
Abstract
Financing health care through out-of-pocket payments results in catastrophic health expenditure (CHE) and impoverishment in many Asian countries, such as Iran. The rate of households’ exposure to CHE is as high as between 8.3% and 22.2% in Iran. However, Iran's Ministry of Health and Medical Education (MoHME) launched a series of reforms in 2014 called as “health transportation plan (HTP)” to decrease the rate.
The findings showed that, despite implementation of the reforms in Iran, proportion of households facing CHE increased from 8.3 in 2011 to 14.2 in 2020.
The dental and inpatient services need to be more widely covered by basic health insurance and households having members ≥65 years along with the poor households should be exempted from paying some of the healthcare expenditures for improving their financial protection against CHE.
Introduction
Growth of health expenditures and increase in their share from Gross Domestic Product (GDP) are major concerns in most countries, especially in developing countries like Iran. 1 Such costs may impose a heavy burden on households and push many households into poverty. Hence, the World Health Organization (WHO) has a special emphasis on financial protection of households against healthcare costs and on access to necessary health services without any financial constraints during receiving the services. 2 The financial protection for the household occurs when household’s out-of-pocket (OOP) payments for healthcare services are in a logical proportion to its ability to pay; otherwise, some households will be exposed to catastrophic health expenditures (CHE). 3
The rate of households' exposure to CHE is one of the most commonly used indices to evaluate and control the financial protection status, and its use has been recommended by the WHO and the World Bank.2,4 WHO defines CHE as a state when household’s OOP payments for healthcare services is equal to or exceeds 40% of household’s income after paying for essential expenditures. 5 Such costs happen more in developing countries, where they rely more on OOP payments to finance health care. The share of OOP payments from the total health expenditures in Iran was as high as 58%, and subsequently, the CHE rate was significantly high, as several regional studies reported the rate of households' exposure to CHE between 8.3% and 22.2%. 6 These features were not in line with the objectives intended in Iran’s Fifth Economic, Social, and Cultural Development Plan; that is, reducing the share of OOP payments to 30% from the total health expenditure and decreasing the percentage of households’ exposure to CHE to less than 1%. 7 In addition to the problems mentioned above, there were some other problems with Iranian health system including low bed occupancy rate, informal payments, poor quality of care, inadequate response to increased demands, inequity in access to healthcare services, and insufficient insurance coverage. However, Iran’s Ministry of Health and Medical Education (MoHME) launched a series of reforms in 2014 called as “health transportation plan (HTP)." The plan followed 3 main objectives introduced by WHO: improving health, enhancing responsiveness, and raising financial protection of households against healthcare costs. To achieve the goals, the MoHME introduced some health service packages including many interventions. The majority of interventions focused on financial protection of households against healthcare expenditures. Such interventions included covering uninsured people by health insurance with no premiums; decreasing coinsurance to 5% and 10% for rural and urban residents, respectively, in order to make it easier for them to receive hospital services in public hospitals affiliated with the MoHME; eliminating informal payments through increasing medical tariffs; reducing the amount of money paid by patients qualified for basic health insurance coverage by 6% and 3% of the total hospitalization expenditures for urban and rural residents, respectively, and also for residents of cities with <20,000 population; providing all necessary medicines, consumables, and other related health services inside the hospitals; and reducing the number of unnecessary referrals to private centers. The plan was funded by 2 main public sources: 10% of incomes earned by the targeted subsidies initiative and 1% of the revenues obtained from value-added tax. 7
Nevertheless, this plan imposed a heavy burden on government and information about the degree of success in achieving the goals, especially in terms of financial protection, which is ambiguous. Several studies have evaluated the rate of CHE after implementation of HTP,7-9 but only 1 study calculated the rate using a before and after approach. 6 The study compared households’ exposure rate to CHE in both before (2008) and after (2015) the implementation of HTP using local data. Since the data obtained from 2015 were for less than 1 year after implementing HTP, it could not show the real effects of HTP on financial protection of households. Considering the lack of information in this area, the goal of present study was to examine the rate of CHE before (2011) and after (2020) the HTP using local data.
Methods
In 2011, a survey was conducted in Yazd city, a city located in central part of Iran with a population close to 1 million. The survey was carried out to determine the amount of households’ exposure to CHE and to identify factors associated with CHE among households. 10 In 2020, the same households were re-examined and the changes were compared. Neighboring households were selected instead of the households that could not be included in this study for any reason.
Sampling and Sample Size
In 2011, a 2-stage cluster sampling design was used for selecting samples. In the first stage, 18 health centers, as 18 clusters, were selected based on geographical sampling framework that covered the entire population of the city. The number of households in each of the clusters was calculated based on proportion of the population under coverage of each health center. Each of the 17 clusters represented 22 households (17 × 22 = 374) and 1 cluster was 36 households. In the second stage, the cluster head of each cluster was selected based on information recorded for each individual in each center.
In 2020, we followed the same households (or addresses) which were included in 2011. Of 386 addresses available from the 2011 survey, 43 households were missing for various reasons such as changed street plates, building demolition, and households’ unwillingness to respond. The missing cases were replaced with neighboring households.
Data Collection
The World Health Survey (WHS) questionnaire developed by the WHO was used in both surveys. The questionnaire includes individual and household questions, and its validity and reliability have been confirmed in Iran. 11 Data were collected through face-to-face interviews in person’s home during a single visit. At household level, a member ≥18 years old who was willing and able to answer the questions and had the most information about households' general and healthcare expenditures was selected to complete the questionnaire. If, for any reason, the interviews could not be conducted with the selected household, it was replaced with the next nearest right-neighboring household. Data quality control was carried out through checking the collected data by telephoning 8 % of the households. This study was approved by the SSU Ethics Committee with the following identification code: IR.SSU.SPH.REC.1398.095. The written informed consent was obtained from all participants prior to data collection.
Statistical Analysis
Catastrophic health expenditures were calculated through the WHO approach. In parallel, health OOP payments equal to or exceeding 40% of capacity to pay were determined as CHE. 5 A household due to OOP payments was considered as an impoverished household which has its total household expenditure after paying for health expenditures below the poverty line. The relationships between the variables (economic status, health insurance status, having members aged above 65 years or under 5 years, having disabled members, dental, and inpatient and outpatient services usage) and CHE were examined by Fisher’s exact test, as well as the differences between characteristics of both surveys was assessed by t test or x 2 test. In addition, the impacts of the variables on CHE were assessed by logistic regression model. Stata version 15 was used for data analyses.
Results
Characteristics of Both Surveys' Respondents.

aSignificant difference between variables of 2 surveys by t test or x2 test.
Percentage of Households Facing CHE and Households Being Impoverished due to Health Expenditures.

Note. CHE = catastrophic health expenditures.
aSignificant difference between variables of 2 surveys by t test.
Relationship Between the Characteristics of Households Facing CHE and the Variables in Both Surveys.
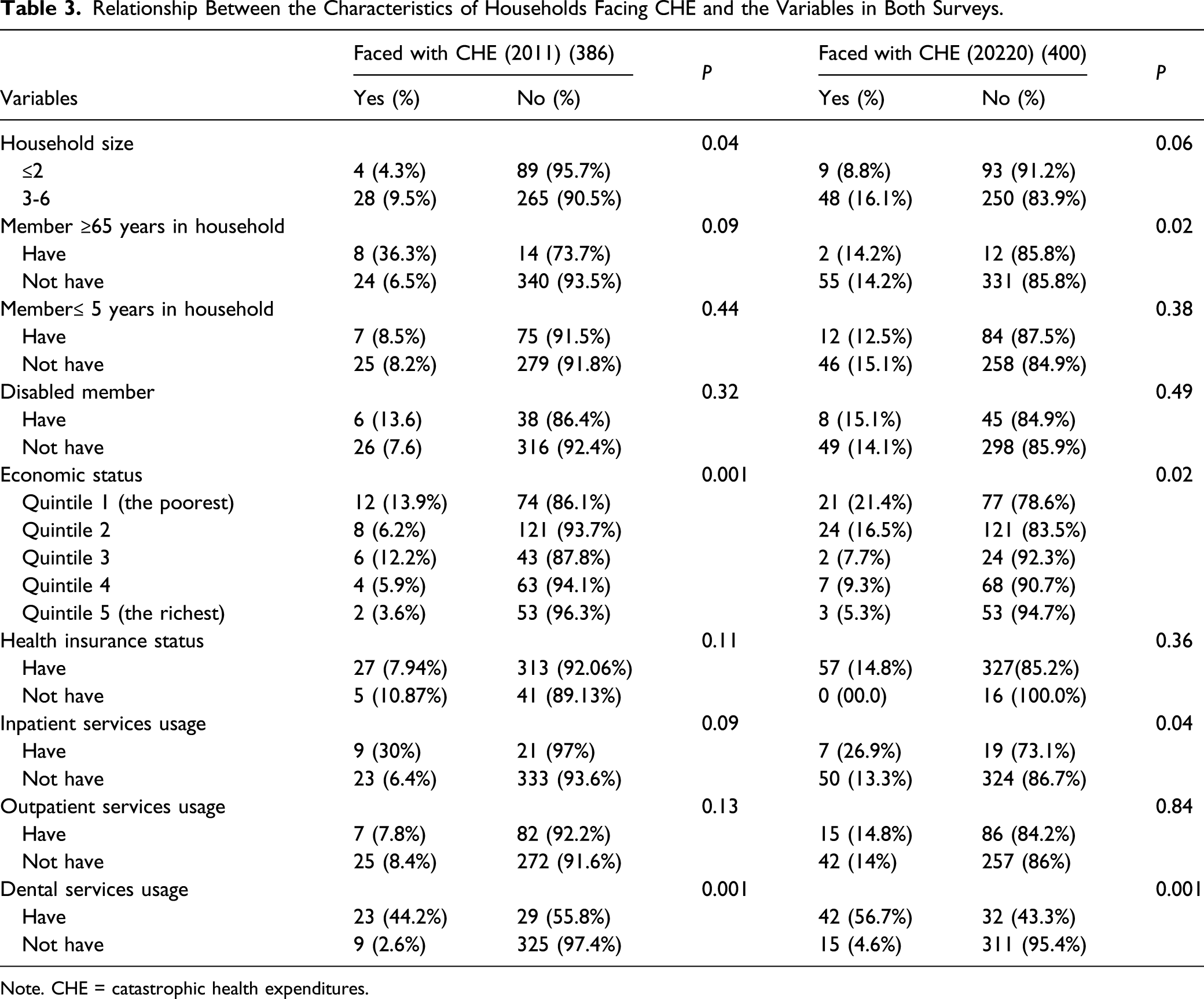
Note. CHE = catastrophic health expenditures.
Determinants of Catastrophic Health Expenditures in Logistic Regression Model.

aP < 0.05.
Discussion
The present study assessed the rate of the households’ exposure to CHE and the effects of socio-demographic and clinical factors on CHE before and after the HTP. The results of our study provided important insights into the CHE based on households’ characteristics that can be more appropriate for policy makers. Mean of CHE rate for households was as high as 8.3 and 14.2 in 2011 and 2020, respectively. The rates were higher than the results (3.91 %) obtained from a systematic review and meta-analysis carried out on the pooled data of 1995 to 2015 in Iran. The findings also fell in the high range of 8.3% to 22.2% of the CHE in several regional studies conducted using the WHO questionnaire on Iranian households between 2009 and 2014. All findings showed that the rate of households facing CHE is high and is not in line with the Iran’s Fifth Economic, Social, and Cultural Development Plan aiming to reduce the proportion of households facing CHE to less than 1%.
Despite having a major reform in this period, we observed that the proportion of households facing CHE increased from 8.3 to 14.2. The only other regional study, which was conducted in district 17 of Tehran, capital of Iran, and was similar to our study, showed that the percentage of households’ exposure to CHE increased from 11.8 in 2008 to 29.9 in 2015, 6 while it was expected to observe significant reduction in CHE according to the data collected in the first year after implementation of the HTP. The percentage of increase in CHE (153 %) for the study was conducted in Tehran was higher than that (71 %) in our study. 6 One possible reason for this finding can be explained by different characteristics of the population living in district 17 of Tehran compared with Yazd population. The district’s population was associated with low socioeconomic status, high rate of immigrants, and work of many residents in hard physical occupations.6,11 The increase in percentage of CHE after implementing the HTP was also observed in a study carried out on national survey data by Yazdi-Feyzabadi et al. 9 They pointed out that the exposure rate to CHE increased from 1.99 in 2011 to 3.46 in 2017 in total urban and rural population. The increase rate of CHE in the aforementioned study (73 %) was almost similar to that of 71 % in our study. 9
One of the most points emphasized by policy analysis for success in the implementation of health policy is the equity in healthcare financing. Atun et al. (2015) assessed the health system reform in Latin America and presented that inequities in the health system was one of the most important effective factors on the development and implementation of health reforms. 12 Moghadam et al. (2019) showed that the inadequacy of health system’s financing indicators and the high average OOP (about 55%) in Iran were the main challenges of HTP.9,13 In recent years, the inadequacy healthcare financing in Iran, especially in the public inpatient sector, following the various economic sanctions deteriorated.
The increase in public health tariffs aiming to make the tariffs closer to the actual final prices is one of the reasons for the high rate of CHE after implementing HTP in this study and the above-mentioned studies. Some empirical evidence showed that the proportion of OOP payments was reduced, but the final OOP payments were not decreased due to the sharp increase in public health tariffs.6,14 According to the WHO report (2010), the negligible CHE occurs when the OOP drops by 15 % in a country. 15 Yardim et al. observed that the rate of CHE decreased to .6 after implementing the HTP in Turkey. They presented that decreasing OOP payments by 19.3 % after the plan was one of the most important reasons for diminishing CHE. 16 Moreover, OOP payments is a common source of healthcare financing in low-income countries and some of middle-income countries like Iran, which increases the chance of catastrophic payments. However, implementing universal healthcare (UHC) in these countries is the most effective way to access health services without facing financial hardship, and UHC should be a high priority for the countries. 17
A major part of the high rate of households’ exposure to CHE is related to the high annual inflation rate in Iran’s economy, especially in recent years. The average annual inflation rate between 2015 and 2019 (20.58) was higher than that of 2010 to 2014 (18.64). In addition, the percentage of increased annual inflation rate from the beginning of the plan until the end of 2019 was 246 %. 17 This inflation has led to a sharp rise in the prices of goods and services and, consequently, an increase in health costs. As when comparing the mean expenditures of the household health services in 2020 with those in 2011, the mean health expenditure was almost 3 times higher than that in 2011. Another reason for the difference in CHE rate before and after the plan can be due to the increased application of the new diagnostic and medical technologies in Iranian health system in recent years. For example, the use of MRI in diagnosis services was not so common in 2011 while in recent years, it is highly used.
The findings showed that only the impact of having members ≥65 years in household on CHE changed to significant in this period. A systematic review and meta-analysis reported that having a member aged 60–65 years or older in the household in 12 of 40 studies increased levels of CHE in Iran. These members are not usually employed and do not earn any income as well. On the other hand, the age-related comorbidities are more prevalent in older adults. Therefore, presence of such members makes households spend a greater part of their capacity to pay on healthcare expenditures. The positive relationship between presence of the member ≥65 years in household and more likelihood of facing CHE was observed in some other countries, such as Turkey. 16
With regard to the features of insurance, it is expected from the health insurance to have a protection effect for the household against CHE. Nevertheless, this effect was not observed in this study. Some evidence of regional studies on Iranian households supports this finding. 18 One reason for failure of health insurance in protecting the households may be the fact that the insurance increases utilization of health care and, subsequently, the risk of CHE. This hypothesis that insurance coverage increases healthcare usage is supported by some studies.3,19,20 These findings suggest that more resources need to be allocated on improving the pattern of patient healthcare usage, managing providers for reducing supplier-induced demand or provision of unnecessary care, and providing healthcare insurance.
The household economic status was a key factor determining CHE in both surveys; as households with better economic status had lower chance of exposure to CHE. This reverse relationship between economic status and facing CHE has been mentioned in the majority of studies in Iran7,11,21 and other countries.16,22,23 Hospitalization is one of the other significant predictors of CHE in both surveys. Compared to 2011 (OR = 6.47), the households receiving inpatient services in 2020 had more chance of facing CHE (OR = 8.19), while it is expected that the rate of exposure to CHE after implementing the plan to be lower in comparison with that of the 2011. 10 This finding was consistent with that of the other study that was conducted before and after the plan in Iran. 6 One possible reason for this can be due to more use of private sector services with their services being expensive and not being covered by the plan.
We found that dental care usage was the most important determinant of CHE in both surveys. Dentistry services are among the more expensive healthcare services in Iran and are not usually covered by basic health insurance benefit packages. Most people pay directly out-of-pocket for receiving such services. This finding supports the results of other studies conducted in Iran,6,11 and other countries such as Brazil 22 and Korea. 23
The present study has some limitations that should be noted. Although the households of each cluster in cluster sampling method are almost similar in terms of socioeconomic characteristics, and in this study, the missed and replaced households were not exposed to CHE, 11% missing cannot be ignored. The participants were restricted to the Yazd province, center of Iran, who may not be perfectly representative of other Iranian population. Thereafter, our results should be applied with caution.
Conclusion
This study showed that, despite implementation of the reforms in this period, proportion of households facing CHE increased from 8.3 in 2011 to 14.2 in 2020. Similar to other studies that compared the rate of CHE before and after the plan, we also found that the objective emphasized in the Fifth Economic, Social, and Cultural Development Plan (i.e., reducing the proportion of households facing CHE to less than 1%) is not yet achieved.
The findings of this study and other studies in Iran indicated that dental and inpatient services were the key determining factors for CHE and those services need to be more widely covered by basic health insurance. The results also showed that the presence of a member over 65 years in household and households with low economic status were among the factors leading to a significant increase in the chances of facing CHE. In this regard, households having member ≥65 years and the poor households should be exempted from paying some of the healthcare expenditures for improving financial protection against CHE.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Shahid Sadoughi University of Medical Sciences (6837).
Ethical Approval
This report is part of a MSc project that was approved by the committee of Shahid Sadoughi University of Medical Sciences (approval number: IR.SSU.SPH.REC.1398.095).
Informed Content
Written informed consent was obtained from all subjects before the study.