
Abstract
To evaluate the current views on doctor–patient relationship (DPR) between citizens and medical staff in post-Corona Virus Disease 2019 (COVID-19) period and predict the possible factors of DPR, we distributed questionnaires by a online questionnaire platform--Questionnaire Star (https://www.wjx.cn) to evaluate DPR in post-COVID-19 period. Overall, 312 questionnaires for citizens and 421 questionnaires for medical staff were completed. Citizens felt that service attitude and communication with medical staff, and registering process have been improved. And their trust in doctors has increased by 86.8%. Majority of citizens (66.0%) preferred the tertiary hospitals. If doctor–patient contradictions occurred, 62.9% citizens preferred internal negotiation (with the doctor involved, 44.6%; with hospital management department, 18.3%). There was significant difference of views on the causes of medical violence incidents and the reasons for doctor–patient conflicts in the future between citizens and medical staff. The DPR score of medical staff was lower than citizens at each stage, and even showed a downward tendency in post-COVID-19 period. Furthermore, 20.4% medical staff believed that harmonious DPR would not be maintained, which was distinct from that of the citizens. Combating the COVID-19 provided an important opportunity to improve the DPR. However, unbalanced allocation of high-quality medical resources, gap between the actual treatment efficacy and patient’s expectation, fairness and efficiency issues, financial conflicts, and medical information symmetry were still the influencing factors of DPR.
What Do We Already Know About This Topic?
Doctor–patient trust is the cornerstone of the treatment relationship, which usually involves medical service quality, communication, and satisfaction; although a healthy and positive doctor–patient relationship is so crucial that can influence the healthcare quality and empower the patient to deal with their disease during a pandemic, the evidence suggests that doctor–patient trust level was insufficient in East Asia, including Mainland China, Japan, and South Korea.
How Does Your Research Contribute to the Field?
Findings suggest the following solutions maintain and consolidate a positive doctor–patient relationship in post-COVID-19 period: (1) improving the infrastructure and talents construction to strengthen support for primary medical institutions; (2) taking advantage of the medical development opportunities via the internet in the COVID-19 period, with the support of medical insurance reimbursement policy, to accelerate the development of programs including drug delivery service, artificial intelligence diagnosis or treatment, and health monitoring, thus improving the efficiency of diagnosis and treatment; (3) popularizing healthcare knowledge in order to match patients’ expectations with medical technical level, since the demand for healthcare knowledge by the citizens has been increased in the COVID-19 period; and (4) increasing positive medias' coverage to reflect that doctors and patients are not antagonistic, but a community of common destiny that fights diseases together.
What are Your Research Implications Toward Theory, Practice, or Policy?
High-quality medical resource allocation imbalance gap between actual efficacy and patient expectations, fairness and efficiency issues, financial conflict, and symmetrical medical information were identified as main factors that influence doctor–patient relationship in post-COVID-19 period. This research will help to solve medical disputes affecting the doctor–patient relationship, and to improve patient satisfaction. Doctor–patient contradictions that may occur in the future can be predicted, and the results can provide the basis for the formulation of strategies to promote a more healthy and positive doctor–patient relationship.
Introduction
The doctor–patient relationship (DPR) has been the cornerstone of medical practice to ensure normal medical process. Doctor–patient trust is the bedrock of the treatment relationship, which usually involves medical service quality, communication, and satisfaction. 1 Healthy and positive DPR is crucial because it can influence the healthcare quality and empower the patient to deal with their disease during a pandemic. 2 Patient’s treatment compliance, therapy outcome, and satisfaction with a healthcare procedure could also influence the DPR conversely.3-5 A gradual deterioration of DPR seems to be an inevitable trend for the healthcare system worldwide over time. Pun et al 6 reported insufficient doctor–patient trust level in East Asia, including Mainland China, Japan, and South Korea. Patients in China reported negative trust in doctors due to less doctor–patient communication and physician–patient shared decision-making. 7 Shared decision-making between the doctor and patient determines the most appropriate and best course of action for an individual patient. 7 In recent years, DPR hasdrastically deteriorated in China. 8 According to the White Paper on the Practice of Chinese Doctors published by the Chinese Medical Doctor Association in 2018, 66% of doctors experienced conflicts with patients, and more than 30% were treated violently.
Corona Virus Disease 2019 (COVID-19) was discovered in China in late December 2019. Because of its long incubation period, highly contagious nature, and various clinical features, 9 COVID-19 has a great impact on the already overburdened healthcare systems and human resources. Whether DPR has remained consistent in this unusual COVID-19 period remains largely unknown. Paul Farmer, an experienced medical anthropologist, highlighted the risk of exacerbation of global and social inequalities due to global health response in emergency conditions. 10 DPR seems harmonious during the COVID-19 pandemic; however, some doctor-patient relationship issues still occurred in China. At present, China has entered a period of normalized prevention and control of COVID-19, but whether the benign DPR will be maintained in post-COVID-19 period has become a debated topic in China11.. However, few research has studied the DPR in post-COVID-19 period.
It is important to understand the evolution of DPR during a pandemic from different objects. 12 The main objective of this study was to evaluate DPR focusing on two groups (medical staff and the patients). To evaluate DPR, the perspective of patient with specific diseases may be insufficient to represent the perspectives of all kinds of patients. Therefore, we obtained information from different perspectives of citizens instead in this research. Questionnaires were used to obtain information regarding the different views on DPR betweenmedical staff and citizens to predict doctor–patient contradictions that may occur in the future, provide strategies to improve the DPR and provide reference for the formulation of healthcare policies.
Methods
Study Design, Setting, and Data Source
Participants should: (1) have a mobile phone with an IP address in Chinese mainland; (2) be able to read and write Chinese; and (3) be voluntary to participate in this study. Participants have been excluded if: (1)the participant is illiterate; (2)same mobile phone IP address that has been filled by other persons is found and then is verified as one of other participants, for preventing one person to take the questionnaire more than twice; (3)the questionnaire is filled with all same choice, to avoid unprecise questionnaire,; and (4) the questionnaire is not filled in completely.
The study was approved by the ethics committee of Changzhou Maternity and Child Health Care Hospital, and informed consent was obtained from all the participants on the internet before the survey. This online survey was conducted in October 2020 for a month. We used convenience and snowball sampling strategies to recruit participants via a professional survey service—Questionnaire Star (https://www.wjx.cn) on WeChat, a social media app. Participants who were interested in this research clicked on the link to participate in the survey and to complete the questionnaire.
The questionnaire we used was a revised version of an original DPR scale,13-17 according to the actual survey needs. Different versions of questionnaire were prepared for citizens and medical staff. The questionnaires for citizens were distributed to patients, students, and staff of government organizations, enterprises, and public institutions. The questionnaires for medical staff were distributed by medical staff to their peers, colleagues, and classmates. Finally, 312 questionnaires for citizens and 421 questionnaires for medical staff were distributed and collected with 100% response rate.
In the questionnaire for citizens, there were 3 different evaluating aspects on DPR in post-COVID-19 period: (1) Medical services experiences: improvements, the level of trust in doctors, and the factors influcing their impressions on the hospital. (2) Personal assumptions: the way to choose a doctor when seeking medical treatment, the way to deal with doctor–patient conflicts, and the willingness of themselves or their relatives to engage in heathcare sector in the future. (3) Practices to increase trust between doctors and patients: the refreshed understanding of DPR in COVID-19 period, the role of social medias in influcing DPR, and factors that are urgently needed to be constructed and integrated in hospitals' culture.
There were 3 different views on DPR between citizens and medical staff in post-COVID-19 period: (1) Views on medical violence incidents. (2) Assumptions about the reasons for doctor–patient conflicts in the future. (3) Views on the persistence of doctor-patient trust and DPR score in COVID-19 period.
Statistical Analysis
The original data were exported using the “spv” file format from the online questionnaire platform--Questionnaire Star. Quantitative data, such as DPR score, are expressed as mean ± standard deviation (mean ± SD). T-test was used for comparison of means between the two groups. Qualitative data, such as gender and occupation, were expressed as constituent ratio/rate, and χ
Results
Basic Characteristics of the Study Subjects
The Distribution of Demographic Characteristics in this Study.
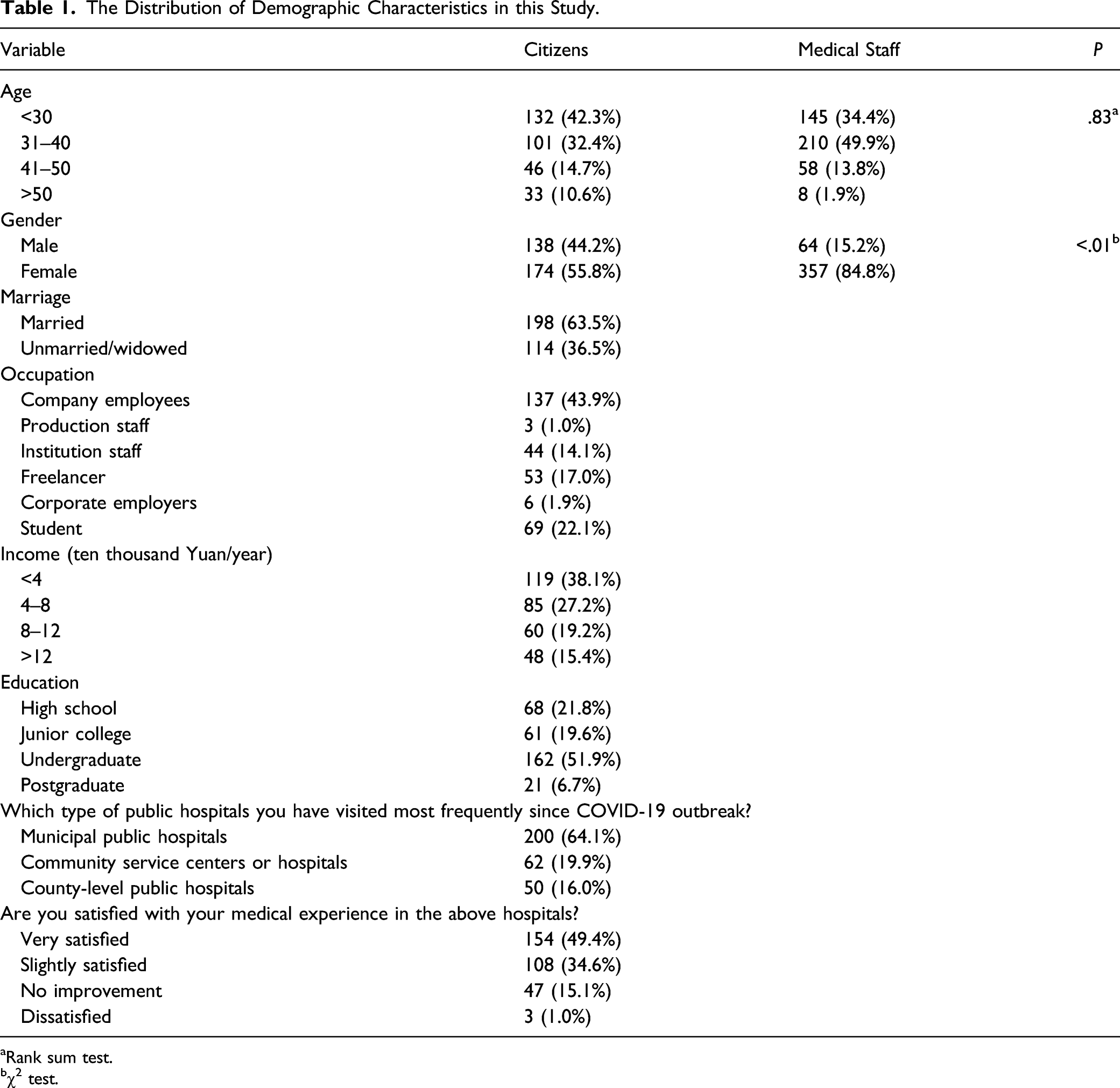
aRank sum test.
bχ2 test.
Medical Services Experiences of Citizens in Post-COVID-19 Period
Citizens' Views on DPR in Post-COVID-19 Period.

Citizens' Personal Assumptions on DPR in Post-COVID-19 Period
Majority of the citizens (50.6%) will directly register with an expert at a tertiary hospital when seeking medical treatment in their city, or directly contact a doctor through an acquaintance (20.8%). Assuming that doctor–patient contradictions will occur in the future, 62.9% citizens preferred internal negotiation involved with the doctor (44.6%) or with hospital management department (18.3%). Although the majority of citizens or their relatives would be willing to engage in heathcare sector in the future, 20.5% citizens selected slightly disagree or strongly disagree (Table 2).
Citizens' Views on Practices to Increase Trust Between Doctors and Patients in Post-COVID-19 Period
The outbreak of COVID-19 has contributed to better doctor–patient trust and lower violence toward doctors. 15 Based on the medical staff’s contributions in COVID-19 period, the view that medical staff’s job task is enormous and risky was recognized by 41.3% citizens, generally. Overall, 38.8% citizens believed that positive media reports about medical staff can improve their occupational image. In the citizens’ opinions, the spirit of unity and devotion were worth integrating into hospital culture (Table 2).
Differences in Views of Citizens and Medical Staff on the Causes of Medical Violence Incidents
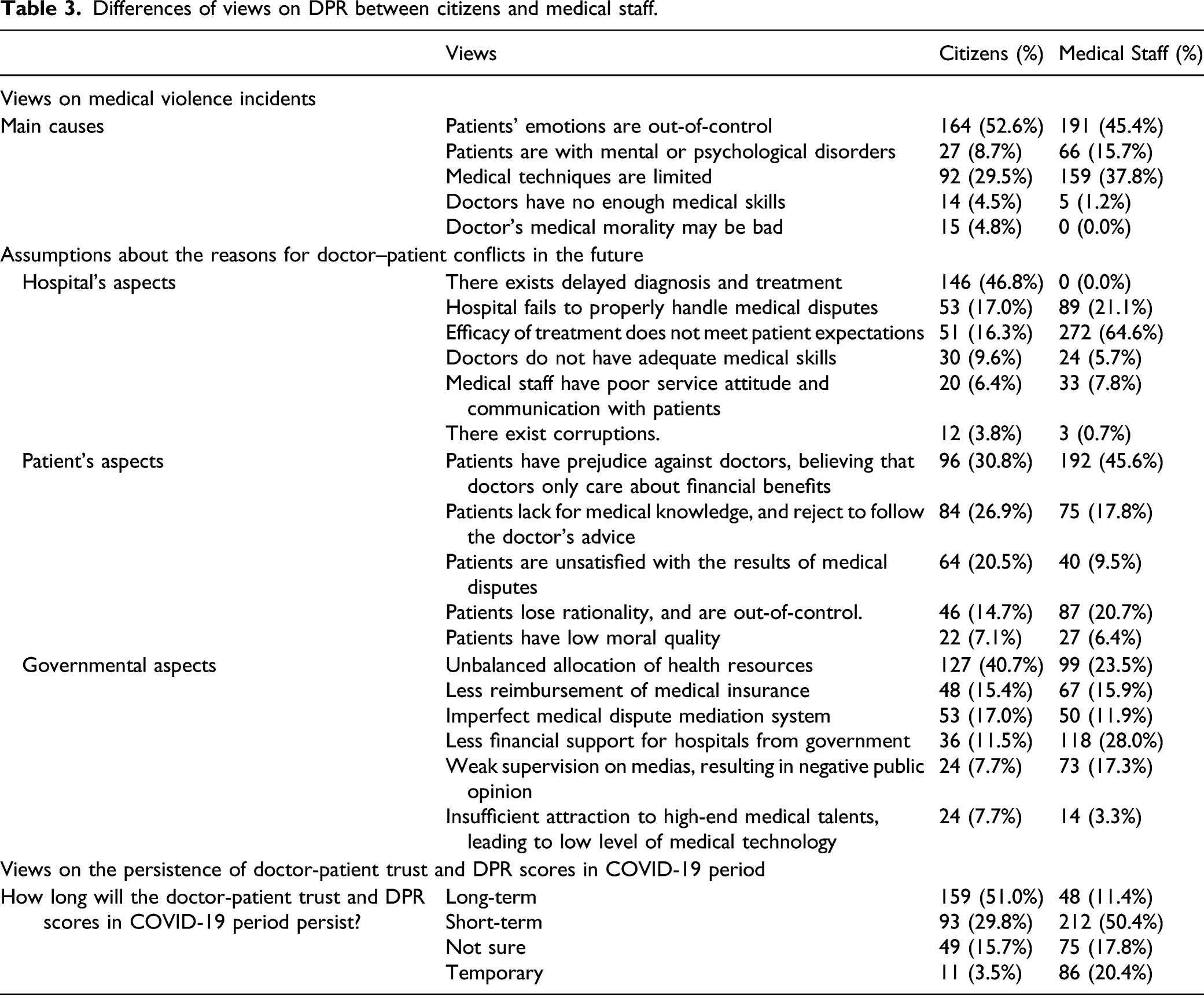
Differences of views on DPR between citizens and medical staff.
Differences of Views on the Reasons for Doctor–Patient Conflicts in Future between Citizens and Medical Staff in Post-COVID-19 Period
The views on the reasons for doctor–patient conflicts in the future between citizens and medical staff in post-COVID-19 period differed significantly in hospital, patient, and governmental aspects (P < .01) (Table 3). Towards the hospital's aspects, 46.8% citizens believed that the future doctor–patient conflicts were related to delayed diagnosis and treatment, while 64.6% medical staff believed that it was related to the efficacy of treatment which did not meet patient expectations. Towards the patient's aspects, the majority of citizens and medical staff (30.8% and 45.6%, respectively) believed that it was related to prejudice against doctors on financial interests. For the governmental aspects, 40.7% citizens believed it was related to unbalanced allocation of health resources, while 28.0% medical staff believed it was related to less financial support for hospitals by the government.
Scoring DPR Between Citizens and Medical Staff at Different Stages of COVID-19 Period
The DPR scorewas designed to be 0–10 points at three stages of COVID-19 period. The higher the score, the more harmonious DPR. Before the COVID-19 was discovered, the mean DPR score of citizens and medical staff was 7.80 ± 1.96 and 6.62 ± 1.97, respectively. During the pandemic stage, the score was 8.53 ± 1.67 and 7.69 ± 1.73, respectively. In the post-COVID-19 period, the score was 8.59 ± 1.57 and 7.30 ± 1.80, respectively. The DPR score of medical staff was lower than that of citizens at each stage and showed a downward trend in the post-COVID-19 period (Figure 1). DPR score of citizens and medical staff at different stages of COVID-19 period.
Differences of Views on the Persistence of Doctor-Patient Trust and DPR score in COVID-19 period.
There was significant difference of views on the persistence of doctor-patient trust and DPR score in COVID-19 period. (P < .001). Overall, 51.0% citizens had a positive attitude toward the fact that harmonious DPR would be maintained long-term, while more than half (50.4%) of medical staff believed that it would be maintained short-term. Surprisingly, 20.4% medical staff even believed that the harmonious DPR would be temporary, which is distinct from that of citizens (Table 3).
Discussion
Joint Fight Against COVID-19 can Improve DPR Significantly
Under the impact of the COVID-19 pandemic, the patients understood better the work of medical staff and improved the level of satisfaction of medical staff. 19 Various medias reported that medical staff’s job task was enormous and risky during the COVID-19 pandemic, and that DPR gradually became more harmonious. Among the citizens, 38.8% believed that media coverage enhanced the occupational image of medical staff. In the fight against the COVID-19 pandemic, China not only showed institutional advantages of coordinating all our efforts to complete key national undertakings, but also reflected the values of pursuing a community of common destiny. Therefore, 36.5% citizens hoped to integrate the spirit of unity into hospital culture.
The score of DPR in post-COVID-19 period was higher than that during COVID-19 pandemic period. Nearly half of the citizens had positive and optimistic attitude toward the long-term maintenance of harmonious DPR. However, Gao et al reported that it is difficult to improve the current DPR situation in China, within a short-term period, even with the impact of COVID-19. 20 Free medical treatment of COVID-19 patients in China eliminated the economical contradiction between doctors and patients. The most improved aspect in the post-COVID-19 period, according to the citizens, was improved service attitude and communication wtih medical staff.”
The COVID-19 is an important opportunity for improving DPR. Similarly, the majority of citizens believed that DPR was improved when against Severe Acute Respiratory Syndrome (SARS). In the post-COVID-19 period, the DPR score of citizens was still slightly increased, while that of the medical staff was decreased. This contrast reflects the obvious lack of confidence of medical staff in the long-term maintenance of harmonious DPR. Whether DPR is harmonious in the post-COVID-19 period is worthy of further study, the same as it did in post-SARS period.
Balanced Allocation of High-Quality Medical Resource can Promote the Long-Term Development of DPR
In this study, 66.0% citizens chose tertiary hospitals for medical treatment. Only 1.6% citizens gave priority to the nearby community health service center, indicating citizen’s distrust of primary medical institutions. Studies have shown that during the COVID-19 outbreak, citizens showed anxiety and panic. 21 In China, citizens often overcome their fear by choosing tertiary hospitals for treatment when they are sick. Both citizens and medical staff believed that primary medical institutions lack high-quality medical resources. Many citizens subconsciously reputed that there are fewer facilities, experts, and experience in disease management in primary medical institutions. Our study found that both citizens and medical staff believed that reducing the financial pressure of patients on medical treatment is an important factor to effectively alleviate the doctor–patient contradiction. Perhaps increasing the proportion of medical insurance reimbursement could improve the willingness of patients to choose primary medical institutions.
The Gap Between the Actual Treatment Efficacy and Patient’s Expectation May Induce Conflicts Between Doctors and Patients
In recent years, with a “fast culture” trend, the society began to pursue a fast-paced lifestyle. Citizens believed that the main cause for doctor–patient conflicts in post-COVID-19 period is delayed diagnosis and treatment. However, none of the medical staff selected this.
The essence of enhanced sensitivity of time by patients is patients' strong expectations for alleviating pain and recovery from diseases. Patients are more sensitive to the waiting time before receiving treatment, especially for those patients with anxiety and negative but irritable emotions. Due to the difficulty in balancing medical equity and efficiency, to increase doctor–patient communication, improve service attitude, and streamline medical treatment processes can moderately improve mental state of patients, thus reducing doctor–patient disputes. It is suggested that more time should be spent in listening to the patients, which is a way of caring for the patients during COVID-19 pandemic. 22 The proportion of medical staff realizing the limitations of medical techniques is obviously higher than that of the citizens. Medical staff are the practitioners and witnesses of medical technology. They have a better understanding of the current level of medical technology and the extent to which they can treat diseases. In fact, some patients often hope to see the effect of treatment immediately after being treated. The gap between the patient’s expectations of the treatment and the actual effect has become an important reason for the contradiction between doctors and patients.
Financial Conflicts Can Induce the Contradiction Between Doctors and Patients
Some medical violence incidents have occured accidentally in China since the COVID-19 was discovered. To resolve doctor–patient conflicts and violence, short-term and high-intensitive positive publicity during the COVID-19 pandemic period is not enough to eliminate violence. Affected by negative opinion of the public, doctors treat current DPR more pessimistically than patients and tend to adopt defensive medical behavior.
There exist financial contradictions between doctors and patients. As we know, medical service satisfaction plays a positive role in trust of doctors and patients. 23 It is impossible to know whether the patient is satisfied with the doctor’s treatment strategy before the treatment has been completed by the patient. Medical services and doctor ethics are involved in the whole therapy process of patients’ perception, which leads to the association of therapeutic effect with medical services and doctor ethics. In addition, majority of both citizens and medical staff believed that prejudice against the doctors on financial interests is a main cause of doctor–patient conflicts in the future. Furthermore, patients will consider the overall medical fee, treatment time, rehabilitation time, and other factors to evaluate treatment efficiency. Some irrational patients may use violence to compensate their loss offinancial interests.
The Asymmetry of Medical Information Between Doctors and Patients May Exacerbate Patients’ Mistrust
During the COVID-19 pandemic period, citizens’ initiative to acquire healthcare knowledge and spontaneous communication has been improved significantly. In addition, the high frequency and full coverage of health science popularization significantly enhanced the citizens’ awareness of epidemic prevention and medical knowledge reserve, which played a promoting role in winning citizens' support for medical treatment. In the past, the contents of medias' report on public hospitals were simple: mostly the dissemination of healthcare knowledge and introduce successful treatment experience. At this time, the patient is in a passive state of acceptance. Only the specific patients care the specific healthcare knowledge. The amount of knowledge is not fully balanced between the needs of patients and the supply of communicators (doctors). The degree of consensus on treatment between doctors and patients will determine the effectiveness of treatment, especially for patients requiring long-term treatment.
According to the experience and social benefits of healthcare knowledge dissemination during the COVID-19 pandemic period, the effectiveness of doctor–patient communication should be considered in speeding up the establishment of medical information symmetry between doctors and patients. 24 In order to meet the patient’s needs, the healthcare knowledge dissemination should not be restricted to traditional media such as TV, newspaper, and radio. It also can be spread through short videos in smartphone apps such as TikTok and WeChat. Effective doctor–patient communication is essential to establish benign DPR. However, many doctors erroneously consider that they already have good communication skills with patients. 25 Recently, in order to promote healthcare knowledge dissemination for citizens, some hospital has taken it into the assessment of daily medical work and professional title for medical staff.
Conclusion
The COVID-19 pandemic is an important opportunity for improving DPR. However, unbalanced allocation of high-quality medical resources, gap between the actual treatment efficacy and patient’s expectation, financial conflicts, and medical information asymmetry are still the influencing factors of DPR. Overall, there are four aspects to maintain and consolidate the benign DPR in post-COVID-19 period: (1) improving the infrastructure and talents construction to strengthen support for primary medical institutions; (2) taking advantage of the medical development opportunities via the internet in the COVID-19 period, with the support of medical insurance reimbursement policy, to accelerate the development of programs including drug delivery service, artificial intelligence diagnosis or treatment, and health monitoring, thus improving the efficiency of diagnosis and treatment; (3) popularizing healthcare knowledge in order to match patients’ expectations with medical technical level, since the demand for healthcare knowledge by the citizens has been increased in the COVID-19 period; and (4) increasing positive medias' coverage to reflect that doctors and patients are not antagonistic, but a community of common destiny that fights diseases together.
Footnotes
Acknowledgments
*This research is an outcome of the doctoral thesis of the corresponding author, undertaken at the Doctor of Management in Healthcare Program jointly held by ISCTE University Institute of Lisbon (Iscte), Portugal, and Southern Medical University (SMU), P. R. China. We would like to express our gratitude to Ms. Yongyi Jiang from Southern Medical University, who has paid great contributions to our study as one of the team members. She is responsible for proofreading to ensure that the paper meets international standards for publication, and has improved the readability of this paper. Thanks again for her great help.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by the special project of soft science research of Changzhou science and technology association in 2020, Jiangsu maternal and child health research project (F202052), and the open project of biological resources sample bank of major diseases in Jiangsu province in 2020 (SBK202007002).