
Abstract
COVID-19 infection resulted in significant economic implications to patients as well as a considerable financial burden to the general population for preventive measures. A descriptive study was conducted among staff at one of the public universities in Malaysia to estimate the monthly out-of-pocket expenditures for preventive measures used for COVID-19 infection. The study tool includes questions on household out-of-pocket expenditure and the measurements of the impact of the expenditure on household income. It was found that the average cumulative monthly expenditures related to the preventive measures were US$ 45.90 (Ringgit Malaysia 187.77), which was 4.3% of the household income. The highest expenditures were for traditional and complementary medicine followed by nutraceutical/supplements and disposable facemask. 8% of the households in this study incurred more than ten per cents of their monthly household income for expenditures related to COVID-19 preventive measures. Several households are experiencing substantial financial implications for preventive measures related to COVID-19 infection. This study highlights the out-of-pocket expenditures incurred for preventive measures were substantial for certain households. Effective initiatives from the government on providing subsidized protective personal equipment and a cost-sharing approach could help to alleviate the household financial burden.
The COVID-19 infection has resulted in significant disease and economic burden globally.
This study measures the magnitude of the economic burden related to COVID-19 in Malaysia.
Findings from this study could help the stakeholders to plan for proper strategies to alleviate the economic burden experienced by the community.
Introduction
A fatal infectious disease caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), called coronavirus disease 2019 (COVID-19), is currently occurring in the world. Despite the announcement made by the World Health Organization (WHO) declaring COVID-19 as a global pandemic on March 11, 2020, at the time of writing, COVID-19 was continuing to spread globally and locally. 1 The transmission of COVID-19 can easily occur through respiratory droplets and direct or indirect interaction with the mucous membranes of the skin, mouth and nose. 2 The viruses are highly lethal in aerosols coming from sneezes, coughing and talking. To make it more challenging, the viruses can survive without losing its viability and virulence for weeks. 3 Other than the contact and droplet transmission, scientific evidence revealed that the COVID-19 infections were also transmitted through airborne transmission. Airborne transmission mainly occurs in indoor and crowded spaces with poor ventilation with a prolonged period of contact such as during dining in restaurants, small classrooms, prayer rooms and others. In these circumstances, COVID-19 transmission could occur if the facemasks were not properly worn and hand hygiene and social distancing were not appropriately practised.1,2 COVID-19 infects the respiratory tract typically presenting with mild symptoms of headache, dizziness, taste and smell dysfunctions and impaired consciousness to a more severe medical complication of acute major organ injury and lead to death in some infected people.4,5 As of January 25, 2021, a total of 183,801 confirmed cases of COVID-19 has been reported by the Malaysian government, with a .3% mortality rate. 6
As part of the federal government’s initiative to combat the rapid spread of COVID-19, public health interventions include non-pharmacological and legislative measures have been issued. All the guidelines prepared by the government are following the WHO recommendations as well as the knowledge on the disease dynamics. 7 As the main modes of transmissions are human-to-human transmission and air pollution-to-human transmission, 8 a set of Standard Operating Procedures (SOPs) was established based on the ‘3Cs’ and ‘3Ws’ guidelines. ‘3Cs’ means avoiding crowded environments, closed areas and close conversation. ‘3Ws’ implies the practice of frequent hand-washing with soap and water, wearing a face mask in public areas and warning against handshakes or physical contact at greetings. 9 Heavy penalties will be imposed on individuals who disobey the set SOPs, including a fine not exceeding US$ 245 (RM1000) or imprisonment up to 6 months. This includes the compulsory wearing of facemasks in public areas enforcement starting from August 1, 2020. The Malaysian government also encouraging their people to used hand sanitizer as a regular disinfection practice. 6
Due to the various modes of transmission and the disease dynamics of COVID-19 infection, it results in significant risks towards vulnerable populations such as elderlies, people with comorbidities, those with a low immune system and small children. Therefore, to shield vulnerable people, strict SOPs are needed to minimize their exposure to them. All the SOPs were outlined clearly by the government and were considered as the ‘new normal’ during the pandemic. 5 This ‘new normal’ procedure has had an impact on the lives of Malaysian people. When they were out of the public, they practised wearing protective masks, regular hand-washing or using hand sanitizer. 10 The new normal eventually made a paradigm change in social normality certainly gives an impact on the economy on the individual and community. One study reported that, there was a 66% increased in the consumption of single-use facemasks due to the mandatory use for health protection compared to pre-COVID era. 11 Additional expenses for the preventive measure resulted in significant financial implications to people, especially those from the low-socioeconomic background, a high number of family members and those with comorbidity conditions mainly because of the volume of the preventive measures that required for all household members with limited income to buy them.12,13
To date, many studies described the burden experienced by the patients and healthcare system and very scarce discussed the financial burden incurred by the general population. Findings from this study could help to describe the economic hardships experienced by the household during the pandemic even though they are not diagnosed with COVID-19 infection. With these findings, policy makers could make effective decisions for the patients, healthcare systems and general population like the legislation on the price of the preventive measures and also assistances to those economically -vulnerable populations. Studies by Lim KH and Azlan AA found that the adherence rate for facemasks and hand hygiene among Malaysians ranged from 50% to 80% and among the restricting factors was the costs and affordability to buy those items especially among lower-income households.14,15 However, both studies did not investigate the magnitude of the out-of-pocket burden. Therefore, this study tried to address the gap of knowledge on the actual financial implications experienced by the households. Among Malaysian, the cost was highly dependent on individual and family income. These costs are summed within all households in the various surveys and referred to as out-of-pocket (OOP) payments. Out-of-pocket healthcare payments are determined by all costs that are paid directly by the household. It would include buying for a face-mask or any preventive tool, user fees and co-payments, over-the-counter and prescription drugs, as well as doctor fees, hospital costs and related charges. 12
The strict lockdown implemented by the government, many households were found to stock up essential items like food, common medicines such as paracetamol, flu medicine, cough syrups and others including traditional and complementary medicine as well as nutraceutical/supplements.10,11 The panic buying resulted in an immediate increase in spending on household consumers. Nevertheless, the magnitude of the spending and its impact on household income was unknown. The study aimed to answer the main research question, which was how much, is the magnitude of the economic burden related to COVID-19 preventive measures incurred by households? This study assessed the economic burden in terms of out-of-pocket health expenditure for COVID-19 prevention incurred among the staff of the public university in Malaysia. These findings would be highlighting the impacts of COVID-19 that emphasize the economic aspect. By understanding the out-of-pocket expenditure on health, the results are useful to facilitate effective planning strategy and helping policymakers to identify new strategies in reducing the economic burden among Malaysians.
Materials and Methods
Study Design, Sample and Searching Strategies
This research used a cross-sectional study design and was carried-out for 6 months from July until December 2020. The study was conducted at 1 of the public universities in Nilai, Negeri Sembilan, The study participants were recruited through convenience sampling method. Lists of staff form all administrative departments and administrators at various faculties at Universiti Sains Islam Malaysia (USIM) were obtained from all the heads of the department and the deans of the faculties. The data were counter checked with the database from the Human Resource (HR) department. From the lists given, the staffs were identified, invited and included in this study.
The study participants include administrative staff with various grades and categories of job scheme in public service in Malaysia. The administrative staff was chosen to reflect various categories of staffs with huge range of monthly salaries, compared to academicians that have limited grades in the university. Information and invitation to join this study was disseminated to all departments and faculties through formal letters. Apart from that, formal emails were also sent through formal university email to recruit participants. To encourage more participation, participants who answered the entire questions were given a bottle of hand sanitizer as a souvenir. As this study was aimed to describe the preliminary findings on the out-of-pocket expenditures incurred by household, a convenient sampling method was used.
The study participants that fulfilled the inclusion and exclusion criteria were invited to join the study. The inclusion criteria were as follows: administrative staffs who were 18 years old and above, able to understand and communicate in Malay and English language and were willing to participate. Staffs who had problems with internet access and do not have any electronic device to participate and answer the questionnaire were not included because the main method of data collection was through Google form.
As USIM is 1 of the public universities in Malaysia, data from this centre can be used to estimate the economic burden related to COVID-19 disease from the perspective of community as various categories of administrative staffs are working at the university. It reflects a governmental organization with administrative staffs that have several grading and pay structures of the civil service in Malaysia. Apart from that, all of the researchers are currently working in USIM and ethical approval for this research has been granted. This study is also 1 of the bigger studies on the various impacts of COVID-19 conducted in USIM. At the moment, the researchers are expanding the study and national study is currently being conducted. The data collection is still on going and we hope to publish the finding soon.
Study Tool, Data Parameters and Measures of Variables Collected
A questionnaire was developed to collect data on basic socio-demographic profiles as well as household characteristics and OOP expenditure for preventive measures related to COVID-19 disease. The questionnaire was developed and validated by the research team prior to the actual data collection. Previously, the same questionnaire was used for a study on hepatitis C virus infection. 16
The questionnaire contained 2 parts: (A) Socio-demographic profiles and household characteristics; and (B) household OOP health expenditure related to preventive measures for COVID-19 disease. Questionnaire on household characteristics include income, size, number of people working, number of children and number of children attending schools. Questionnaire on the household OOP health expenditure for the preventive measures related to COVID-19 disease include expenditure for face-masks, face shield, hand sanitizers, gloves, wet tissues, supplements, traditional and complementary medicine (TCM) and also other reported preventive measures by the study participants.
All study participants in this study were required to sign an informed consent form after receiving information about the aim of the study, the type of data required and the method of data collection. All patients were required to complete the Google form given through their phone numbers or Whatsapp application or to their email addresses. The questionnaire was piloted and tested for face and content validity prior to actual data collection.
Data Analysis Procedures
Statistical analysis was performed using SPSS version 20.0 (SPSS Inc., Chicago, Illinois, USA). Descriptive analyses of socio-demographic profiles, household characteristics and household OOP expenditure were conducted. Visual assessment and normality testing (such as Kolmogorov-Smirnov test) were used to test for normality of distribution prior to conducting and reporting the descriptive analysis. Continuous variables, where appropriate, were presented as means and standard deviations (SD). For findings that were not normally distributed, median and inter-quartile range (IQR) were used. For categorical variables, results were presented as frequencies and percentages. All expenditure collected was in Ringgit Malaysia (RM) in 2020 price values, (US$ 1 = RM 4.09) and all the expenditure reported in this study was in US dollars.
Out-of-pocket health expenditures made were presented descriptively. The households were categorized into non-poor and poor based on national poverty line income for Malaysia. 17 In this study, poverty impacts were also reported. The poverty impact is the difference between poverty headcount and poverty gap before and after healthcare payment was calculated. Poverty headcount is the number of households with monthly household income below the defined poverty line. The difference in the poverty headcount before and after expenditures describes the incidence of poverty among included participants. The poverty gap is defined as the income shortfall among poor households below the poverty line. The difference in the poverty gap before and after healthcare payment illustrates the severity of poverty among included participants. 18
The expenditure and monthly household income were used to determine the proportion of OOP payments from the household income. 19 Any household with a value of more than 10% is considered to have catastrophic health payment due to out-of-pocket expenditure. The threshold of 10% is often used as an indicator of CHE in developing countries. 20
Results
Sociodemographic profiles and household characteristics of study participants.

The mean (SD) monthly household income among the 77 participants was US$ 1436.28 (865.21). The minimum monthly household income was US$ 195.60 while the maximum monthly household income was US$ 3667.48. Only 1 (1.3%) household was categorized as poor as the household income was below the national poverty line. In this study, the mean (SD) household members was 4 (2). 46 (59.7%) of the households were categorized as small household size, 27 (35.1%) were categorized as medium household size while only 3 (3.9%) had large household size. There was 1 missing value on the household size. Of all the 77 participants in this study, 65 of them have children in their households with the mean (SD) number of 2 (2). The mean (SD) number of children attending school in a household was 2 (1).
Types of preventive measures used and the mean OOP expenditure incurred.
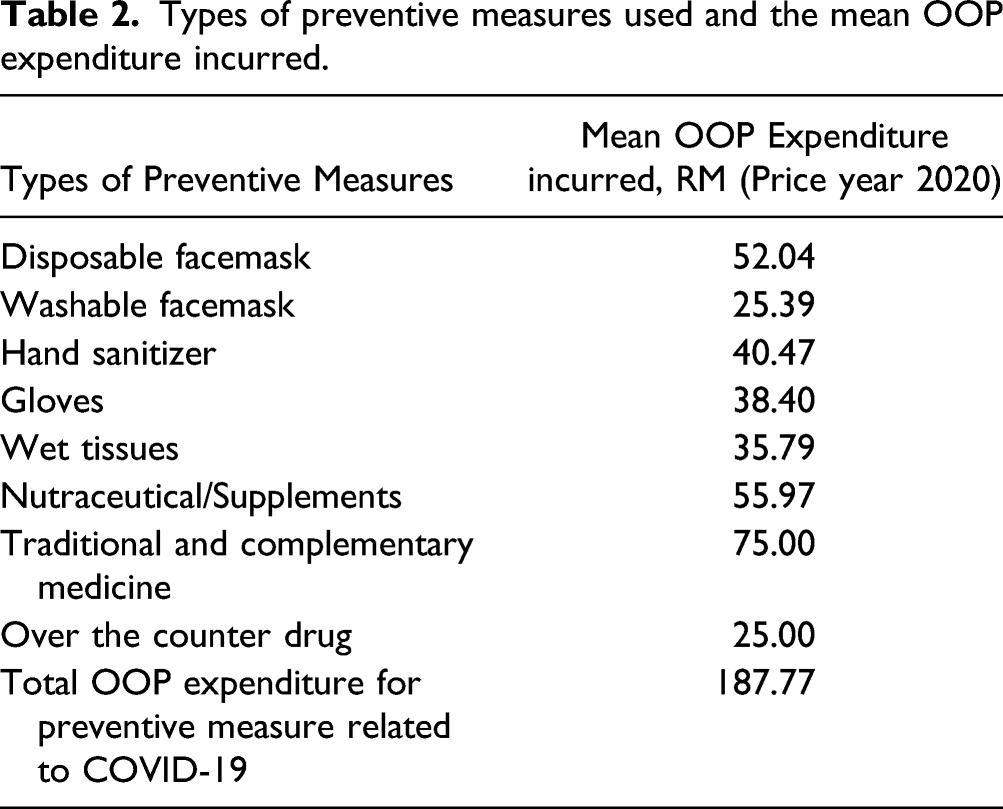
One participant reported to incur one-off OOP expenditure for COVID-19 Reverse transcription-polymerase Chain Reaction (RT-PCR) test was US$ 73.35 while 2 of the participants incurred one-time OOP expenditures for COVID-19 Antigen Rapid Test Kit (RTK-Ag), which ranged from US$ 12.22 to US$ 17.11. None of the participant incurred any OOP expenditure for face shield and N95 masks.
The mean (SD) percentage of monthly expenditure over household income among the study participants was 4.3% (4.87%). Figure 1 shows the average percentage of expenditure over household income based income categories. It was found that as the household income increases, the proportion of the expenditure over the income reduced. Average percentage of expenditure over household income based income categories.
Six out of 77 (8%) households in this study incurred more than 10% of their monthly household income for OOP expenditure related to COVID-19 preventive measures and was considered to experience catastrophic health expenditure (CHE). Among the 6 households, the mean (SD) monthly expenditure was US$ 109.21 (49.35) and the mean (SD) proportion of the expenditure to income was 17.2 (6.31).
Prior to the expenditure, 1 household (1.3%) was categorized as ‘poor’ as the household’s income was below the national poverty line. Following the expenditure incurred for the COVID-19 related preventive measures, the number of poor household remained 1. For that particular ‘poor’ household, the poverty gap prior to the expenditure was US$ 31.78 (RM 130). The OOP expenditure caused the poverty gap to increase to US$ 51.34 (RM 210), with an overall poverty impact of US$ 19.56 (RM 80).
Discussion
COVID-19 pandemic resulted in significant and unprecedented health and economic crisis worldwide. This pandemic not only leads to public health crisis however causes severe economic repercussions to countries, healthcare services, business, patients and their household as well as to the general population. It was reported that the economic shock took off soon after the initial outbreak of the pandemic as early as February 2020.
The economic implications of COVID-19 are huge and affect various groups of people globally, which are worse than the severe acute respiratory syndrome (SARS) and comparable to Zika and Ebola epidemics. 3 The economic impact of COVID-19 is highly significant in less developed economies especially in countries with poor healthcare system and population density is high whereby outbreak containment is challenging. The economic impact of COVID-19 is mainly due to the disruptions in the supply and demand chain. 4 The disruptions occurred due to the reduction in the manpower following mortality and morbidity of COVID-19 infection, disruption of production networks due to lockdowns and movement control orders, panic buying among consumers and others, which created market anomalies.4-6 Facemask markets and other preventive measures were among the affected businesses activities. The rising demands on these preventive measures resulted in the upward trends in the prices.7,21
Many studies reported the economic impacts of COVID-19 from various perspectives such as impacts on health systems and economies22-25 to describe the financial burden from the provider’s perspective. Studies that described on economic burden from individual perspective mainly concentrated on the out-of-pocket expenditures incurred by COVID-19 patients for treatment and clinical management of the disease. A study found that, COVID-19 treatment caused a household to spend approximately 25% of their income for related clinical management. 26 A similar finding on other pandemic reported on 2009 pandemic H1N1 influenza on direct non-medical costs 27 and by many community members where they were paying large sums OOP during the Ebola outbreak in 2014.28,29 Studies on general population perspective reported on the economic impacts on unemployment, underemployment and loss of income following the closing down of many businesses.30,31
Apart from the income and productivity losses, the society incurred significant amount of out-of-pocket expenditures for preventive measures during this pandemic. The lower income households are the most vulnerable group by the increasing prices of the preventive measures. While COVID-19 vaccine is effective to curb the diseases, many countries are still far from achieving the her immunity and therefore those countries are focussing on the non-pharmaceutical interventions such as wearing facemask, good hand hygiene and social distancing to control the pandemic.4,5 These interventions require people to buy and get the preventive measures, which could further exaggerate the economic burden of low-household income families. Our study found that, the out-of-pocket expenditure reported was on average US$ 45.91 (RM 187.77) per month per household, which was approximately 4.3% of the monthly household income for various preventive measures related to COVID-19. In Vietnam, a study found that, for a family with 4 household members, the average OOP expenditure for disposable facemask was VND 1.5 million. 32 The OOP expenditure was approximately 20% of their monthly household income for expenses on facemask only, which were higher, compared to our finding, which could be due to the price increase of three-to 10-fold compared to the regular prices due to the high demand particularly during the first months of the pandemic.
The regulation of wearing the mask in the public area to reduce the risk of getting COVID-19 infection has been made mandatory by the Malaysia government. 33 As a result, many people have to incur some amount of their out-of-pocket expenditures for facemasks as well as other preventive measures. A survey conducted among Malaysians reported that 96.7% of participants wearing face masks for COVID-19 prevention. 22 This is in line with finding from this study that found participants used face-mask as the preventive measure with the majority preferred used disposable face mask (97.4%) compared to the washable face mask (23.4%). In order to minimize the financial burden, Malaysia government has set a maximum retail price of US$ .24 (RM1) per unit for the disposable three-ply face masks on 15 August 20, 20. 34 In this study, we found the average monthly OOP expenditure on disposable facemasks was of US$ 12.72 (12.14) per household, which shows only slight additional household expenditure due to the pandemic. Previous study has found that, out-of pocket expenditure for preventive measure could create significant financial repercussion and can decrease adherence rate of preventive intervention. Therefore, the initiatives by the government have alleviated the related out-of-pocket expenditure by the society. 31
From this study, we found most of the participants also spending on hand sanitizer (93.5%) as a means of protection and prevention against COVID-19 with the mean OOP expenditure incurred of US$ 9.89. A study among Malaysians reported 88.7% always wash their hands using soap or disinfectant liquid when they were outside the home. 22 This could be due to campaigns and recommendations by government and other health organizations including WHO and Food and Drug Administration (FDA) on the utilization of disinfectant and hand sanitizer as the best way to prevent the spread of infections and decrease the risk of getting sick.35-37
Additionally, more than half of participants (62.3%) used wet tissue as the means of protection against COVID-19 with the mean OOP expenditure incurred of US$ 8.75 This concurs with another study that reported that antiseptic wet wipes were commonly used strategies after using masks and hand sanitizers to reduce infection risk rates for COVID-19. 38 Moreover, our finding is also in-line with a review of non-pharmaceutical behavioural measures to prevent COVID-19. Chan et al 39 (2020) reported the primary prevention of wearing face masks, using hand-sanitizer and wet tissue is the most preferred line of defence to reduce health risks when there is an absence of an effective treatment or vaccine.
Additional to the primary prevention recommended by a health organization, our study also found more than half of the participants (53.2%) are consuming nutraceutical food to boost their immunity in order to attain and maintain a good nutritional status, to fight against the virus. The mean OOP expenditure incurred was US$ 24.02, with the most common nutraceutical food was a Vitamin C supplement. This could reflect good health awareness and literacy among the study participants. The previous study has shown evidence that Vitamin C tends to make a robust immune system, thus boosting our immune system and treating or preventing any viral infections.40,41 Our study also found the highest mean OOP expenditure incurred was for TCM with US$ 18.34 (24.14). To date, there is no available evidence or guidance on the supplement other than Vitamin C and TCM used for COVID-19 prevention. 40 Therefore, these supplements shall be taken according to the body’s need, including Vitamin C, so it will not harm the health and negatively impact the financial burden, including making the unnecessary expenditure for ineffective supplement and TCM.42,43
According to the guidelines on COVID-19 testing using RTK-Ag from the MoH, this test is made a priority in cases or samples that require urgent result for prompt patient management to be given. However, RT-PCR is used for high-risk groups and screen for severe acute respiratory illness (SARI).44,45 Thus, the additional burden of OOP expenditure for COVID-19 testing may have impacting the community as reported in this study where they spend US$ 12.22 to US$ 17.11 for RTK-Ag and US$ 73.35 for RT-PCR. It was also found that, several agencies and organizations make it a compulsory for their workers and attendees to do the antigen test prior for them to report duty, to continue work or to attend any meeting. This regulation could cause financial burden to the people especially when they had to incur the cost of the test trough out-of-pocket payments.
Catastrophic health expenditure (CHE) is an OOP for healthcare coverage that exceeds the defined household income threshold. 46 This study defined CHE as direct OOP medical costs exceeding 10% of the monthly household income. 20 We found 7.8% of households experiencing CHE with mean (SD) monthly expenditure at US$ 109.21 (49.35) and the mean (SD) proportion of the expenditure to income was 17.2% (6.31). Available data on the COVID-19 pandemic to CHE remain limited. Nevertheless, from previously pandemic including Ebola, chikungunya and 2009 H1N1, CHE’s burden remains large infecting those in the low income, vulnerable group, from integrated areas and no insurance coverage.27,47,48
Finding from this study highlighted that OOP health expenditure was high in some households and cause of financial burden to them. Thus, this study could guide us to conduct a more extensive one in the future, particularly among those who had more prominent household members, had chronic conditions and had less economic security and reserves. Besides, economic challenges can often lead to socioeconomic disparities, which should be analysed from health and social perspective.49,50 Therefore, in addition to the quantitative approach, the qualitative approach can also be utilized to provide more in-depth perspectives on the health and economic impacts of this pandemic.
Moreover, in reducing the burden on healthcare expenditure, the employer needs to provide all necessary preventive measures to their employees including adequate amounts of quality face-masks and hand hygiene supplies at workplaces and work from home (WFH) policy. Additionally, governments also can attempt to ensure widespread financial protection against this infectious disease by covering the cost of care and loss of productivity in Social Security Organization (SOCSO). It was also reported that, a cost-sharing initiative for preventive services and any related preventive measures could benefit society, as it is 1 of the methods of cost-containment approach. The cost-sharing initiative has been proof to increase the adherence to preventive services as well as encouraging people to pursue a healthier lifestyle.51-53
Several policy responses are required to minimize the financial repercussions of COVID-19 infection. It was reported that, countries with higher investments in healthcare have applied a shorter period of lockdown, therefore minimizing the impacts on economic system and disruption of economic growth. Reinforcement of healthcare sector with high investments in health sector could alleviate the significant economic impacts on socioeconomic systems.21,53 The government plays critical roles by providing financial assistance to vulnerable household, entrepreneurs and other sectors while strengthening the healthcare system to minimize both disease and economic burdens of this pandemic. Also, adequate budget allocation should be provided to improve the capacity and preparedness of health systems.4-6 In Malaysia, approximately US$ 78 billion (RM 320 billion) was allocated for the Ministry of Health and US$ 2.5 billion (RM 10 billion) was announced to support small-and medium-size enterprises.3,7 Many studies have demonstrated that effective policies that identify people at risk and evaluate the vulnerability of localities to future epidemics based on environmental factors could help in planning for adequate health resources. The predictive analysis approach will support appropriate long-run strategies of infectious diseases on public health, economy and society.50,54-60
One of the strengths of this study is that this is the first study assessing the community’s preventive measure of COVID-19 risk comprehensively. By conducting this study, we can report the comprehensive types of prevention utilized by the community. With the ongoing pandemic situation, in addition to the increase in cases due to the third wave of COVID-19, the compound rate imposed by the government to ensure compliance with the wearing of face masks, the primary prevention will be 1 of the preventive methods used in society.61-63 This causes an increase in society’s financial burden as the majority will be spending their income on primary prevention of COVID-19. 62
Unfortunately, there is a limitation to this study. As a preliminary study, this study had a small sample size and only included civil servants. Thus, it may not represent the whole Malaysian population because they will not experience retrenchment, loss of a job and income loss. As this is a self-administered questionnaire where the participants fill it in themselves, without an interviewer, it is also possible that we will not wholly capture health expenses for all household members.
Conclusion
In conclusion, COVID-19 pandemic resulted in considerable economic implications. Several households experienced catastrophic health expenditure due to the high out-of-pocket payment for preventive measures. This study provides descriptive evidences on magnitude of burden related to out-of-pocket payment experienced by various households in Malaysia. Effective initiatives from the higher authority on providing protective personal equipment at workplace and cost sharing approach could help to alleviate the burden. Public should be given comprehensive health education on the appropriate prevention to minimize unnecessary expenditure on non-effective measures and non–evidence-based approaches. Nevertheless, this study provides limited information due to the small sample size and single-centred study area. Future and larger-scale national study is ongoing and could provides better perspective on the burden among general population in Malaysia and other South-East Asian countries with similar economic and health systems background.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.