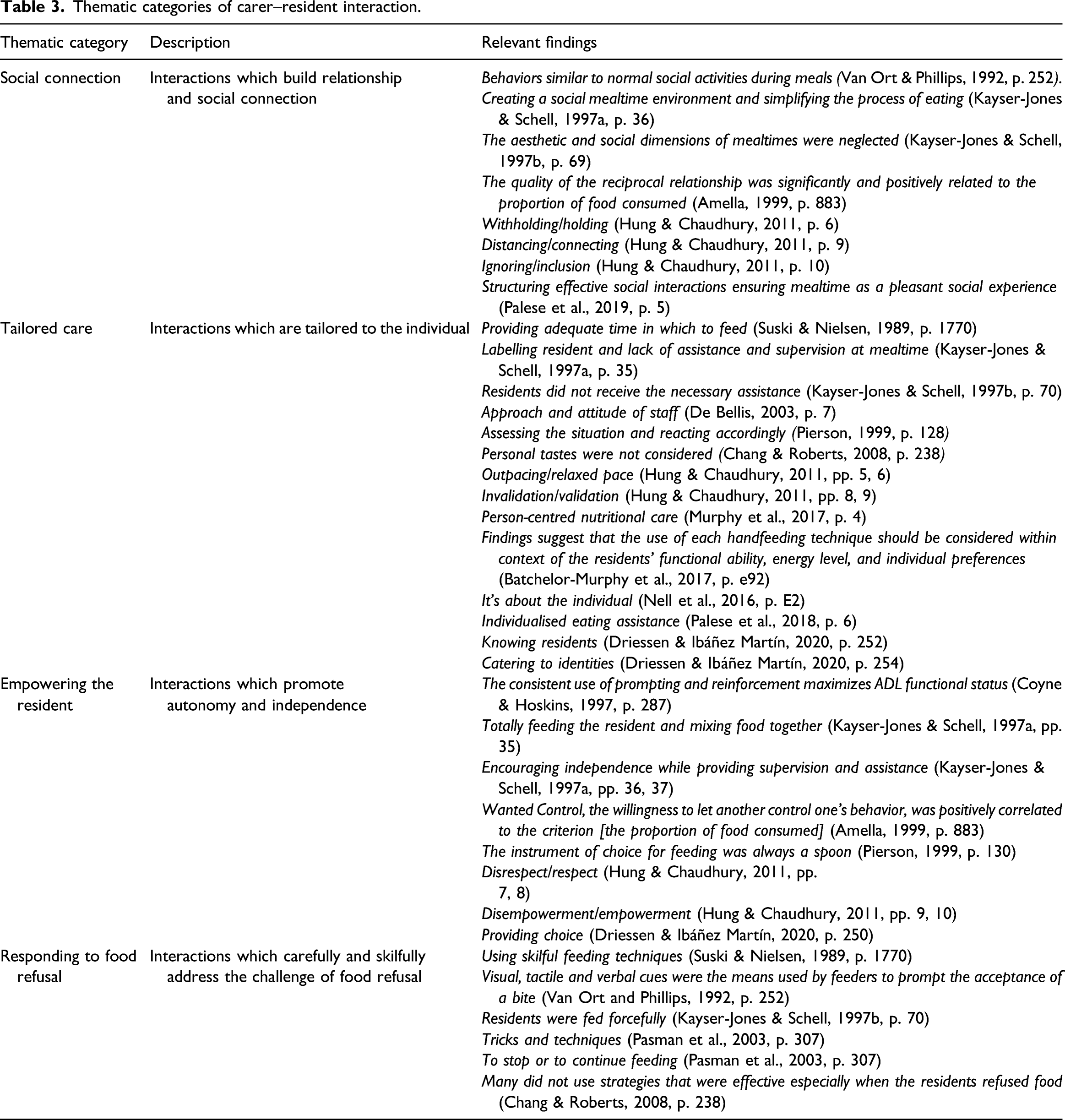
Social connection
Social connection refers to interactions which build relationship between carer and resident and which facilitate social connection at mealtimes. This sense of relationship and social connection featured in findings from six studies. Two studies identified the importance of carer–resident relationship (Amella, 1999; Hung & Chaudhury, 2011). Four studies found that social interactions were key at mealtimes (Kayser-Jones & Schell, 1997a, 1997b; Palese et al., 2018; Van Ort & Phillips, 1992).
Tailored care
Tailored care denotes interactions which are tailored to the individual. The idea of tailored care was represented in findings from 12 studies. Some studies emphasised tailoring the amount of direct assistance to suit the resident (Batchelor-Murphy et al., 2017; Kayser-Jones & Schell, 1997a, 1997b; Palese et al., 2018; Pierson et al., 1999). Other studies highlighted the importance of knowing residents’ preferences (Driessen & Ibáñez Martín, 2020; Murphy et al., 2017; Nell et al., 2016). Focusing on the individual resident – rather than the task – was identified in other studies (De Bellis, 2003; Hung & Chaudhury, 2011).
Empowering the resident
Empowering the resident is about interactions which promote the resident’s autonomy and independence. Empowerment in this way was represented in the findings of several studies. Encouragement of independent eating was advocated (Hung & Chaudhury, 2011; Kayser-Jones & Schell, 1997a). So too was ceding control to the resident in mealtime interactions (Amella, 1999; Batchelor-Murphy et al., 2017; Hung & Chaudhury, 2011). Provision of choice was a key theme in Driessen and Ibáñez Martín (2020). Pierson (1999) highlighted the problem of carers making decisions on residents’ behalf.
Responding to food refusal
Responding to food refusal is concerned with interactions which carefully and skilfully address the challenge of food refusal. Some studies promoted the use of skills and techniques in dealing with this challenge (Pasman et al., 2003; Suski & Nielsen, 1989; Van Ort & Phillips, 1992). The balance of encouraging oral intake without using force was also highlighted in studies (Kayser-Jones & Schell, 1997b; Pasman et al., 2003).
Engström and Hammar (2012) was included in the synthesis but did not contribute to the thematic categories. This study reported contradictory findings for the effects of carers humming during mealtimes. For one participant, oral intake was increased during the intervention, but for the other participant, it was reduced.
Discussion
This systematic review has investigated the published evidence on mealtime care for people with dementia living in care homes. It has taken an intentionally broad, inclusive approach to study selection, and as a consequence, the included studies are heterogeneous in design. The review has focused on ways in which care staff interact with residents whilst providing mealtime care. It has identified four thematic categories of interaction across the studies: Social connection, Tailored care, Empowering the resident and Responding to food refusal.
These findings may be informative for practitioners, researchers and policy makers seeking to optimise mealtime care for people with dementia living in care homes. Firstly, the findings point to social connection as an important part of mealtime care. Care home staff are able to foster social connection at mealtimes, not only through their own interactions with residents but also by facilitating interactions between residents. For some staff, this may be a very natural undertaking; for others, it may have to be more intentional. Interventions promoting social connection at mealtimes should be considered (Watkins et al., 2019), but these also need to take account of residents’ individual characteristics (Cherry et al., 2008). Secondly, the findings indicate that mealtime care should be tailored to the resident. This means knowing the resident’s needs and preferences and prioritising them during mealtimes – but also being receptive to the idea that they may change (Driessen & Ibáñez Martín, 2020). Thirdly, the findings say that good mealtime care helps residents to be empowered. This can happen when residents are given choice at mealtimes (e.g. whether this is choice of what to eat, where to eat and when to eat). It can also happen when care home staff allow residents to be in control at mealtimes – for example, to eat without assistance, even if this takes longer. Complexities may arise from this, particularly when a resident’s choice is perceived as unwise. An understanding of the Mental Capacity Act is likely important in this context (Manthorpe and Samsi, 2016a). Fourthly, the findings suggest that responding carefully and skilfully to food refusal is a significant element of mealtime care. Skilled care home staff may be able to respond in a way that encourages (but does not coerce) a resident to eat more. Further work is needed to find ways to articulate and delineate this skill so that it can be replicated (Liu et al., 2020).
In reporting review findings, it is important to consider strength of evidence, the context of other literature and review methods (Moher et al., 2009).
Strength of evidence
The strength of evidence for these thematic categories was varied. The category Social connection was supported by six studies. Some of these had significant shortcomings in their design or reporting. For example, the qualitative studies by De Bellis et al., (2003) and Kayser-Jones and Schell (1997a, 1997b) provided only brief or minimal illustrations from data to show the basis of their conclusions. By contrast, both Hung and Chaudhury (2011) and Palese et al. (2018) used plentiful direct quotes and data extracts to support their themes.
The concept of Tailored care was supported by 12 studies, easily the most of all the categories. Again, however, the quality of evidence was mixed. There was variation, for example, in the reliability of outcome measures used in the quantitative studies. Some measures of oral intake were precise and objective (Batchelor-Murphy et al., 2017), while others had greater risk of unreliability (Suski and Nielsen, 1989). There was also variation in the extent to which qualitative studies reported a congruent philosophical perspective and research methodology. Some studies clearly articulated a link between the two (De Bellis et al., 2003; Hung & Chaudhury, 2011; Pierson, 1999), while others did not (Chang & Roberts, 2008; Driessen & Ibáñez Martín, 2020; Kayser-Jones & Schell, 1997a, 1997b; Nell et al., 2016; Murphy et al., 2017; Palese et al., 2018).
Evidence for Empowering the resident, provided by six of the included studies, was also varied in quality. One quantitative study (Amella, 1999) met all criteria except identification of confounding factors. The other (Coyne & Hoskins, 1997) missed three criteria, partly due to lack of clarity in reporting. The qualitative studies (Driessen & Ibáñez Martín, 2020; Hung & Chaudhury, 2011; Kayser-Jones & Schell, 1997a; Pierson, 1999) were each marked down on more than one criterion – for example, none addressed influence of the researcher on the research and vice versa.
Responding to food refusal was supported by the lowest number of studies: five. Several of these scored poorly in quality appraisal. Two achieved half of the available criteria. Kayser-Jones and Schell (1997b), a qualitative study, was unclear on philosophical perspective, data analysis and ethical approval – and did not adequately represent participants’ voices. Suski and Nielsen (1989), a quantitative study, was unclear on how the condition was measured and on how to deal with confounding factors – and did not measure outcomes in a reliable way. A third study – Chang and Roberts (2008) – achieved only one criterion, pertaining to the connection between data and conclusions. For six other criteria, this study was rated Unclear.
Comparison to other literature
The thematic categories generated by this review are for the most part echoed in other related literature – for example, broader mealtime care literature and dementia care literature. A number of recent studies have pointed to the importance of social interactions at mealtimes in long-term care (Chaudhury et al., 2017; Keller et al., 2018; Watkins et al., 2017). Also, current guidance has emphasised the value of social relationships and interactions more broadly for people living with dementia (Alzheimer’s Society, 2019; National Institute for Health and Care Excellence (UK), 2018). In dementia care and more widely, relationships and interactions are considered central to quality care (see, e.g. relationship-centred care (Nolan et al., 2004; Tresolini et al., 1994)).
Similarly, the idea of tailoring care to the individual resident is prevalent both in broader mealtime care literature (Reimer & Keller, 2009; Slaughter et al., 2020; Wu et al., 2018) and in dementia care literature (Fazio et al, 2018; Manthorpe and Samsi, 2016b). This concept also features prominently in guidance and regulation in this area (Care Quality Commission, 2014; Social Care Institute for Excellence, 2020).
The importance of empowering the resident is a common theme in previous work on general mealtime care. Several studies have emphasised the need for interventions which maximise independence and autonomy at mealtimes (Iuglio et al., 2018; Mann et al., 2019; Palese et al., 2019; Reimer & Keller, 2009). The topic also features in studies which explore dementia care more broadly (Boumans et al., 2019; McCormack, 2001) and in various published guidelines for dementia care (Alzheimer’s Association, 2009; Irish Nutrition and Dietetics Institute, 2016).
The way that carers respond to food refusal is less prevalent than the other categories in recent studies on mealtime care (although it is found in some older literature, particularly from Scandinavia (see Athlin & Norberg, 1987; Jansson et al., 1995) and in published guidance (Caroline Walker Trust, 1998)). At a broader level, the idea of refusal of/resistance to a care act of some kind – and the way in which staff respond to this challenge – is well documented in the dementia care literature. There are examples in the context of medication (Haskins & Wick, 2017; Young & Unger, 2016), oral hygiene (Jablonski, et al., 2011) and general care (Konno, et al., 2012; Mahoney et al., 1999). It is not clear why there is a relative absence of this theme in mealtime care literature. Perhaps it is taken for granted (and therefore sometimes unstated) that mealtime care includes response to food refusal. New research in this area may be beneficial, to better understand the challenges of food refusal, and optimal ways to respond.
Strengths and limitations of the review
As well as considering the strength of evidence provided by included studies – and the relationship between these studies and other literature – it is important to evaluate the robustness of methods used in the review.
The review has included heterogeneous study designs. This decision was taken in order to maximise findings and the ability of those findings to inform policy and practice (Harden, 2010); an appropriate strategy to address the complexity of healthcare research questions (Bressan et al., 2017). By synthesising data from a variety of sources, the review has been able to identify broad categories of the carer–resident interaction in mealtime care. It does not, however, provide an estimate of the effectiveness of a current intervention (or type of intervention). Instead, it is intended to identify relevant principles which may help with intervention development and thus improve practice.
In keeping with this inclusive approach, the decision was taken to accept for synthesis all studies meeting the eligibility criteria for the review; that is, there was no cut-off score for quality. Instead, quality assessment was used to gain an understanding of the strength of the evidence and taken into account during the process of synthesis (Centre for Reviews and Dissemination, 2008, p. 227). There is a range of quality within the groups of studies supporting each thematic category in the synthesis, and for each category, the methodological strengths and weaknesses are reported narratively. It is therefore possible to draw only provisional conclusions about the thematic categories, and further robust evidence is needed because of the mixed quality of included studies.
As well as taking into account methodological quality as assessed by the JBI critical appraisal tools, it is worth noting studies with findings that were problematic in other ways. Engström and Hammar (2012), as previously mentioned, reported contradictory findings for their intervention. Van Ort and Phillips (1992), in attempting to develop categories of caregiver and resident behaviour, found ‘mutually exclusive categories were difficult to distinguish’ (p. 253). Pierson (1999) sought to describe the work of carers providing mealtime care but decided this an almost impossible task since it comprises embodied practices and unspoken knowledge. Chang and Roberts (2008) organised their findings under broad descriptive headings rather than discrete themes, which meant the findings were not easily amenable to the synthesis process. Coyne and Hoskins (1997) trialled their mealtime care intervention in a somewhat different way to other studies: it was intended to increase independence of residents at subsequent mealtimes, not the current mealtime.
A qualitative approach has been used in the review synthesis. Following Popay et al. (2006), it was necessary to use a common rubric for synthesis of quantitative and qualitative data, and in this case, a textual summary of results was produced for each study. There is the potential for reviewer bias in this method, but this was mitigated by using only verbatim descriptions of explicit study findings and themes whilst developing the synthesis and through regular discussion of emerging thematic categories by the review team.
The decision was made to specify people with dementia as the population of interest, rather than care home residents more generally. It is possible therefore that some studies have been excluded with useful findings on the broader topic of mealtimes in care homes. However, the particular nature of the challenges faced by people with dementia at mealtimes – and their carers – has motivated the authors to focus their research on this population.
Finally, the review has focused on carer–resident interaction at mealtimes. This focus has allowed for detailed analysis of this aspect of mealtime care as it is reported in the literature. At the same time, it must be acknowledged that there are other, organisational, factors which may impact on the way people with dementia experience mealtimes – for example, physical environment, food service and menu provision. These factors are not explored here because they have been covered in previous reviews (Abdelhamid et al., 2016; Bunn et al., 2016; Herke et al., 2018; Jackson et al., 2011; Liu et al., 2015). Nevertheless, it would be essential to consider such organisational factors in future intervention studies on this topic. Carer–resident interactions are, after all, influenced by care home environment, staffing ratios, company policies, staff training and many other things outside the immediate control of the care staff themselves. Complex interventions literature is a useful reference point here, to help researchers take account of systems and context (see O'Cathain et al., 2019; Hawe et al., 2009; May & Finch, 2009).
Conclusion
This evidence synthesis has brought together a diverse body of data on the topic of mealtime care for people with dementia who live in care homes. It has focused on carer–resident interaction at mealtimes. Notwithstanding the aforementioned limitations, the findings indicate that good mealtime care may involve interactions which facilitate social connection, which are tailored to individual residents, which empower residents to promote autonomy and independence and which carefully and skilfully respond to the challenge of food refusal. Given the variable quality of evidence, it is not possible to make definitive practice recommendations here. Nevertheless, each of the identified thematic categories has echoes in related literature and provides promising directions for future research. They merit further consideration as new interventions are developed to improve mealtime care for this population.
Supplemental Material
sj-pdf-1-dem-10.1177_14713012211002041 – Supplemental Material for How do we provide good mealtime care for people with dementia living in care homes? A systematic review of carer–resident interactions
Supplemental Material, sj-pdf-1-dem-10.1177_14713012211002041 for How do we provide good mealtime care for people with dementia living in care homes? A systematic review of carer–resident interactions by James Faraday, Clare Abley, Fiona Beyer, Catherine Exley, Paula Moynihan and Joanne M Patterson in Dementia
Footnotes
Acknowledgements
The authors would like to thank Anne Barrett, Claire Marcroft, Ananya Namdeo, Kim Pearce and Laura Prato for their contributions to this systematic review.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: James Faraday (Clinical Doctoral Research Fellow, ICA-CDRF-2017-03-060) is funded by Health Education England (HEE)/National Institute for Health Research (NIHR) for this research project. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR, HEE, NHS or the UK Department of Health and Social Care.
Ethical Approval
The study is a systematic literature review, and therefore, the work has not required approval from an Ethical Committee.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.