
Abstract
Background
College students are vulnerable and may experience high stress due to COVID-19, especially girls. This study aims to identify posttraumatic stress disorder (PTSD) and related factors among the target population during the initial phases of the COVID-19 pandemic.
Methods
In the initial phase of COVID-19 epidemic (February 23 to March 5, 2020), 2205 female college students from six provinces in mainland China were enrolled in this study and completed the online survey about the cognitive status of COVID-19, including the Impact of Event Scale-6, the Multidimensional Perceived Social Support Scale and a self-developed 10-item Perceived threat scale. Univariate and multivariate logistic regression were performed using SPSS software to explore the determinants of PTSD symptoms.
Results
PTSD symptoms were prevalent in female college students, and 34.20% met the cut-off for PTSD. Self-reported fair or poor health (AOR = 1.78, 95% CI: 1.22-2.59), high concern about COVID-19 (AOR = 1.66, 95% CI: 1.35-2.03), beliefs that “COVID-19 can cause a global outbreak” (AOR = 1.26, 95% CI: 1.02-1.56), the perception of “risk of infection” (AOR = 2.46, 95% CI: 2.16–2.81), beliefs that “closed management” and “COVID-19 as a public health emergency of international concern” would have an impact, and the fear of “impact on life planning” were all positively associated with PTSD (AOR = 1.37, 1.22, and 1.29, respectively); however, perceived social support from family (AOR = 0.81, 95% CI: 0.70-0.93) was negatively associated with PTSD. Among the significant variables at the bivariate level, multivariate logistic regression revealed that the greatest protector for PTSD was the high knowledge score (AOR = 0.73, 95% CI: 0.60–0.90), while had confirmed cases among relatives and friends (AOR = 7.70, 95% CI: 1.28-46.25) was the strongest predictor of PTSD.
Conclusions
In summary, PTSD symptoms were prevalent among female college students in China during the COVID-19 epidemic. Targeting vulnerable populations to improve their knowledge about COVID-19 and create an atmosphere of social support would be beneficial. Moreover, the joint efforts from family, school administrators, and policymakers are essential to improve the mental health of the female students during the COVID-19 epidemic.
Highlights
Background
The coronavirus disease 19 (COVID-19) infection began in December 2019 and, as of May 2, 2021 has resulted in 151 812 556 cases and 3 186 817 deaths worldwide. 2 In China alone, there were 103 667 reported cases and 4858 deaths due to COVID-19. 3 Given the serious situation, the World Health Organization (WHO) declared COVID-19 a Public Health Emergency of International Concern (PHEIC) on January 30, 2020 and due to the unprecedented spread of the virus, it was declared as a global pandemic on March 11, 2020. 4 Since the beginning of the outbreak many countries have adopted strict measures to control the outbreak, including nationwide lockdown, home isolation, quarantine, and social distancing.
The COVID-19 pandemic has caused an enormous psychological impact among all kinds of the population worldwide.5–7 Globally, relatively high rates of posttraumatic stress disorder (PTSD) (7%–53.8%) symptoms were reported in the general population during the COVID-19 pandemic, especially in college students.1,7–10 Exposure to such stressful events can lead to acute stress disorder and persistent symptoms leading to PTSD. At the end of February, college students in China were notified about the postponement of schools. They could not resume school like normal days, and their regular routines of the study were disrupted. Meanwhile, they were youths who developed self-discipline and emotional control and thus easily prone to such stress. 11 In a study among college students in mainland China during the beginning of COVID-19 outbreak, 30.8% (95% CI: 28.8–32.8%) of the participants who completed the survey presented clinically relevant PTSD symptoms. 1
Females are usually more likely to have mental health problems than males when under the stressful events.12,13 Due to sex hormones (estradiol and progesterone) and the life trajectory they experience, females are always worried about interpersonal stressors, gender-based violence, lack of gender equality, and discrimination compare to the similar-age male.12,13 A previous study showed that the home isolation due to COVID-19 was associated with a worse psychological status with a stronger association in women compared to men. 14 PTSD is one of the most prevalent long-term psychiatric disorders for females while facing traumatic events.15–17 Previous studies indicated that acute psychological disorders and PTSD symptoms are more prevalent in females than males after traumatic events.18–20 A study conducted in South Lebanon revealed that females have twice the prevalence of PTSD as males after experienced the 2006 war (24.3 vs 10.4%). 19 Similarly, among Indian females and males affected by flash floods in 2010, 22.3% and 18.1% met the diagnostic criteria for PTSD, respectively. 20
Given the dispositional traits of females and influences of COVID-19 on university students, this study aims to focus on female college students and identify the PTSD symptoms and related factors of this vulnerable group during the initial phases of COVID-19 pandemic through a multicenter study. The results of this study may assist government and health care agencies in developing interventions by understanding the causes of adverse psychological outcomes to alleviate stress in college students, especially for female students in the event of future outbreaks, infectious diseases, or disasters.
Methods
Settings and Participants
We conducted a cross-sectional survey from February 23 to March 5, 2020 in various provinces of mainland China, when the COVID-19 outbreak new cases showed a downward trend in China and an upward trend overseas. Due to the isolation and social distancing measures recommended by the Chinese government, the questionnaire survey and corresponding data were distributed and collected electronically via the internet. In mainland China, potential participants from six universities (University of Jinan, Sichuan University, Sun Yat-sen University, Shanxi University of Chinese Medicine, Henan University of Engineering and Dalian University of Technology) are located in different geographical areas territories were electronically invited by partner teachers in each university. Moreover, the participants have to meet the following criteria: (1) college female students; (2) aged ≥18 years; and (3) proficiency in Chinese. After meeting the inclusion criteria and providing electronic informed consents, they were directed to complete the self-reported questionnaire.
During the study period, in addition to staying at home compulsorily rather than returning to school, participants living in different areas would be required to strictly follow local prevention and control policies. According to the epidemic risk level, mainland China has divided coping strategies into the following three categories: (1) In low-risk areas, the strategy is to “strictly prevent importation,” (2) in middle-risk areas, the strategy is “to prevent the importation and stop transmission internally,” and (3) in high-risk areas, the strategy is “to stop transmission internally, prevent exportation and implement strict prevention and control measures.”
Measurements
The structured questionnaire was designed to encompass the following areas: (1) demographic characteristics such as age, major, and health status, (2) variables related to COVID-19 (e.g., awareness of COVID-19, levels of concern to the outbreak), (3) daily perceived social support, (4) perceived threat associated with COVID-19, (5) PTSD. PTSD, perceived threat, and perceived social support were measured as outlined in the following.
Impact of Event Scale-6
The Impact of Event Scale-6 (IES-6) is an abbreviated 6-item version of The Impact of Event Scale-revised, which has been widely accepted as a core outcome measure for PTSD in critical illness survivorship research.21,22 Respondents are asked to report the psychological impact after exposure to a crisis situation within 7 days of exposure using a 5-point Likert scale (0 = not at all; 4 = extremely), and PTSD is measured when the score of IES-6 is greater than or equal to 10. 21 In the present study, the Cronbach’s α was 0.84.
The Perceived Threat Scale
To measure the extent of threat to which participants perceived from COVID-19 pandemic, the 10-Item perceived threat scale was developed. The items were based on earlier studies,23–25 each item can be rated on a scale from 1 (Strongly disagree) to 5 (Strongly agree). Exploratory factor analysis on the 10 items of perceived threat yielded 3 dimensions: risk of infection, impact on life planning, and impact of PHEIC. The three dimensions of the perceived threat scale were proved to have satisfied content and concurrent validity. Sample items includes: “I feel anxious and scared when thinking of COVID-19.” In the present study, the Cronbach’s α for the three dimensions were 0.83, 0.84, and 0.88, respectively (See Appendixes A1 and A2).
The Multidimensional Scale of Perceived Social Support (MSPSS)
The 12-item perceived social support scale (MSPSS) assesses a respondent’s perceived support on a 7-point Likert scale (1 = strongly disagree; 7 = strongly agree). 26 Total possible scores range from 12 to 84, with higher scores indicating higher levels of perceived support obtained from family, friends and significant others. The Chinese version of the MSPSS has adequate internal consistency in earlier study and in present study (Cronbach’s α = 0.89 and 0.94, respectively). 27 The Cronbach’s α for family, friends and significant others were 0.88, 0.92 and 0.87, respectively.
Statistical Analysis
The data were analyzed using SPSS 23.0. A descriptive analysis of the demographic data was conducted to describe the sample characteristics. Categorical variables were expressed as frequencies and percent distributions, while continuous variables were presented as means ± standard deviations (SD). The prevalence of PTSD was derived according to the cut-off values routinely used in previous studies. Bivariate generalized linear modeling with a binary logistic distribution was conducted to examine background and other variables related to PTSD. Variables that were significant at the bivariate level (P < 0.1) were adjusted in further multivariate analysis for factors related to PTSD. A value of P < 0.05 was considered statistically significant in multivariate analysis. The results were reported as odds ratios (ORs) and adjusted odds ratios (AORs).
Results
Background Characteristics
A total of 2205 individuals participated in the questionnaire survey with a mean age of 20.85 years (SD, 1.50 years; range, 18–26 years). Among participants, 96.78% were Han Chinese, 60.09% were rural residents, 45.90% were majored in medicine, 1.86% ever had at least one of the chronic diseases (e.g., diabetes, cardiovascular diseases), and 93.15% reported they have good health status. The mean score of perceived support from family, friends, and significant others was 5.65, 5.60, and 5.49, respectively.
Background Characteristics of Female College Students (N = 2205).

Knowledge, Awareness and Perceived Threat of COVID-19 Pandemic
Knowledge About COVID-19 and the Correct Rate of Participants (N = 2205).

*Multiple choice questions with incomplete and complete correct rate; Mean knowledge score: 10.58 ± 1.30 (range, 4-14; median, 11).
Knowledge, awareness and the perceived threat of COVID-19 pandemic among female college students (N = 2205).
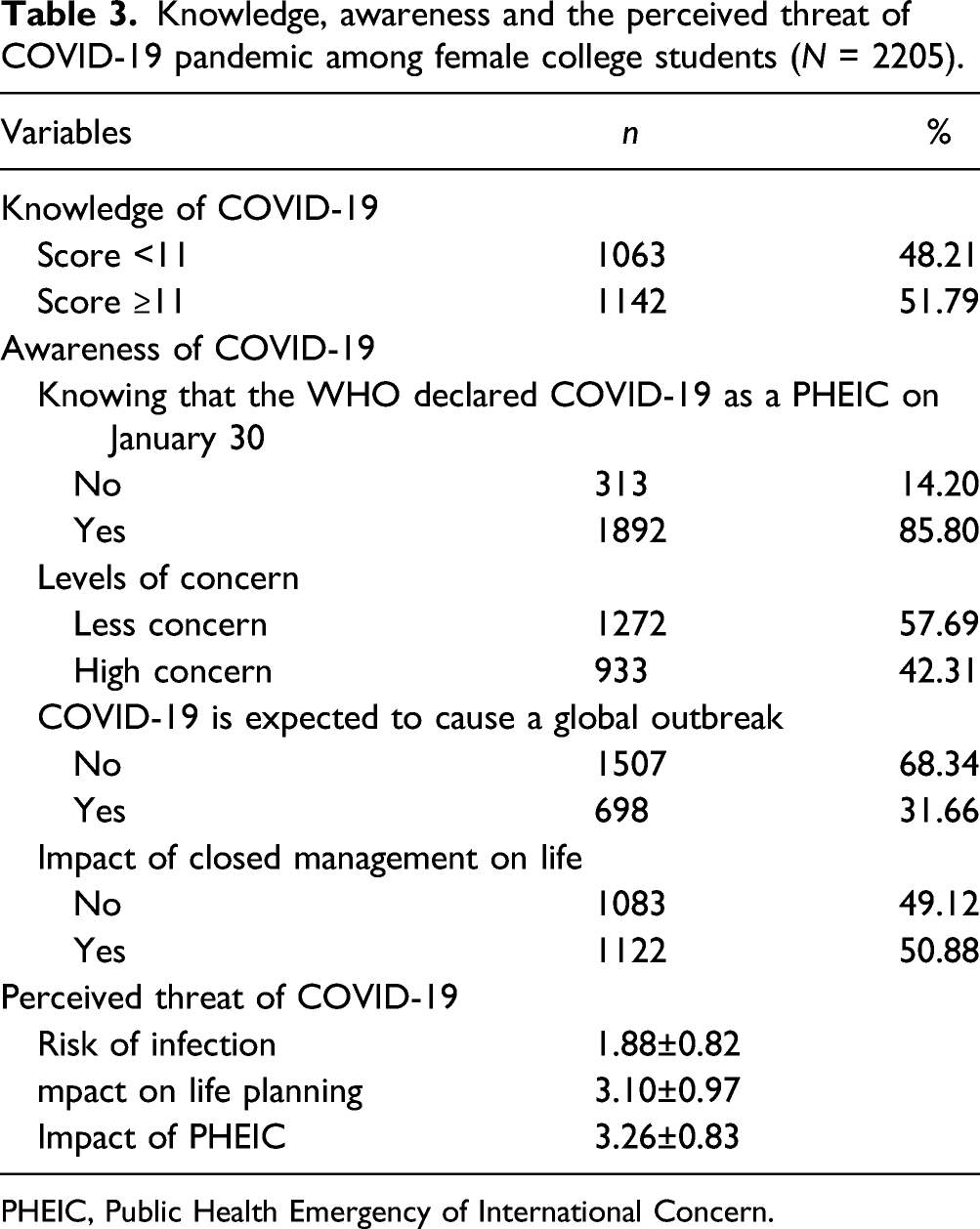
PHEIC, Public Health Emergency of International Concern.
Bivariate Correlates of PTSD
In the present study, the IES-6 scale was used to measure the PTSD of COVID-19 outbreak, which revealed a sample mean score of 7.42 (SD = 4.87), and 732 (34.20%) of participants were considered to have the PTSD symptom.
Bivariate correlation of background, knowledge, awareness, and perceived threat predicting PTSD (N = 2205).

OR: odds ratio; CI: confidence interval;
*P < 0.1
**P < 0.05.
Multivariate Correlates of PTSD
Multivariate predictors of PTSD during the epidemic (N = 2205).

AOR: adjusted odds ratio; CI: confidence interval;
**P < 0.05.
High concern about COVID-19, beliefs that “COVID-19 can cause a global outbreak” (AOR = 1.66, P = 0.00) and “impact of closed management on life” (AOR = 1.26, P = 0.03) were positively associated with PTSD. Concerns that “risk of infection,” “impact on life planning” and “impact of PHEIC” were all positively associated with PTSD (AOR = 2.46, 1.29 and 1.22, P = 0.00). Major in school, ever been quarantined or isolated and had close relatives and friends in key epidemic areas were not related to PTSD at the multivariate level.
Discussion
The findings of this study highlighted the major psychological challenges faced by Chinese college girls during the initial phase of the COVID-19 pandemic. Compared to the similar domestic and overseas studies, the prevalence of PTSD symptoms in this study was relatively high; nearly one-third of participants met the cut-off for PTSD.1,10,28,29 This might be partly due to the timing of the study, which was carried out at the initial phase of the COVID-19 outbreak. At that time, the overall understanding of the disease, and the corresponding measures of prevention and control of the epidemic was still in infancy. Moreover, during the study period, the COVID-19 outbreak escalated to a global pandemic and got serious. Thus, the prevention, control measures, and the growing pandemic trend may cause a general panic. 4 Furthermore, the international influence of the COVID-19 pandemic and its impact on people’s lives is unprecedented; hence, the short-term response of females is so overwhelming as they were likely to develop ASD, and eventually PTSD symptoms if it persists for a period of time.
Previous evidence suggested that females were more prone to PTSD than males.12,13,30,31 Under sudden or uncertain events, men have more activation in the inferior parietal lobule, while women have more activation in the postcentral gyrus. 30 The activation of different parts of the brain may explain why women are more likely to panic and limit their ability to act seriously than men who usually can control their emotions quickly and think about how to respond to the event, indicating that women are more likely to fall into a vicious cycle of acute emergency disorder that eventually develop into PTSD. 30 In addition, female sex hormones such as estradiol and progesterone play an important role in regulating mood states, and sex hormonal fluctuations caused by menstruation or severe stressful experiences could result in gender differences in PTSD susceptibility.12,13 Furthermore, due to gender differences in traditional culture and social roles, females always worry about interpersonal stressors, gender-based violence, lack of gender equality, and even discrimination compare to the similar-age male, making females more likely to suffer from anxiety, depression, PTSD, and other mental disorders. 31 Suffering from PTSD will undoubtedly affect female college students’ physical and mental health, academic performance, and work plan, and even their future lives. Therefore, identifying risk factors at the beginning of the epidemic, offer targeted psychological counseling, provide appropriate psychological support and theory-based interventions during the rehabilitation process are crucial.
People with moderate or bad health are not only susceptible to the COVID-19 infection (especially with the lack of proper protection) but also have a poor prognosis once diagnosed. The study results are in line with the previous study that PTSD symptoms are remarkably high among those who perceived themselves as not very healthy. 32 During the closed-off period, unhealthy participants might seek medical treatment or other health services; however, it may become a little difficult due to the traffic control and shortage of medical care in this extraordinary situation.33,34 Due to the absence of medical care and medical supply during the epidemic, these unhealthy populations were at an increased risk of PTSD symptoms.35,36 Therefore, in the COVID-19 pandemic, health officials should carefully weigh risks and benefits when planning the medical needs of vulnerable populations and chronic patients during the containment period. Basic medical services for these people should be ensured and relieve their mental stress to avoid the extra burden of other diseases apart from the epidemic.
In the current study, most of the respondents had high levels of social support, and the support from family, but not from partners or peers was negatively associated with PTSD symptoms, the same trend was observed among U.S. young adults during the COVID-19 pandemic. 28 College students were in-home quarantine during the study period. Substant support and security might be important in maintaining the mental health of young adults because many of them face acute stress and broken rhythms of life, such as holiday extension, financial pressure, graduation issues, and unemployment. Emotional support coupled with material security provided by the family would be an important factor in protecting them against PTSD. Besides, the unique social position of college students may also be a protective factor for PTSD. The government and universities have issued a series of measures to ensure the normal routines of students' study at home, the graduation and employment needs of students in their last academic year. 37 Therefore, apart from supporting policy measures, family support should be addressed in the whole society to guarantee the psychological wellbeing of female college students during the COVID-19 pandemic.
Consistent with the González-Sanguino C’s study, 17 our results revealed that those who had confirmed cases among relatives and friends were prone to have PTSD symptoms, which was one of the strongest predictors of adverse psychological impacts during the COVID-19 pandemic. When something stressful and terrifying happens around them, they may feel frightened and helpless since they are positively affected by the event.38,39 Therefore, they are likely to go into the “crisis phase,” characterized by crying, stress, insomnia, and nightmares, and eventually develop symptoms of PTSD if symptoms persist.40,41 This suggests that we should identify and focus on female college students who have COVID-19 patients among close relatives and friends, guide them to adjust their mental health, divert attention, and provide social support to encourage them to re-plan their lives under existing conditions. 42
Another protective factor for PTSD symptoms found from this study is a high level of knowledge on COVID-19. With easy access to the internet, most respondents can get instant updates on news related to the COVID-19 outbreak, and the role of information seemed to be fundamental to cope with the epidemic mentally and physically. A negative relationship between sufficient knowledge and adverse psychological impact of the pandemic is also found in other studies.15,16,43 However, it should be cautious on the infodemic.44,45 Social platforms play an important role in information acquisition and dissemination during the epidemic. Though the information from various sources and platforms is updated in real-time, it lacks quality control. This suggests that the learning ability and experience of female college students to identify false or valid information may be a potential protective factor for PTSD. When we are surrounded by information, which may have to affect our emotions and behavior, such as the looting of Shuanghuanglian in the initial phase of the epidemic in China, worries, fear and panic-driven by false information may cause people to develop PTSD symptoms. Therefore, it is critical to ensure that upto-date, accurate and scientific information can be obtained from reliable sources to avoid panic caused by insufficient and inaccurate information and knowledge.
Additionally, our self-developed COVID-19 related perceived threat scale uniquely predicted PTSD symptoms among young females, underscoring how the specific features of this pandemic give rise to acute and posttraumatic stress. Participants were not only worried about accidentally getting infected by COVID-19 but also worried that their work and life arrangements would be affected by the continuity of the epidemic. Long-term accumulation of adverse emotions would finally result in PTSD symptoms, including intrusion, avoidance and hyperarousal if symptoms persist.32,41 There is an urgent need to explore the mechanisms behind their potential PTSD symptoms and formulate specific interventions accordingly. First, the official media, schools and teachers should strengthen the publicity of preventive measures to reduce their perceived infection risks. Second, the network structure of online teaching and job recruitment should be improved to alleviate the target population’s concerns about future plans, and ensure their normal paces of study and work. Finally, the government should show confidence to the public in coping with the economic downturn due to the pandemic and provide appropriate subsidies to minimize the impact of the epidemic on individuals, such as measures adopted by the UK and Australia.46,47
In summary, this study provides a basis for implementing measures to improve the mental health among female college students during the COVID-19 outbreak and has a reference value for identifying students who may have a high risk of adverse psychological problems. Our study has many strengths, including large sample size and robust statistical analysis. Additionally, to verify the relationship between knowledge of COVID-19 and PTSD, we have designed a 14-item COVID-19-related knowledge and behavior questionnaire, including basic information about COVID-19, main symptoms, routes of transmission, and health behaviors to deal with COVID-19 infection. Our results demonstrated that high-level knowledge about COVID-19 is of most importance in protecting against PTSD among female college students. Finally, considering the characteristics of female college students, we have developed the 10-item perceived threat scale with three dimensions, and its validity has also been confirmed in this research.
Limitations
There are several limitations to this study. First, the generalizability of our conclusions is impacted, given the results were possibly due in part to the nonrandom selection of the sample, the possibility of sampling bias should be considered. In addition, the uncontrolled online observational study of college students and the cross-sectional nature of the data warrant further longitudinal studies to determine the predictors of PTSD symptoms during the COVID-19 outbreak. Furthermore, the different psychological scales used in this study may lead to different measurement outcomes compare to previous similar studies. Finally, this study relied on anonymous network responses and self-reported answers regarding experience during home-quarantine stay, which may not align with clinical psychological diagnosis.
Conclusions
During the initial phase of the COVID-19 pandemic (February 23 to March 5, 2020), this observational cross-sectional study revealed that more than one-third of participants suffered from PTSD symptoms. Identifying high-risk individuals who are vulnerable to PTSD, improving their understanding of COVID-19, and providing a socially supportive atmosphere would be beneficial to maintain and promote the mental health of female college students during the COVID-19 epidemic. Therefore, the joint efforts from family, school administrators, and policymakers are imperative to maintain the psychological well-being of the female college students under the circumstances of public health emergencies.
Footnotes
Author Note
This research was supported by Chinese Academy of Medical Sciences and National Health Commission of the People’s Republic of China
Authors' contributions
Xiao-You Su, Ming-Yu Si prepared the first draft. You-Lin Qiao provided overall guidance. You-Lin Qiao, Xiao-You Su, Wen-Jun Wang and Ming-Yu Si managed the overall project. Xiao-You Su, Wen-Jun Wang, Xiao-Fen Gu, Li Ma, Jing Li, Shao-Kai Zhang and Ze-Fang Ren were responsible for the questionnaire survey of people in seven geographical regions of China. Xiao-You Su and Ming-Yu Si analyzed data. Yu Jiang and Yuan-Li Liu finalized the manuscript on the basis of comments from other authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Asian Regional Special Cooperation Fund of National Health Commission of the People’s Republic of China (BLXM01) and Innovation Fund for Medical Sciences sponsored by Chinese Academy of Medical Sciences (2020-I2M-2-015, 2019-I2M-2-005).
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Jining Medical University of Shandong Province on February 12th, 2020, right before the initiation of the study (approval number: JNMC-2020-KY-001). After passing the qualification review and voluntarily providing the electronic informed consent, potential participants were directed to complete the self-reported questionnaire.
Data Availability
The original data generated from this study and the analyzed results will be available from the corresponding author upon reasonable request
Appendix A
Factor loading of perceived threat items among college students (N = 2205).

| Perceived threat (items) | N (%) | Factor1 |
Factor2 |
Factor3 |
|---|---|---|---|---|
| I feel anxious and scared when thinking of COVID-19 | 209 (9.48) | 0.14 | 0.07 | 0.85 |
| I feel that I can be infected by the virus anytime and anywhere | 233 (10.57) | 0.09 | 0.07 | 0.88 |
| Worried about being infected and sick | 202 (9.16) | 0.07 | 0.03 | 0.84 |
| Worried that the epidemic will affect my study plan | 1525 (69.16) | 0.84 | 0.10 | 0.04 |
| Worried that the epidemic will affect my test plan | 1334 (60.50) | 0.88 | 0.12 | 0.05 |
| Worried that the epidemic will affect my social plan | 794 (36.01) | 0.67 | 0.11 | 0.15 |
| Worried that the epidemic will affect my work plan | 1196 (54.24) | 0.86 | 0.14 | 0.11 |
| Worried about the closure of tourism and/or trade, affecting international cooperation and exchanges | 1186 (53.79) | 0.12 | 0.88 | 0.05 |
| Worried about the lack of goods due to the interruption of import and export logistics | 1122 (50.88) | 0.12 | 0.92 | 0.06 |
| Worried about rising prices and rising exchange rates | 1209 (54.83) | 0.16 | 0.86 | 0.07 |
| Eigenvalue | 3.65 | 1.97 | 1.79 | |
| Cumulative % of variance explained | 36.46% | 56.18% | 74.06% | |
| Cronbach’s alpha | 0.84 | 0.88 | 0.83 |
Exploratory factor analysis, using principle component analysis for factor extraction (with varimax rotation). Factor 1–3 addressed threat due to pandemic impact and perceived risk (KMO = 0.77).
Appendix B
Pearson correlation between perceived threat and DASS-21 scale (N = 2205).

| Variables | Depression | Anxiety | Stress | |||
|---|---|---|---|---|---|---|
| β (95% CI) | P | β (95% CI) | P | β (95% CI) | P | |
| Perceived threat | 1.30 (1.11, 1.49) | 0.000 | 1.15 (1.00, 1.30) | 0.000 | 1.65 (1.46, 1.85) | 0.000 |
| Risk of infection | 1.01 (0.87, 1.14) | 0.000 | 0.98 (0.88, 1.09) | 0.000 | 1.30 (1.16, 1.44) | 0.000 |
| Impact on life planning | 0.53 (0.41, 0.66) | 0.000 | 0.43 (0.32, 0.52) | 0.000 | 0.65 (0.52, 0.78) | 0.000 |
| Impact of PHEIC | 0.45 (0.30, 0.60) | 0.000 | 0.37 (0.25, 0.49) | 0.000 | 0.59 (0.43, 0.75) | 0.000 |
The Chinese brief version of the Depression, Anxiety, and Stress Scale (DASS-21) consists of three subscales (each with 7 items) measuring depression, anxiety, and stress, and higher scores denote a greater severity of psychological symptoms. The DASS-21 has been validated in Chinese populations and the Cronbach’s alpha of 0.83, 0.80, and 0.82 for the Depression, Anxiety, and Stress subscales, respectively, and 0.92 for the total DASS [1, 2]. Taking the DASS-21 scale as a reference, the perceived risk and its three dimensions obtained in this study are all positively related to it, which further determines the content and validity of the perceived threat.
1. Wang K, Shi HS, Geng FL, et al. Cross-cultural validation of the Depression Anxiety Stress Scale-21 in China. Psychol Assess. 2016 May; 28 (5):e88-e100. Doi: 10.1037/pas0000207. 2. Lovibond PF, Lovibond SH. The structure of negative emotional states: comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav Res Ther. 1995 Mar; 33 (3):335-343. doi: 10.1016/0005-7967 (94)00075-u.