
Abstract
Background
Many features of health care organizations (HCOs) have been identified to be associated with health information exchange (HIE), but subcategories of organizational factors focusing on nurse workforces still need to be identified. The objective of this study is to investigate the association of number of nurses with HIE use in Korea.
Methods
This study had a retrospective study design and used health insurance claim data from June 1, 2016 to June 30, 2018. The unit of analysis was the HCO, and any health insurance claims having HIE were counted by HCO. There were a total of 1490 HCOs having any HIE and 24 026 HCOs not having HIE. For statistical analysis, two-part model was used: logistic regression for HIE participation and the generalized linear model for the volume of HIE use.
Results
HIE was used by 44.6% of general hospitals, and 8.6% and 5.3% of small hospitals and clinics, respectively. Both HIE use and its volume were significantly positively associated with nurse variables. The use of HIE was significantly positively associated with nurse-to-bed ratio in general hospitals (OR 1.028; 1.016 to 1.041) and in small hospitals (OR 1.021; 1.016 to 1.027), and with the number of nurses (OR 1.041; 1.028 to 1.054) in clinics (P<.001). The volume of HIE use was also positively associated with nurse-to-bed ratio in general hospitals (OR 1.010; 1.004 to 1.017) and in small hospitals (OR 1.014; 1.006 to 1.022), and with the number of nurses (OR 1.055; 1.037 to 1.073) in clinics (P<.01).
Conclusion
This study found that there was a low rate of HIE use in small hospitals and clinics. The number of nurses was critically associated with the use of HIE and the volume of HIE claims. HIE policy makers need to be aware of this factor in seeking to accelerate HIE.
Keywords
● Health Information Exchanges (HIEs) are influenced by several factors at governmental (e.g., HIE regulations), organizational (e.g., information technology infrastructure, Internal rules, etc.), and behavioral levels (e.g., collaboration and communication among providers and health care organizations (HCOs), etc.). However, there was not any studies verifying the relationship between HIE and the volume of nurses in HCOs.
● The study findings can contribute to the knowledge expansion of health service research and medical informatics fields: the number of nurses is strongly associated with HIE use and volume of HIE in all types of HCOs. The study result was based on large data brought from the entire national health insurance clams.
● The result of this study indicates that healthcare policy makers should be aware of organizational factors, especially the magnitude of nurses, to promote and to accelerate HIE use in hospitals and clinics. Enforcing the education and training of HIE for nurses would be one of strategies to expand HIE.Highlights: Association of the Magnitude of Nurses With the Use of Health Information Exchanges: Analyzing the National Health Insurance Claim Data of Hospitals and Clinics in Korea
Introduction
The government of the Republic of Korea (hereafter “Korea”) has implemented a nationwide health information exchange program called as “the Patient Referral and Transferring System (PRTS)” since June 1, 2016. This system has been operated by the government agency, Health Insurance Review and Assessment Service (HIRA), which runs the nation health insurance program providing professional health insurance review and assessment services. Healthcare providers can send and receive patient’s clinical information through the PRTS. Healthcare organizations (HCOs) using the system get a small amount of additional reimbursement arranged from approximately $20 to $60. Technically, the system was developed based on IT standards with Health Level7’s Fast Healthcare Interoperability Resources (FHIR).
Sending and receiving patient’s clinical information through an electronic system has been called as electronic Health Information Exchanges (HIE). Electronic HIE is defined as a process of allowing health care professionals to access or share a patient’s information electronically in a pertinent and protective manner. 1
According to a study conducted in the European Union (2014), European hospitals used HIE to different extents for different purposes: for sharing information with other hospitals (39%), with external general practitioners (GPs) (36%), and with external specialists (33%). 2 A study conducted by the Organization for Economic Co-operation and Development (OECD)’s Health Information and Communication Technology (ICT) Benchmarking Pilot Group in 2016 showed that there was considerable variation between countries in HIE use. 3 A comprehensive literature review study on HIE in the U.S showed that HIE use has substantially risen since 2000, and approximately 40% of physicians in 2013 and 82% of non-federal hospitals in 2015 used HIE. 4 However, it is not academically known why and how many hospitals and clinics has participated in HIE in Korea.
Several factors have known to affect or be associated with HIE use. HIE use was associated with government programs such as the American Recovery and Reinvestment Act of 2009 and meaningful use requirement in the United States.5,6 Patient factors such as age, prior healthcare, and status of chronic condition were associated with HIE use. 7 For example, a comprehensive review study found that patient factors such as their benefits and concerns, and types of health information were also critical factors associated with HIE use. 8 Patients’ participation or willingness to share medical data is indeed an important factor in HIE use. 9
However, several studies suggest a possibility that number of nurses of HCOs may be closely related with use and volume of HIE. One study investigated the use of HIE, focusing on the user. 10 The study stated that clinical sites with nurses who had the access to HIE showed the highest use of HIE but the sites without the access by nurses had very low usage of HIE. Another study showed how HIE was used differently in 2 different role-based workflow models: nurse-based and physician-based. 11 One thing clear in this study is that nurses ask patients about recent hospital visits and record details on various notes. Thus, if there are many nurses, then possibility of HIE to other hospitals would increase.
Both studies were meaningful since they analyzed the use of HIE in different clinical sites focusing on nurses and suggested the possibility of connecting the sources of HIE with nurses. In addition, HIE is also associated with physicians’ coordination and provider communication, 12 nurses’ experience, their working conditions such as having a friendly adviser. 13 These studies also suggest that HIE may be closely related with number of nurse in HCOs because physicians in clinical settings would generally speaking have close collaboration and communication with nurses.
The Task-Technology Fit Model14,15 proposed by Goodhue and other colleagues20,21 assumes that supporting a task with technology will improve individual and group performance if organizations can harmonize task and technology. This theory may support our prediction. From here, the former, “Task,” could be defined and measured by various activities related with nurses or their volume, and the latter, “Technology,” could be defined and measured by HIE use (explicitly, PRTS) or similar ways. This could be a broad conceptual framework investigating the relationship between HIE use and the number of nurses.
Even with several previous studies on HIE use, none of studies directly investigated the relationship between HIE use and nurses. Previous studies also did not clearly show the robust relationship between HIE use and number of nurses. In addition, these studies are qualitative studies based on observation and interviews having limited clinic sites. Thus, it is necessary to verify whether there are any significant relationships between two contexts using quantitative data. Therefore, this study sets for a hypothesis that HIE participation and the volume of HIE use will be associated with the number of nurses.
It is crucial to know that nurse’s workforce factor help to overcome and eliminate the hurdles hindering HIE use in order to increase the adoption of HIE in empirical clinical settings. The roles of nurses in clinical setting are core factors to deliver healthcare. There are differences in the roles of the nurses in terms of their feeling and competencies. For example, nurses in Finland take an important role in care treatment ordered by general practitioners. 16 In Korea, nurses have expanded their roles, leadership, and working scopes rapidly.17,18 Thus, there is still much room for us to delve into how they are related to HIE use and how we could encourage them to use more clinical information to enhance HIE.
Therefore, this study aimed to investigate the current relationship between HIE use and number of nurses in clinical settings. Using both health insurance claims and administrative data which were objectively collected and measured, this study expects to contribute the knowledge expansion on unknown relationship between two contextual factors.
Methods
Study Design
This study was approved by the Institutional Review Board (IRB) of HIRA on February 05, 2018 (IRB No. 2018-004-001). The unit of analysis in this study is HCO such as hospital and clinic. In case of hospitals, there are 3 types of hospital in Korea: tertiary hospitals, general hospitals, and hospitals (hereafter “small hospitals”). The Medical Law and the National Health Insurance Law differentiate hospitals according to the number of beds and the number of medical specialties. In Korea, general hospitals should have either 100-299 beds and at least 7 medical specialties or more than 300 beds and 9 specialties. Small hospitals should have more than 30 beds but do not belong to the category of general hospitals. There were 43 tertiary hospitals, but they are excluded from the study because all hospitals participated in HIE without exception. Therefore, the study population consisted of: 301 general hospitals (GHs), 1466 small hospitals (SHs), and 30 938 clinics (CLs). Most of these HCOs had adopted EMR systems: general hospitals (96%), small hospitals (92%), and clinics (94%). 19
Data Collection Procedure
This study used the secondary administrative data on health insurance claims and HCOs. All health insurance claims were retrieved from HIRA’s Data Warehouse (DW) having any HIE claims from the time the HIE program started until June 30, 2018. HCOs should use the PRTS in order to get the HIE fee reimbursement. Through the PRTS, they can send and receive patient’s clinical information. HIRA′ DW system has kept HIE use records including health insurance claims. Generally speaking, HIRA’s database systems have collected health insurance claims data and other administrative data from various health care institutions, which is specifically described in one of previous studies. 20
This study obtained all the HCOs’ institutional data from the administrative DW. After retrieving the claim data and institutional data, this study merged both sets of data together by using each HCO’s identification (ID) number and, then, excluded potential study subjects which were not consistent with the study purpose. After reviewing the merged data, this study excluded 7 general hospitals, 55 small hospitals, and 7127 clinics due to missing values for the number of beds or the number of nurses (Figure 1). Data integration and management process.
Outcome and Predictor Variables
This study has two main outcome variables. One is whether HIE was used by an HCO or not, which allows analysis of which features of the HCO are associated with the use of HIE. The other is the volume of HIE use. For HCOs using HIE, this study explored the relationship between the features of HCOs and the volume of HIE use. This study did not differentiate whether the claims were for inpatients or outpatients. Once HCOs had any inpatient or outpatient claims, this study considered the HCO as using HIE.
Our selection of predictor variables was based on previous studies examining the relationship between HCO’s characteristics and HIE partition or use. Independent variables in this study are types of HCO ownership (private vs public),21,22 practice type (only for clinics),23,24 how many years the HCO has operated,13,25 location of facility (urban vs rural),21,23 the number of beds,21,26 and the number of registered nurses (RNs). 11 For the facility location, urban location means the administrative district having more than 100 000 residents and rural location is the one with less than 100 000 residents. Practice type was measured with solo vs multi-specialty. This study had information on the number of physicians and inpatients which were excluded from the analysis due to high correlation with the number of nurses and the number of beds. For the number of nurses in clinics, this study included certified nurse assistants (CNAs) in addition to RNs because many clinics hire CNAs instead of RNs. According to the Korean Medical Law, physicians, dentists, and oriental doctors in primary care clinics can directly supervise or guide CNAs without having nurses, so that CNAs can help physicians and provide nursing care services. Thus, many clinics do not have RNs.
Data Analysis
Before conducting the main analysis, we looked at the general characteristics of HCOs. This descriptive analysis was conducted for each class of HCO types (GHs, SHs, and CLs), because they have distinct characteristics such as the numbers of beds and nurses. In addition, separate descriptive statistics were derived and compared for two groups of HCOs: HCOs submitting HIE claims vs not submitting HIE claims. When comparing the statistical difference between two groups, we conducted t-tests when the target variable was numeric and Chi-square tests when the target variable was categorical.
We also examined correlations among covariates, and then excluded or transformed variables having high correlations to avoid multicollinearity issues. Excluded covariates were the numbers of inpatients and physicians. Considering the volume of nurses, the number of nurses was transformed to the nurse-to-bed ratio in hospitals for regression models, but the raw number of nurses was considered in clinics because most of clinics do not operate beds.
For the main analysis of the relationship between HIE use and HCO covariates, this study conducted a logistic regression. For the volume of HIE use, this study diagnosed the distribution of the outcome variable and found that it was heavily skewed to the right side which is the number of HIE use. This study presumably fitted a model with other variables following the suggestions of previous studies1-3 and used its residual information in the main analysis. Specifically, this study conducted the regression analysis using the generalized linear model (GLM) in which the GENMOD procedure of the SAS program was used with “LINK = LOG” and the “DIST = GAMMA” options. All data analyses for this paper were generated using SAS/STAT software, Version 9.4 of the SAS System for Windows, 27 and statistical significance was assessed at alpha level of .05.
Results
General Characteristics
General Characteristics of Healthcare Organizations.

HIE: Health Information Exchange.
Factors Associated With the Use of HIE
Association of Healthcare Organization Features With HIE Use and Its Volume: General Hospitals.
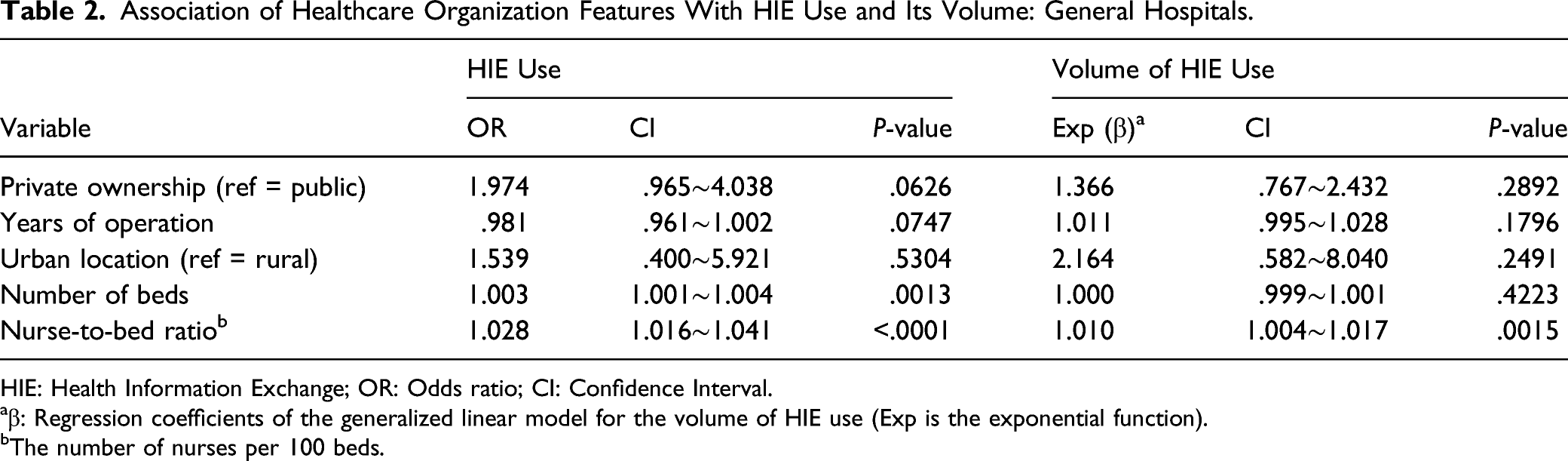
HIE: Health Information Exchange; OR: Odds ratio; CI: Confidence Interval.
aβ: Regression coefficients of the generalized linear model for the volume of HIE use (Exp is the exponential function).
bThe number of nurses per 100 beds.
Association of Healthcare Organization Features With HIE Use and Its Volume: Small Hospitals.

HIE: Health Information Exchange; OR: Odds ratio; CI: Confidence Interval.
aβ: Regression coefficients of the generalized linear model for the volume of HIE use (Exp is the exponential function).
bThe number of nurses per 100 beds.
Association of Healthcare Organization Features With HIE Use and Its Volume: Clinics.

HIE: Health Information Exchange; OR: Odds ratio; CI: Confidence Interval.
aβ: Regression coefficients of the generalized linear model for the volume of HIE use (Exp is the exponential function).
In addition, the estimated OR of the number of beds was 1.003 (95% CI 1.001 to 1.004, P = .0013): The odds of using HIE increased .3% as the number of beds increased by one. Clinics’ practice type (OR .632; .547 to .730, P < .0001) and urban location (OR 3.335; 2.269 to 4.903, P < .0001) were significantly associated with HIE use. The odds of using HIE in multi-specialty clinics was 1.582 ( = 1/0.632) times higher than that in solo-type clinics, and the odds of using HIE in clinics located in urban areas was 3.335 times higher than that of rural clinics.
Factors Associated With the Volume of HIE Use
The associations of HCO covariates with the volume of HIE use by HCO types are also presented in Tables 2-4. The volume of nurses was also significantly associated with the volume of HIE use in all three HCO types. The estimated ORs of nurse-to-bed ratio were 1.010 (95% CI 1.004 to 1.017, P = .0015) and 1.014 (95% CI 1.006 to 1.022, P = .0007) in general hospitals and small hospital, respectively: When nurse-to-bed ratio increase by one, the odds of the volume of HIE use increase by 1.0% and 1.4%, respectively. In clinics, the number of nurses was also significantly associated with the volume of HIE use (OR 1.055; 1.037 to 1.073, P < .0001).
Except general hospitals, the years of operation were significantly associated with the volume of HIE use in small hospitals (OR 1.089; 1.051 to 1.129, P < .0001) and clinics (OR 1.021; 1.012 to 1.030, P < .0001): The odds of the volume of HIE use increase by 8.9% and 2.1% as the years of operation increase by one for small hospitals and clinics, respectively. The practice type of clinics was significantly associated with the volume of HIE use (OR .522; .430 to .634, P < .0001): The odds of the volume of HIE use in multi-specialty clinics was 1.916 ( = 1/0.522) times higher than that in solo-type clinics.
Discussion
This study investigated the relationship between HIE use including volume of HIE and number of nurses in different types of HCO. The study found that the HIE utilization rate in general hospitals, small hospitals, and clinics was 44.6%, 8.6%, and 5.2%, respectively. This study also investigated the relationship of HCO features with HIE use and its volume. Both HIE variables were significantly positively associated with number of nurses in all three HCO types. It was also positively associated with the number of beds in general hospitals, and clinics located in urban area and practicing multi-specialty were more likely to use HIE. The volume of HIE was increasing as HCO’s years of operation in small hospitals and clinics.
For the HIE utilization rate, the results of this study can be compared with European study results showing 36% of HCOs utilized HIE. 2 This study result is aligned with the following study which found that, for general hospitals, the proportion of documents digitalized in the EMR system was much higher than that for small hospitals. Moreover, clinical documents were received at general hospitals with generally higher frequency than at small hospitals. 28 The reason why the HIE use in general hospitals was much higher than that in small hospitals and clinics may due to the significant differences in the study population: the number of general hospitals was 294, whereas the numbers of small hospitals and clinics were 1411 and 23 811. Another reason could be various technical issues such as slow system speed and low data interoperability which primary care clinics faced in Korea. 29 The limited healthcare ICT infrastructure of clinics is one of problems preventing the adoption of HIE among clinics. 30
It is a very interesting finding that HIE use is associated with the number of nurses. Are HCOs with more nurses more likely to arrange the patients’ referrals or transfer in? HCOs with more nurses may give more information on patient referral to doctors, which may trigger the use of HIE. The study result may be aligned with two previous studies in which either physicians or nurses are critical roles in HIE although two studies analyze several clinical cases.10,11 Regarding the number of beds in general hospitals, there is a higher possibility of HIE use as the number of beds increases. Large hospitals may have higher medical necessity to make patient referrals due to short length of stay for acute patients. Urban clinics are more likely to use HIE than clinics in rural areas. Clinics in urban locations may easily transfer patients to larger hospitals which are generally located in urban areas, while patients living in rural communities may go directly to large hospitals, which may reduce the use of HIE in clinics. It seems natural that multi-specialty clinics make fewer referrals and have lower needs for HIE use than clinics in solo practice type. These factors need further research because there have been few studies of these issues.
Regarding the relationship between the features of HCOs and the volume of HIE use, it is also a very interesting finding that the number of nurses was still related with the volume of HIE use in all three types of HCOs. This study finding could be explained in terms of the links between the number of nurses and the use of HIE suggested above. It is also an interesting finding that small hospitals and clinics with more years of operation made more HIE claims. Small hospitals with more years of operation may have more referral networks with larger hospitals, which may result in the positive relationship between years of operation for small hospitals and the volume of HIE use. This relationship was also observed at the general hospitals although it was not statistically significant. Other than that, compared to multi-specialty type, solo-type was negatively associated with the volume of HIE use in clinics. We have some limitations in providing full discussion of the results because there have not been similar studies.
Although this study has yielded meaningful results, there are some limitations. First, most HIE use inevitably occurs due to patient factors, including medical and socio-demographic factors.31,32 However, this study did not include patient factors. Second, the rate of HIE use in this study was low, especially in small hospitals and clinics, where it was below 10%. The present study only included HIE processed through health insurance claims. This limitation may have led to much loss of important information on HIE occurring at the outside of the boundary of national insurance system. Third, methodologically, this study has a cross-sectional study design. This means that the study can only provide associations between HIE and HCO covariates rather than determine the causality of HIE use, which remains a goal for future research. We expect that a future study could reflect all aforementioned limitations.
This study result indicates that healthcare policy makers should be aware of and pay more attention to the number of nurses in HCOs to promote and to accelerate HIE use. Providing nurses with educating and training HIE would be one of practical alternatives, and advertising governmental HIE programs through nurses or related associations would be another strategy. Ultimately, these approaches would result in significant improvement of health care quality in clinical settings.
Conclusion
This study has verified that there are several organizational factors associated with HIE use. Among them, the number of nurses was an important and dominant predictor of HIE use and the volume of HIE in all types of HCOs. The study verifies that the number of nurses is positively associated with HIE use and the volume of HIE use in all types of HCOs. The study result was based on large big and solid data using the entire national health insurance clams. The study findings can contribute to the knowledge expansion of health service research and medical informatics fields.
Footnotes
Acknowledgments
We deeply thank to Dr Christopher Lane, formerly Senior Lecturer in Linguistics, Victoria University of Wellington, New Zealand, and currently Senior Advisor, Analytics and Intelligence, Health Workforce Directorate, Ministry of Health, New Zealand for reviewing the manuscript and giving us excellent comments.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the HIRA Institutional Review Board on Feb 5, 2018 (Approval number, 2018-004-001).